Quali insuline nel diabetico anziano - Dott.ssa Emanuela Gianotti Verona, 25/05/2019 - Accademia di Geriatria
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

Quali insuline nel diabetico anziano
Dott.ssa Emanuela Gianotti
Verona, 25/05/2019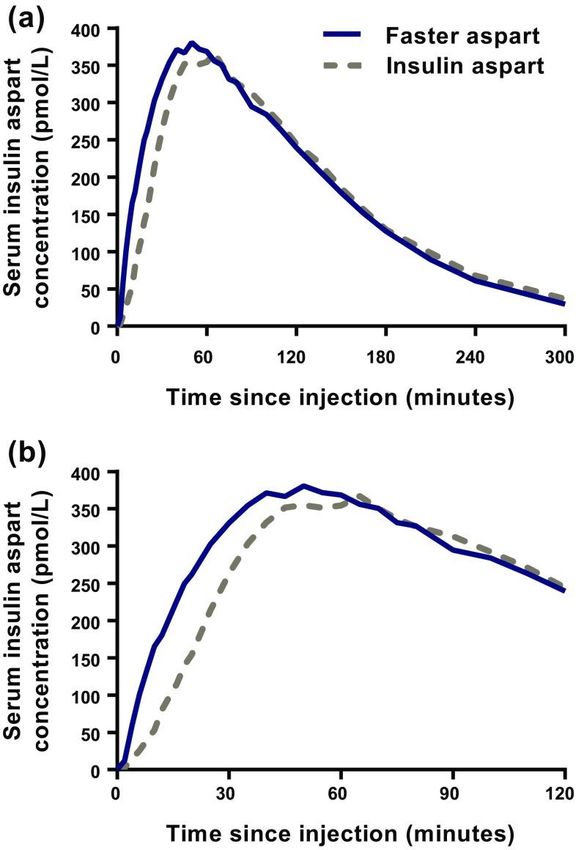
Presentation title Date 2 Il diabete mellito è una patologia molto frequente nell’anziano con percentuali di prevalenza anche superiori al 20% in persone ultrasettantenni. Negli ultimi 10 anni c’è stato un progressivo incremento della prevalenza della malattia nella popolazione di età superiore ai 65 anni, in particolare nelle fasce di età più avanzata. Questo dato trova conferma negli Annali AMD 2011 che hanno valutato 414.814 soggetti con diabete tipo 2 visitati nell’anno 2009 in 236 Servizi di diabetologia italiani; 165.388 pazienti aveva età inferiore a 65 anni, 144.965 avevano un’età compresa tra 65 e 75 anni, 104.461 avevano un’età superiore a 75 anni. Ne risulta che i pazienti affetti da diabete mellito con età> 65 anni rappresentano circa il 60% dei pazienti assistiti dai Centri diabetologici italiani.
Presentation title Date 3 • La locuzione «anziano con diabete mellito» è un termine generico che sottintende una grande varietà di situazioni: la malattia diabetica può essere diagnosticata molti anni prima; possono essere presenti o meno complicanze micro e macrovascolari; possono coesistere fragilità, comorbilità o disabilità che condizionano diverse aspettative di vita. • La fragilità è una sindrome multidimensionale derivante dall’interazione complessa tra variabili sociali, biologiche e psicologiche, predisponente a una maggiore vulnerabilità, al declino funzionale, a cadute, ospedalizzazione e morte.
Aspetti fondamentali della gestione del diabete
in soggetti anziani
Spettanza di vita Stato Funzionale
• Young-old (65-74 anni) • Demenza
• Old-old (75-84 anni) • Malattie concomitanti
• Oldest-old (85+ anni) • Supporto di terzi
Età alla diagnosi Autonomia
• onset in età adulta • Funzionale (cosa posso fare)
• onset in età avanzata
• Decisionale (cosa voglio fare)
5 Il paziente anziano con diabete rappresenta l’esempio paradigmatico di un «patient- centered approach» nella strategia terapeutica della malattia diabetica, come raccomandato in un position statement congiunto ADA/EASD. La cura di questi pazienti dovrebbe garantire «l’assoluta disuguaglianza del trattamento» favorendo l’estrema personalizzazione della terapia.

