I nuovi farmaci antidiabetici e l'anziano - Renato Turco Seminari del Venerdì - grg-bs.it
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
Seminari del Venerdì
14/03/2014
I nuovi farmaci antidiabetici
e l’anziano
Renato Turco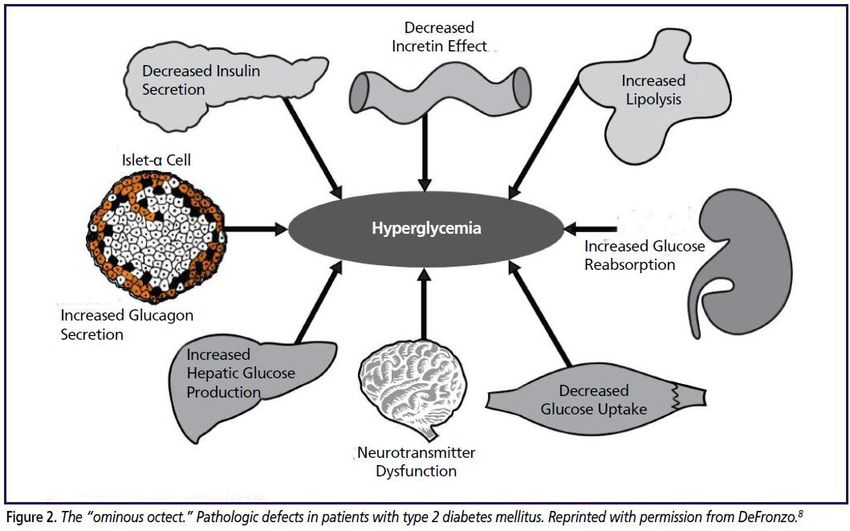
Sommario • Epidemiologia • Classificazione e criteri diagnostici • Target glicemici • Farmaci antidiabetici (vecchi e nuovi) • Management • Conclusioni
Caso clinico
Paziente (XY) di 87 aa, giunta alla nostra osservazione il 23/01 proveniente dalla divisione di cardiologia ospedaliera. Anamnesi fisiologica e familiare • Scolarità: 5° elementare • Casalinga • Vedova, 1 figlio, vive sola Anamnesi patologica remota • Pregressa appendicectomia • Pregressa isterectomia • Diabete mellito 2 • Osteoporosi • Ipercifosi dorsale • Discopatie L5-S1 • Riferito dal figlio, da qualche anno, lieve deficit di memoria
Terapia domiciliare Principio attivo Posologia • Glimepiride 2 1 cp die (pranzo) • Metformina 1000 1 cp die (pranzo) • Acarbosio 50 1 cp die (cena) • Ezetimibe/simvastatina 10/10 1 cp die • ASA 100 1 cp die • Fosinopril 20 1 cp die • Lercanidipina 10 1 cp die • Alendronato 70 1 cp/settimana • Zolpidem 10 1 cp die • Macrogol 1 busta al bisogno

Anamnesi patologica prossima • Il 14/1 per dispnea ingravescente condotta c/o PS e per NSTEMI con scompenso cardiaco secondario ricoverata c/o cardiologia. • All’ecocardiogramma acinesia della parete laterale medio- distale, setto medio distale e parete anteriore medio distale. FE 37%. Sezioni dx nella norma. • Proposta coronarografia, rifiutata dalla pz e dai familiari • Praticata terapia insulinica • Alla dimissione K+3,9; Na+139, creatinina 0,94, BNP 527, Hb 11,5, PLT 160000, GB 7540, troponina 21→2,94
Terapia in atto alla dimissione dalla cardiologia Principio attivo Posologia • Bisoprololo 5 1 cp die • Zofenopril 7,5 1 cp x 2 die • Ivabradina 5 1 cp x 2 die • Furosemide 25 1 cp x die • Kanreonato di K+ 100 ½ cp die • Clopidogrel/ac. acetilsal. 75+75 1 cp die • Omeprazolo 20 1 cp die • Risperidone 0,5 mg x 2 die • Promazina 5 gocce la sera • Atorvastatina 40 1 cp die

Terapia in atto alla dimissione dalla cardiologia Principio attivo Posologia • Bisoprololo 5 1 cp die • Zofenopril 7,5 1 cp x 2 die • Ivabradina 5 1 cp x 2 die • Furosemide 25 1 cp x die • Kanreonato di K+ 100 ½ cp die • Clopidogrel/ac. acetilsal. 75+75 1 cp die • Omeprazolo 20 1 cp die • Risperidone 0,5 mg x 2 die • Promazina 5 gocce la sera • Atorvastatina 40 1 cp die • Ipoglicemizzanti orali sec. schema personale (da noi impiego insulina)
Valutazione multidimensionale
Premorboso Ingresso
C.A.M. 0/4
MMSE 27/30
Geriatric Depression Scale 12/15
Mini Nutritional Assessment 10+9.5/30
IADL (n funzioni perse) 6/8
BARTHEL INDEX 96/100 71/100
TINETTI 19/28
FIM 85/126
Albumina 3.2
APS 0
Ingresso
Esami ematici GB 7.47 10^3/ul 4.00-9.00
GR 4.35 10^6/ul 4.00-5.50
Ht 36.9 % 38.0-50.0
Hb 11.8 g/dl 11.5-14.5
MCV 84.8 Fl 80.0-95.0
PLT 171 10^3/ul 150-400
Neutrofili 43.1 % * 10^3/ul 40.0-75.0
Linfociti 46.6 % * 10^3/ul 20.0-40.0
Monociti 6.3 % * 10^3/ul 0.0-12.0
Eosinofili 3.3 % * 10^3/ul 0.0-2.5
Basofili 0.7 % * 10^3/ul 0.0-0.54
VES 24 mm/1° ora 2-20
PCR 0.6 mg/dl 0.0-1.0
Azotemia 55 mg/dl 10-50
Creatinina 0.85 mg/dl 0.6-1.3
Na 143 MEq/L 135-147
K 4.1 MEq/L 3.5-5.3
Cl 105 MEq/L 97-108
Calcio 4.52 MEq/l 4.2-5.1
Glicemia 168 mg/dl 60-110
GOT 11 U/L 2-31
GPT 10 U/L 3-35
CPK 56 U/L 26-173
Fosfatasi alc 91 U/L 60-258
GT 19 UI/L 0-33
PT (INR) 1.22 0.9-1.2
proteine tot 6 g/dl 6.2-8.5
Albumina 53.5/3.2 %-g/dl 52.0-65.1/3.1-5.2
1 3.7 % 1.0-3.0
2 19.8 % 9.5-14.4
13.9 % 8.6-15.6
9.1 % 10.7-20.3
TSH 1.1 MicroUI/ml 0.27-4.20
Hb glicosilata 7.8 % 4.0-5.6
es. urine PS 1017; pH 5; leucociti+; batteri+Diario clinico
Gli interventi clinici sono stati i seguenti:
• sostituita l’insulina con repaglinide, mantenendo
un discreto compenso dei valori glicemici;
• considerato il buon compenso cardiorespiratorio è stata
ridotta la terapia diuretica;
• ecocardiogramma di controllo: (EF=50%);
• per bradicardia sinusale è stata sospesa la terapia con
ivabradina, instaurata durante il ricovero ospedaliero;
• per insonnia è stata inizialmente praticata terapia con
melatonina, poi sostituita per inefficacia con zolpidem,
risultato invece efficaceTerapia in atto alla dimissione dalla cardiologia Principio attivo Posologia • Bisoprololo 5 1 compressa die • Zofenopril 7.5 1 compressa x 2 die • Furosemide 25 1 compressa die • Atorvastatina 40 1 compressa die • Acido acetilsalicilico/clopidogrel 100+75 1 compressa die • Gastroprotettore sec nota 1 compressa die • Repaglinide 1 1 compressa x 2 die • Alendronato 70 1 compressa martedì • Colecalciferolo 10000 25 gocce martedì • Zolpidem 1/2 compressa die • Macrogol 1 bustina die
Valutazione multidimensionale
Premorboso Ingresso Dimissione
C.A.M. 0/4
MMSE 27/30
Geriatric Depression Scale 12/15
Mini Nutritional Assessment 10+9.5/30
IADL (n funzioni perse) 6/8
BARTHEL INDEX 96/100 71/100 96/100
TINETTI 19/28 25/28
FIM 85/126 104/126
6 MWT 267 mt 300 mtQuesiti • Era adeguata la gestione farmacologica del diabete al domicilio? • …e in ospedale? • …e in riabilitazione?
Sommario • Epidemiologia • Classificazione e criteri diagnostici • Target glicemici • Farmaci antidiabetici (vecchi e nuovi) • Management • Conclusioni
Al Ali et al. BMC Public Health 2013, 13:507
Babitha George et al. EPMA Journal 2010
Liu et al. Health and Quality of Life Outcomes 2010
Juana A Flores-Le Roux et al. Cardiovascular Diabetology 2011
Sommario • Epidemiologia • Classificazione e criteri diagnostici • Target glicemici • Farmaci antidiabetici (vecchi e nuovi) • Management • Conclusioni
CLASSIFICAZIONE
-
Nosografia del diabete
Associazione Medici Diabetologi - Società Italiana di Diabetologia
Standard italiani per la cura del diabete mellito 2009-2010Caratteristiche fisiopatologiche del diabete tipo 2
Craig W. Spellman. J Am Osteopath Assoc. 2011Sommario • Epidemiologia • Classificazione e criteri diagnostici • Target glicemici • Farmaci antidiabetici (vecchi e nuovi) • Management • Conclusioni
These estimates are based on ADAG data of ;2,700 glucose measurements over 3 months per A1C measurement in 507 adults with type 1, type 2, and no diabetes. The correlation between A1C and average glucose was 0.92 (ref. 77). A calculator for converting A1C results into eAG, in either mg/dL or mmol/L, is available at http://professional.diabetes .org/eAG.
Ranges of self-monitored blood glucose
values for various A1c goals
It is not recommended to achieve target fasting glucose values below 70 mg/dL. ** This average uses both
fasting and post-prandial blood glucose readings from continuous glucose monitors or from 7-point daily testing.