6 Nell’anziano fragile l’insorgenza di ipoglicemie è facilitata da: • Coesistenza di un deficit cognitivo • Errori nell’ assunzione dei farmaci • Incapacità di valutare rapporto carboidrati dieta/terapia/attività fisica • Insufficiente comprensione da parte del paziente o del care giver • Insufficienza renale • Terapia con sulfaniluree o insulina • Malnutrizione o scarsa alimentazione • Neuropatia autonomica • Ospedalizzazione recente • Ridotta capacità di compenso ed efficacia dei meccanismi controregolatori • Ridotta consapevolezza del paziente • Ridotta intensità dei sintomi • Politerapia
Come possiamo somministrare le varie insuline per raggiungere tali obiettivi in sicurezza?
8 I punti chiave nella gestione della terapia insulinica nel paziente anziano possono essere così riassunti: 1) Utilizzare insuline che possano uniformarsi il più possibile al profilo fisiologico dell’insulino- secrezione. 2) Utilizzare insuline con alta riproducibilità d’azione. 3) Utilizzare insuline con assente o basso rischio di indurre manifestazioni ipoglicemiche. 4) Utilizzare insuline prandiali ad azione “ultrarapida” in associazione basal-bolus
9 I punti chiave nella gestione della terapia insulinica nel paziente anziano possono essere così riassunti: 1) Utilizzare insuline che possano uniformarsi il più possibile al profilo fisiologico dell’insulino- secrezione (analoghi dell’insulina). 2) Utilizzare insuline con alta riproducibilità d’azione. 3) Utilizzare insuline con assente o basso rischio di indurre manifestazioni ipoglicemiche. 4) Utilizzare insuline prandiali ad azione “ultrarapida” in associazione basal-bolus
Perché gli analoghi?
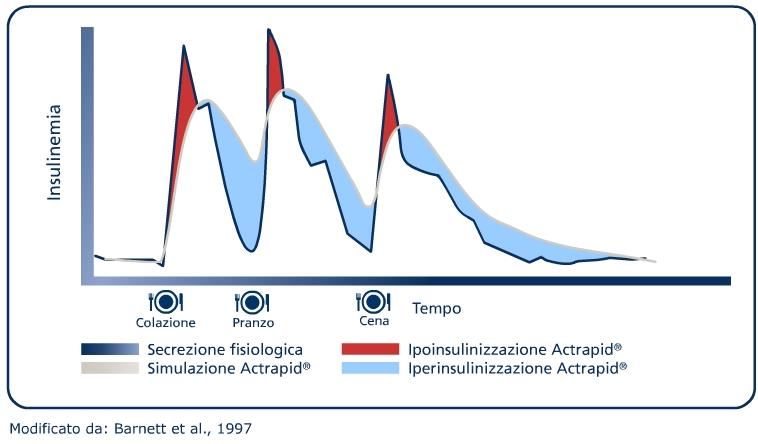
Insulina umana solubile: i limiti
Limiti delle insuline umane
rDNA
rDNA rDNAUltra-fast insulin: approaching a physiological insulin
profile even further
Ultra-fast insulin should:
From the normal pancreas • Better approach physiological insulin
secretion in T1D
Insulin action (at mealtime)*
‘Ultra-fast’ insulin
• Replace early insulin secretion in T2D
Rapid-acting insulin • Have a better profile for pump therapy
Regular human insulin
Time (h)
*Schematic representation
T1D, type 1 diabetes; T2D, type 2 diabetes
Adapted from Home. Diabetes Obes Metab 2015;17:1011–20Changing the formulation: faster aspart is insulin
aspart in a new formulation
Niacinamide: absorption modifier
Vitamin B3
L-Arginine: added for stability
Insulin aspart
Naturally occurring amino acid
Faster aspart, fast-acting insulin aspart
FDA. Inactive Ingredient Search for Approved Drug Products database. www.accessdata.fda.gov/scripts/cder/iig/index.cfm. Accessed June 2016.Niacinamide increases monomer fraction and