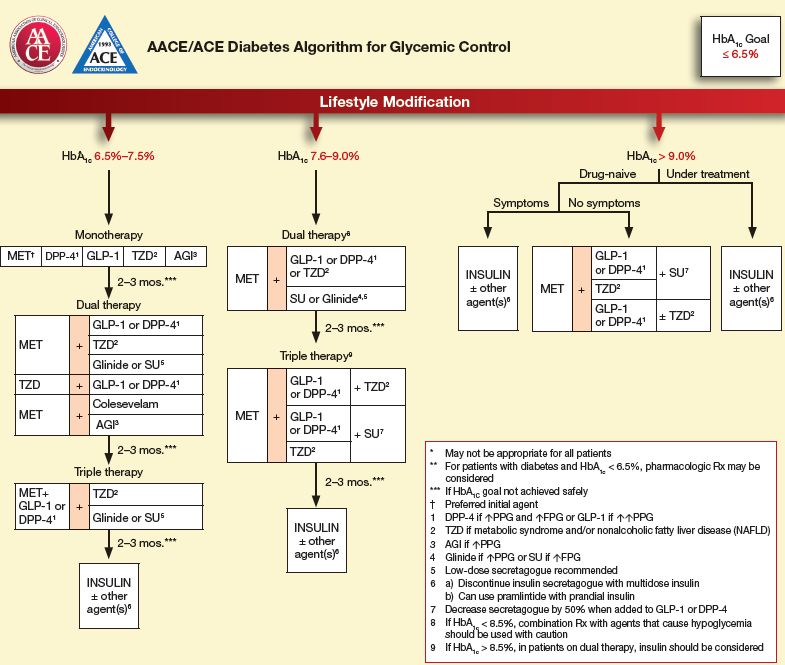
Diagnosis and Management of Type 2 Diabetes Mellitus in Adults. Algorithm Annotations
Fifteenth Edition/April 2012 Institute for Clinical Systems Improvement www.icsi.org 11Treatment of type 2 diabetes mellitus in the elderly patient
The overall goals of diabetes management in older adults
are similar to those in younger adults and include
management of both hyperglycemia and risk factors.
However, in frail elderly patients with diabetes, avoidance
of hypoglycemia, hypotension, and drug interactions due to
polypharmacy are of even greater concern than in younger
patients with diabetes. In addition, management of
coexisting medical conditions is important, as it influences
their ability to perform self-management.
David K McCulloch et al, UpToDate 2014Treatment of type 2 diabetes mellitus in the elderly
patient
SUMMARY AND RECOMMENDATIONS
The appropriate target for hemoglobin A1C (A1C) in
fit elderly patients who have a life expectancy of
over 10 years should be similar to those developed
for younger adults (* **
** ***
*Functional categories of older people with diabetes
Are living independently, have no
important impairments of activities of
daily living (ADL), and who are receiving
none or minimal caregiver support
Have impairments of ADL such as
bathing, dressing, or personal care. This
increases the likelihood of requiring
additional medical and social care.
Characterized by a combination of
significant fatigue, recent weight loss,
severe restriction in mobility and
strength, increased propensity to falls,
and increased risk of institutionalization
Significant memory problems, a degree
of disorientation, or a change in
personality, and who now are unable to
self-care. Many will be relatively
physically well.
IDF Global Guideline for Managing Have a life expectancy reduced to less
Older People with Type 2 Diabetes 2013 than 1 yearGeneral glycaemic targets according
to functional category*
IDF Global Guideline for Managing
Older People with Type 2 Diabetes 2013Research / Projects
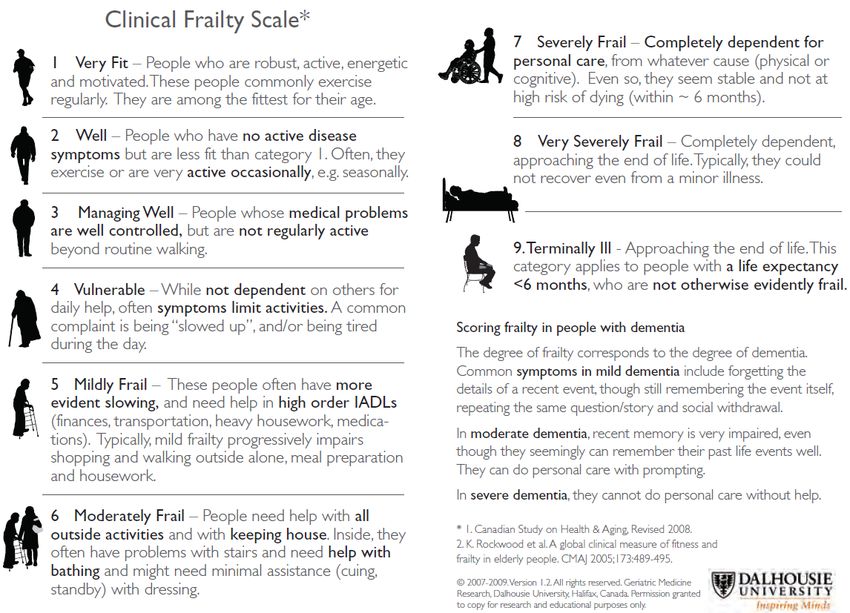
Clinical Frailty Scale ©
• Background: There is no single generally accepted clinical definition of frailty. Previously
developed tools to assess frailty that have been shown to be predictive of death or need for
entry into an institutional facility have not gained acceptance among practising clinicians. We
aimed to develop a tool that would be both predictive and easy to use.