permeation rate of insulin aspart
Monomer fraction Permeation rate across
HDMEC cell monolayers
+27%
+35%
6x10-06
0.05
monomers in buffer
Volume fraction of
0.04
Papp (cm/s)
4x10-06
0.03
0.02
2x10-06
0.01
0.00 0
Human Insulin Faster Human Insulin Faster
insulin aspart aspart† insulin aspart aspart†
†Concentration of niacinamide simulating subcutaneous environment after injection
HDMEC, human dermal microvascular endothelial cells
Buckley et al. ATTD 2016 (ATTD-0083);Early insulin exposure – pooled analysis
Twice as fast onset of appearance
Two-fold higher insulin exposure within the first 30 min
300 Faster aspart
Insulin aspart serum conc. (pmol/L)
Insulin aspart
250
200 AUCIAsp, 0–15 min
3.83 (3.41;4.29)b*
150 AUCIAsp, 0–30 min AUCIAsp, 0–1 h AUCIAsp, 0–2 h
2.01 (1.87;2.17)b* 1.32 (1.26;1.39)b* 1.10 (1.06;1.14)b*
100
50
0
0 15 30 60 90 120
4 9 Onset of appearance Time (min)
Onset of appearance –4.9 (–5.3;–4.4) mina*
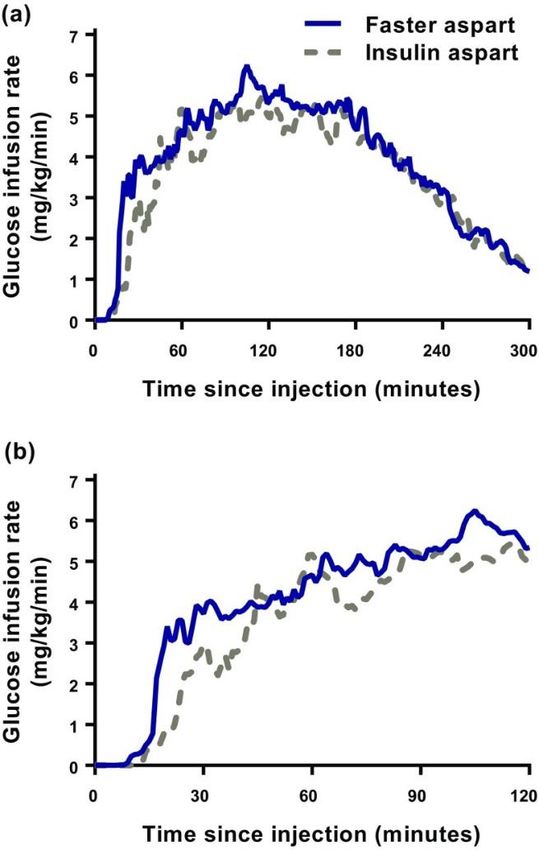
*pEarly insulin action – pooled analysis
74% greater insulin action within the first 30 min
Faster aspart
8 Insulin aspart
6
GIR (mg/kg*min)
4
2 AUCGIR, 0–30 min AUCGIR, 0–1 h AUCGIR, 0–2 h
1.74 (1.47;2.10)b* 1.34 (1.25;1.43)b* 1.13 (1.07;1.19)b*
0
0 30 60 90 120
Onset of action Time (min)
–4.9 (–6.9;–3.0) mina*
*pFaster Aspart nell’anziano Mean serum insulin aspart concentration–time profiles for 5 h (a) and 2 h (b) after administration of faster aspart and insulin aspart (0.2 U/kg) in elderly subjects with type 1 diabetes mellitus
Faster Aspart nell’anziano Mean glucose-lowering effect–time profiles for 5 h (a) and 2 h (b) after administration of faster aspart and insulin aspart (0.2 U/ kg) in elderly subjects with type 1 diabetes mellitus
EGP accounts for a significant proportion of
postprandial hyperglycaemia in T2D
100 (10%)
T2D (n=26) 10
p=0.007
Healthy (n=15) (5%)
80
PPG release over 6 h (g)
4 Glycogenolysis
20 27
15 (28%) Gluconeogenesis
Plasma glucose (mM)
(20%) pSuppression of EGP
Treatment ratio
1.12 (1.01;1.25)a**
0 Faster aspart
30
0 Insulin aspart
25
Suppression of EGP (%)
20
15
Treatment ratio
1.96 (1.13;4.43)a*
10
5
0
30 min 60 min
Two-fold greater suppression of EGP in the first 30 min with faster aspart vs. insulin aspart
*p=0.017; **p=0.040
aTreatment ratio, 95% CI. Full analysis set
CI, confidence interval; EGP, endogenous glucose production; faster aspart, fast-acting insulin aspart
Basu et al. Diabetes Obes Metab 2018;doi: 10.1111/dom.13270; Pieber et al. Diabetologia 2017;60(Suppl 1):690-PLimiti delle insuline basali umane