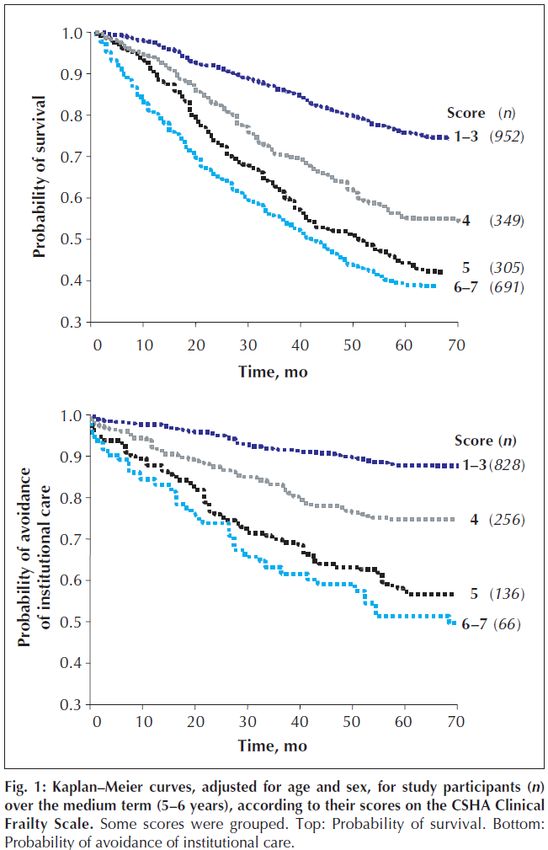
• Methods: We developed the 9-point Clinical Frailty Scale© and applied it and other established
tools that measure frailty to 2305 elderly patients who participated in the second stage of the
Canadian Study of Health and Aging (CSHA). We followed this cohort prospectively; after 5 years,
we determined the ability of the Clinical Frailty Scale© to predict death or need for institutional
care, and correlated the results with those obtained from other established tools.
• Results: The CSHA Clinical Frailty Scale was highly correlated (r = 0.80) with the Frailty Index.
Each 1-category increment of our scale significantly increased the medium-term risks of death
(21.2% within about 70 mo, 95% confidence interval [CI] 12.5%–30.6%) and entry into an
institution (23.9%, 95% CI 8.8%–41.2%) in multivariable models that adjusted for age, sex and
education Analyses of receiver operating characteristic curves showed that our Clinical Frailty
Scale© performed better than measures of cognition, function or comorbidity in assessing risk
for death (areaunder the curve 0.77 for 18-month and 0.70 for 70-month mortality).
• Interpretation: Frailty is a valid and clinically important construct that is recognizable by
physicians. Clinical judgments about frailty can yield useful predictive information.
©2007-2009 Version 1.2. All rights reserved. Geriatric Medicine
Research, Dalhousie University, Halifax, Canada. Permission granted
to copy the Clinical Frailty Scale for research and educational
purposes only.CMAJ • AUG. 30, 2005; 173 (5)
CMAJ, February 4, 2014, 186(2) Frail if they had a score greater than 4
Sommario • Epidemiologia • Classificazione e criteri diagnostici • Target glicemici • Farmaci antidiabetici (vecchi e nuovi) • Management • Conclusioni
Vecchi antidiabetici orali
Biguanides
• They reduce hyperglycemia by decreasing hepatic
gluconeogenesis (primary effect) and increasing peripheral
insulin sensitivity (secondary effect).
• They do not increase insulin levels or cause weight gain.
• Alone, they rarely cause hypoglycemia.
• Are absorbed from the intestines and are not bound to plasma
proteins.
• They are not metabolized and are rapidly eliminated by the
kidneys.
• Drug levels increase markedly in renal insufficiency.
• Lactic acidosis is a rare, but serious, complication that may
occur with drug accumulation
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Lipska et al. Diabetes Care 2011
Sulfanylureas
• Are time-honored insulin secretagogues (ie, oral hypoglycemic
agents). Sulfonylureas function by stimulating the release of
insulin from pancreatic beta cells and can usually reduce
HbA1c by 1-2% and blood glucose concentrations by about
20%.
• The most common adverse effect limiting its use is
hypoglycemia, especially in older adults with impaired renal
function, hepatic dysfunction, and those with poor oral intake.
• To avoid the use of long-acting sulfonylureas (chlorpropamide,
glyburide, and glimepiride) in elderly adults and to prefer to
use a short-acting sulfonylurea, such as glipizide.
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Meglitinides (Repaglinide, Nateglinide)
• They work by stimulating insulin release from pancreatic beta cells
• Have much more short-acting insulin secretagogues than sulfonylureas
• Have similar or slightly less efficacy in decreasing glycemia than
sulfonylureas
• Have similar risk for weight gain as sulfonylureas but possibly less risk of
hypoglycemia
• Unlike nateglinide, repaglinide is principally metabolized by the liver,
with less than 10 percent renally excreted. Dose adjustments with this
agent do not appear to be necessary in patients with renal insufficiency.
In addition, repaglinide is somewhat more effective in lowering A1C than
nateglinide.
• Thus, repaglinide could be considered as initial therapy in a patient with
chronic kidney disease who is intolerant of metformin and sulfonylureas
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Alpha-glucosidase inhibitors
(Acarbose and miglitol)
• Inhibit the gastrointestinal alpha-glucosidases that convert
dietary starch and other complex carbohydrates into
monosaccharides, thereby slowing the absorption of glucose,
which results in a slower rise in postprandial blood glucose
concentrations.
• Have not been widely tested in elderly diabetic patients, but
are likely to be fairly safe and effective.
• The main side effects that limit their use are flatulence and
diarrhea, which are very common
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Nuovi antidiabetici orali
Thiazolidinediones (rosiglitazone and pioglitazone)
• Reduce insulin resistance in the periphery (ie, they sensitize
muscle and fat to the actions of insulin) and perhaps to a small
degree in the liver (ie, insulin sensitizers, antihyperglycemics).
They activate peroxisome proliferator–activated receptor (PPAR)
gamma, a nuclear transcription factor that is important in fat cell
differentiation and fatty acid metabolism. The major action of
thiazolidinediones is probably actually fat redistribution. These
drugs may have beta-cell preservation properties.
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Thiazolidinediones (rosiglitazone and pioglitazone)
• Have moderate glycemic efficacy
• They can be given to patients who have impaired renal function, are well
tolerated in older adults, and do not cause hypoglycemia. However,
thiazolidinediones should not be used in patients with class III or IV heart
failure. In addition, limited experience, high cost, and concerns regarding
fluid retention, congestive heart failure, MI, and fractures limit their
usefulness, particularly in the elderly. If a thiazolidinedione is to be used as
therapy, pioglitazone is preferred because of the greater concern about
atherogenic lipid profiles and a potential increased risk for cardiovascular
events with rosiglitazone.
• New concerns regarding increased risk for bladder cancer with pioglitazone,
in addition to fluid retention and bone loss, have led to decreased enthusiasm
for its use
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Amylinomimetics
These agents mimic endogenous amylin effects by delaying gastric
emptying, decreasing postprandial glucagon release, and
modulating appetite
• Pramlintide
– is a synthetic analog of amylin that is administered by mealtime
subcutaneous injection with insulin. It is available for the treatment of both
type 1 and insulin-treated type 2 diabetes. It requires multiple
subcutaneous injections and, therefore Its role in the management of
diabetes in the elderly is limited
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Sodium-glucose co-transporter 2 (SGLT2)
inhibitors
• SGLT2 is expressed in the proximal tubule and mediates reabsorption of
approximately 90 percent of the filtered glucose load.
• SGLT2 inhibitors promote the renal excretion of glucose and thereby
modestly lower elevated blood glucose levels in patients with type 2
diabetes.
• Canagliflozin (Invokana) lowers the renal glucose threshold (ie, the plasma
glucose concentration that exceeds the maximum glucose reabsorption
capacity of the kidney). Lowering the renal glucose threshold results in
increased urinary glucose excretion.
• Dapagliflozin (Farxiga), reduces glucose reabsorption in the proximal renal
tubules and lowers the renal threshold for glucose, thereby increasing
urinary glucose excretion.
David K McCulloch et al. UpToDate 2014Sodium-glucose co-transporter 2 (SGLT2)
inhibitors
• Decrease in blood pressure and weight,
• Low incidence of hypoglycemia
• Canagliflozin should not be given to patients with eGFRSodium-glucose co-transporter 2 (SGLT2)
inhibitors
• SGLT2 inhibitors reduced A1C by approximately 0.5 to 0.7
percentage points (mean difference versus active comparators -
0.06 percent), making them relatively weak glucose-lowering
agents, similar in potency to the DPP-4 inhibitors.
• We do not recommend sodium-glucose co-transporter 2 (SGLT2)
inhibitors for routine use in patients with type 2 diabetes. SGLT2
inhibitors may play a role as a third-line agent in patients with
inadequate glycemic control on two oral agents (eg, metformin
and sulfonylurea) if for some reason combination metformin and
insulin is not a therapeutic option.
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Glucagonlike Peptide-1 (GLP-1) Agonists
(Exenatide and Liraglutide)Incretins/GLP-1 mimetics
• Incretins are gut-derived peptides secreted in response to meals; the
incretin effect refers to the augmented release of insulin from oral ingestion
of glucose compared with an i.v. glucose challenge. The two major incretins
are GLP-1, which is produced by the neuroendocrine L cells of the ileum and
colon, and glucose-dependent insulinotropic peptide, which is produced by
the K cells of the duodenum and jejunum.
• Both are released rapidly after a meal and they limit postprandial glucose
excursions.
• Incretins stimulate insulin production from pancreatic b cells and GLP-1 also
decreases glucagon secretion, slows gastric emptying, and suppresses
appetite. GLP-1 may also reduce b-cell apoptosis and promote b-cell
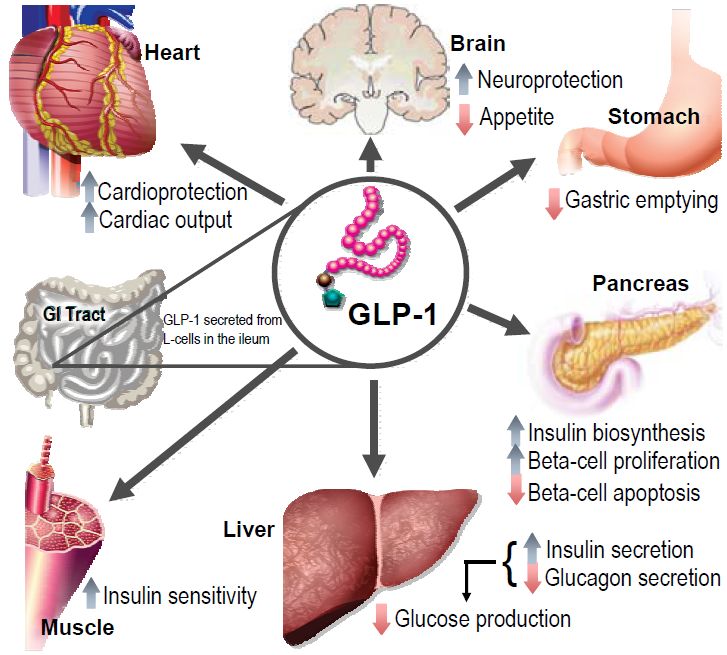
proliferationPhysiology of GLP-1 secretion and action on GLP-1 receptors
in different organs and tissues
(Richard E. Pratley and Matthew Gilbert, The Review of Diabetic Studies 2008)
GLP- 1 is produced postprandially by intestinal L-cells. Through activation of insulin receptors on beta-cells GLP-1 (like GIP) stimulates
insulin biosynthesis and secretion and inhibits glucagon secretion in the pancreas, which in turn reduces hepatic gluconeogenesis. GLP-1
release also exerts protective effects on heart and brain. Insulin sensitivity in the periphery is increased by improved insulin signaling and
reduced gluconeogenesis. Figure modified with permission from Cell Metabolism [3].Incretins/GLP-1 mimetics • Patients with diabetes demonstrate a blunted rise in GLP-1 concentrations after food intake
Glucagonlike Peptide-1 (GLP-1) Agonists
(Exenatide and Liraglutide)
• Have a novel mechanism of action: they mimic the
endogenous incretin GLP-1, stimulating glucose-dependent
insulin release (as opposed to oral insulin secretagogues,
which may cause non–glucose-dependent insulin release and
hypoglycemia), reducing glucagon, and slowing gastric
emptying
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Liraglutide
• Administered once daily
• Not excreted by the kidneys
• Not subjected to DPP-4 degradation
• Associated with reductions in HbA1c and blood pressure
• Provides greater improvements in glycaemic control
• Induces weight loss
• The most common adverse events are nausea, vomiting, and
diarrhea, (10 to 40%)
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Exenatide
• It is usually administered twice daily as injections
• Is resistant to DPP-4 degradation
• Is cleared by the kidneys
• Reduction in both fasting and postprandial glucose concentrations
• A 1–2% reduction in HbA1c concentrations
• Moderate weight loss of 2–5 kg.
• Use caution with moderate to severe renal impairment. Exenatide should not
be used with GFR < 30.
• A recent study of once-weekly dosing using a sustained release formulation of
exenatide showed improvements in glycaemic control, no increased risk of
hypoglycaemia, and similar reductions in body weight.
• Side-effects include nausea and less commonly, vomiting or diarrhoea,
particularly when starting therapy.
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Glucagonlike Peptide-1 (GLP-1) Agonists
(Exenatide and liraglutide)
• There is no risk of hypoglycemia
• Both drugs are sometimes associated with significant
reduction in weight.
• The most common adverse events are nausea, vomiting, and
diarrhea, occurring in 10 to 40 percent of treated patients
• Cost and limited availability of this class in many parts of the
world are major determinants of their use
• Small studies have shown equal efficacy and tolerability in
younger and older people
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Exenatide once weekly versus liraglutide once daily in patients with
type 2 diabetes (DURATION-6): a randomised, open-label study
Abstract
BACKGROUND: Glucagon-like peptide-1 receptor agonists exenatide and liraglutide have been shown to improve
glycaemic control and reduce bodyweight in patients with type 2 diabetes. We compared the efficacy and safety
of exenatide once weekly with liraglutide once daily in patients with type 2 diabetes.
METHODS: We did a 26 week, open-label, randomised, parallel-group study at 105 sites in 19 countries between
Jan 11, 2010, and Jan 17, 2011. Patients aged 18 years or older with type 2 diabetes treated with lifestyle
modification and oral antihyperglycaemic drugs were randomly assigned (1:1), via a computer-generated
randomisation sequence with a voice response system, to receive injections of once-daily liraglutide (1·8 mg) or
once-weekly exenatide (2 mg). Participants and investigators were not masked to treatment assignment. The
primary endpoint was change in glycated haemoglobin (HbA(1c)) from baseline to week 26. Analysis was by
intention to treat. This trial is registered with ClinicalTrials.gov, number NCT01029886.
FINDINGS: Of 912 randomised patients, 911 were included in the intention-to-treat analysis (450 liraglutide, 461
exenatide). The least-squares mean change in HbA(1c) was greater in patients in the liraglutide group (-1·48%, SE
0·05; n=386) than in those in the exenatide group (-1·28%, 0·05; 390) with the treatment difference (0·21%, 95%
CI 0·08-0·33) not meeting predefined non-inferiority criteria (upper limit of CIInsulin vs GLP-1 analogues in poorly controlled Type 2
diabetic subjects on oral therapy: a meta-analysis
Abdul-Ghani MA et al. J Endocrinol Invest. 2013 Mar
Abstract
AIM: To compare insulin and GLP-1 analogues therapy on glycemic control in poorly controlled Type 2
diabetes (T2DM) subjects failing on oral therapy.
METHODS: The electronic database PubMed was systematically searched for randomized controlled
trial (RCT) with duration >16 weeks comparing the addition of insulin therapy vs glucagon-like peptide
(GLP-1) analogues in poorly controlled T2DM subjects on oral therapy.
RESULTS: We identified 7 RCT with 2199 patients of whom 1119 were assigned to insulin therapy and
1080 received a GLP-1 analogue. Both insulin and GLP-1 analogues were effective in lowering glycated
hemoglobin (HbA(1c)) with no statistically significant difference between the mean decreases in
HbA(1c). However, insulin was more effective than GLP-1 analogues in lowering the fasting plasma
glucose concentration, while GLP-1 agonists were more effective in lowering the postprandial glucose
concentration. Insulin therapy was associated with weight gain while GLP-1 analogues consistently
caused weight loss and the difference between the mean change in body weight between the two
therapies was highly statistically significant. Despite a similar decrease in HbA(1c), the risk of
hypoglycemia was 35% lower (p=0.001) with GLP-1 therapy compared to insulin. Compared to insulin,
GLP-1 analogues caused a significant decrease in systolic blood pressure and were associated with
greater rate of gastrointestinal adverse events.
CONCLUSION/INTERPRETATION: In poorly controlled T2DM subjects on oral therapy, GLP-1 analogues
and insulin are equally effective in lowering the HbA(1c). However, GLP-1 analogues have additional
non-glycemic benefits and lower risk of hypoglycemia. Thus, GLP-1 analogues should be considered
as a treatment option in this group of diabetic individuals.The DURATION clinical trial program comprises controlled clinical trials of 24–30 weeks
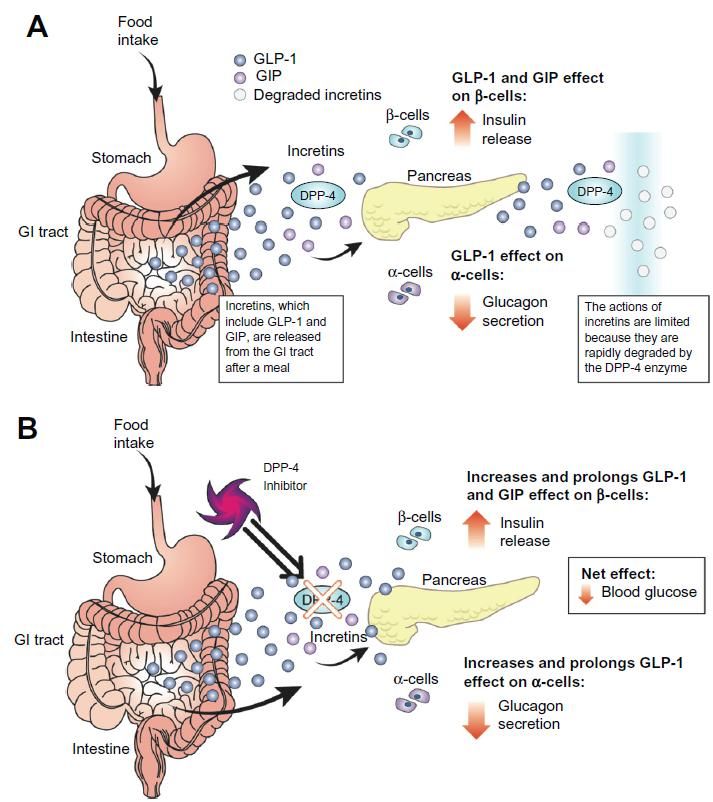
Dipeptidyl Peptidase IV Inhibitors (DPP-4)
• DPP-4 degrades numerous biologically active peptides,
including the endogenous incretins GLP-1 and glucose-
dependent insulinotropic peptide (GIP).
• DPP-4 inhibitors prolong the action of incretin hormones.
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Kristen Kulasa, Steven Edelman.
Core Evidence 2010Dipeptidyl Peptidase IV Inhibitors (DPP-4)
• They mainly:
– have once a day dosing,
– have low risk of hypoglycaemia without the risk of gastrointestinal
side-effects.
– do not reduce appetite or cause weight loss such as GLP-1 agonists
– have lower efficacy (approximate HbA1c lowering by 0.5-0.8%/6-9
mmol/mol) than other agents and may not be easily available in many
countries due to high expense;
– may cause adverse events such as increased blood pressure,
neurogenic inflammation, and immunological reactions. No severe
effects have been reported to date, but further long-term trials are
needed.
• Kyung Soo Kim et al. Diabetes Metab J 2012
• IDF Global Guideline for Managing
• Older People with Type 2 Diabetes 2013
• David K McCulloch et al. UpToDate 2014
• Romesh Khardori et al, Madescape Jan 2014Dennis J. Et al. Hosp Pharm 2013
Dennis J. Et al. Hosp Pharm 2013
Mark Wstolar et al. November 2013
Exenatide once weekly (EQW) resulted
in better long-term glucose control,
greater reductions in fasting plasma
glucose, and more significant weight
loss than sitagliptin.
EQW: Exenatide once weeklyGLP-1 receptor agonists vs DPP-4 inhibitors
Jeffrey S. Freeman, J Am Osteopath Assoc. 2011Piano terapeutico Incretine: si riportano le nuove Determinazioni AIFA per singolo principio attivo e medicinale per la classe delle Incretine e simili (agg. 9 dicembre 2013). Si ricorda che il Piano Terapeutico pubblicato in forma di allegato cartaceo alla Determinazione in GU, nelle more della definizione del PT web-based, è da compilarsi ai fini della rimborsabilità a cura dei Centri specializzati, Universitari o delle Aziende Sanitarie, individuati dalle Regioni e dalle Province autonome di Trento e Bolzano, da rinnovarsi semestralmente e consegnare al paziente in formato cartaceo.
GLP-1 receptor agonists or DPP-4 inhibitors:
how to guide the clinician?
Abstract
Pharmacological treatment of type 2 diabetes has been enriched during recent years, with the
launch of incretin therapies targeting glucagon-like peptide-1 (GLP-1). Such medications comprise
either GLP-1 receptor agonists, with short (one or two daily injections: exenatide, liraglutide,
lixisenatide) or long duration (one injection once weekly: extended-released exenatide, albiglutide,
dulaglutide, taspoglutide); or oral compounds inhibiting dipeptidyl peptidase-4 (DPP-4), the enzyme
that inactives GLP-1, also called gliptins (sitagliptin, vildagliptin, saxagliptin, linagliptin, alogliptin).
Although both pharmacological approaches target GLP-1, important differences exist concerning the
mode of administration (subcutaneous injection versus oral ingestion), the efficacy (better with GLP-
1 agonists), the effects on body weight and systolic blood pressure (diminution with agonists versus
neutrality with gliptins), the tolerance profile (nausea and possibly vomiting with agonists) and the
cost (higher with GLP-1 receptor agonists).
Both agents may exert favourable cardiovascular effects. Gliptins may represent a valuable
alternative to a sulfonylurea or a glitazone after failure of monotherapy with metformin while GLP-1
receptor agonists may be considered as a good alternative to insulin (especially in obese patients)
after failure of a dual oral therapy. However, this scheme is probably too restrictive and modalities
of using incretins are numerous, in almost all stages of type 2 diabetes. Physicians may guide
the pharmacological choice based on clinical characteristics, therapeutic goals
and patient's preference
Scheen AJ. Ann Endocrinol (Paris). 2013 DecSommario • Epidemiologia • Classificazione e criteri diagnostici • Target glicemici • Farmaci antidiabetici (vecchi e nuovi) • Management • Conclusioni
Ma per i pazienti anziani?
Brunetti et al, December 2012 • P&TIDF Global Guideline for Managing Older People with Type 2 Diabetes 2013
Kyung Soo Kim et al
Health Technology Assessment 2010; Vol. 14: No. 36
Costo annuo dei farmaci in Italia
Farmaco Dose Costo annuo in €
Glimepride (Amaryl e generici) 2-4 mg al giorno € 28-47
Metformina (generico) 1.500-2.000 mg al giorno €46-58
Insulina glargine (Lantus) 20-40 UI € 389-778
Saxagliptin (Onglyza) 5 mg al giorno € 849
Sitagliptin (es Januvia) 100 mg al giorno € 855
Vildagliptin (Galvus) 100 mg al giorno € 855
Pioglitazone (Actos) 15-45 mg al giorno € 506-1.277
Exenatide (Byetta) 5-10 mcg x 2 al giorno € 1717
Liraglutide (Victoza) (1,2-1,8mg/die) € 1.777-2.666Brunetti et al,
December 2012 •
P&T
Figure 1 American Diabetes Association algorithm for the treatment of type-2 diabetes mellitusBlood glucose treatment algorithm for older people with diabetes
IDF Global Guideline for Managing
Older People with Type 2 Diabetes 2013Glucose-lowering algorithm for frail patients with type 2 diabetes mellitus
European Diabetes Working Party for Older People 2011
Clinical Guidelines for Type 2 Diabetes Mellitus (EDWPOP)…..ritornando al caso clinico
General glycaemic targets according
to functional category*
IDF Global Guideline for Managing
Older People with Type 2 Diabetes 2013…..ritornando al caso clinico
• Verosimilmente non era adeguata la gestione farmacologica del
diabete al domicilio (assunzione di sulfanilurea a lunga durata
d’azione, associazione di 3 farmaci di cui nessuno a dosaggio
massimo)
• Adeguato l’uso di insulina in ospedale in fase acuta di IMA e
scompenso cardiaco. Non opportuno rilasciare alla dimissione la
terapia pre-ricovero
• E in riabilitazione?
– Si poteva optare per la metformina ma considerato il recente IMA e in
attesa di rivalutazione ecocardiografica è stato preferito l’uso di
repaglinide, poi mantenuta in terapia considerato il mantenimento di
buoni valori glicemiciConclusioni • Nei diabetici anziani funzionalmente dipendenti (fragili e/o con demenza) il target dei valori di A1C è più elevato che in quelli funzionalmente indipendenti • Dei nuovi farmaci antidiabetici alcuni risultano efficaci ma molto costosi, altri meno efficaci e supportati da pochi dati di letteratura sull’efficacia a lungo termine • Nel paziente anziano la scelta del trattamento farmacologico deve essere fatta tenendo conto, oltre che dei valori di A1C, anche delle condizioni funzionali, della comorbilità, dei costi e del rapporto rischio/beneficio • Nell’anziano rimane la metformina il farmaco (seppur vecchio) di prima scelta
Puoi anche leggere