• assorbimento irregolare
• profilo caratterizzato da un picco d’azione
• durata d’azione non sufficiente
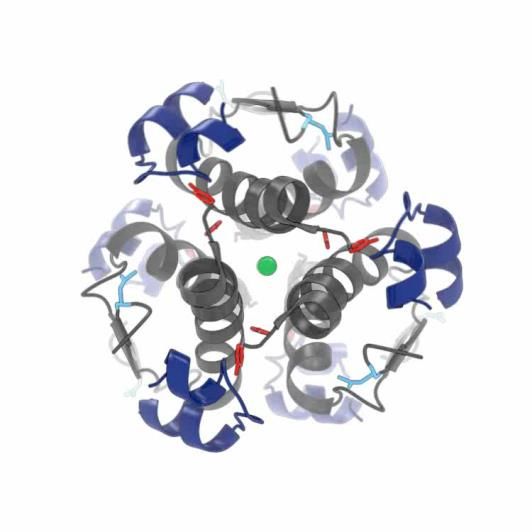
6 13 20Insulin degludec: from injection to slow release
from the subcutaneous depot
Phenol
Zn2+
Insulin degludec injected
Phenol from the vehicle
diffuses quickly, and hexamers link
up via single side-chain contacts
Subcutaneous depot
Long
multi-hexamers
assemble
Zinc diffuses slowly causing individual
hexamers to disassemble, releasing
monomers
Monomers are absorbed from the
Zn, zinc depot into the circulation
Jonassen et al. Pharm Res 2012;29:2104–14IDegludec PD profile at steady state in T2DM
5
0.8 U/kg
0.6 U/kg
0.4 U/kg
GIR (mg/kg/min) 4
3
2
1
0
0 2 4 6 8 10 12 14 16 18 20 22 24
Time since injection (hours)
Nosek et al. ADA 2011; 49-P LB;
Nosek et al. Diabetologia 2011;54(Suppl. 1):S429 (1055-P) (NN1250-1987)26 I punti chiave nella gestione della terapia insulinica nel paziente anziano possono essere così riassunti: 1) Utilizzare insuline che possano uniformarsi il più possibile al profilo fisiologico dell’insulino- secrezione (analoghi dell’insulina). 2) Utilizzare insuline con alta riproducibilità d’azione. 3) Utilizzare insuline con assente o basso rischio di indurre manifestazioni ipoglicemiche. 4) Utilizzare insuline prandiali ad azione “ultrarapida” in associazione basal-bolus
Glucose variability predicts future risk of hypoglycaemia Adapted from Kovatchev et al. Diabetes Care 2006;29:2433–8
Reducing average glycaemia without reducing variability may be dangerous Adapted from Kovatchev et al. Diabetes Care 2006;29:2433–8
Reducing average glycaemia without reducing variability may be dangerous Adapted from Kovatchev et al. Diabetes Care 2006;29:2433–8
Insulin degludec: Significantly less within-patient
variability in glucose control
220
IDeg
200 Four times lower
IGlar
Day-to-day variability (CV%)
pharmacodynamic
180
variability with IDeg
160 vs IGlar (p31 I punti chiave nella gestione della terapia insulinica nel paziente anziano possono essere così riassunti: 1) Utilizzare insuline che possano uniformarsi il più possibile al profilo fisiologico dell’insulino- secrezione (analoghi dell’insulina). 2) Utilizzare insuline con alta riproducibilità d’azione. 3) Utilizzare insuline con assente o basso rischio di indurre manifestazioni ipoglicemiche. 4) Utilizzare insuline prandiali ad azione “ultrarapida” in associazione basal-bolus
Insulin Degludec: Meta-analysis • Prospectively planned • SAP (statistical analysis plan) reviewed by FDA • The revision included: • Which trials to include • How to analyse the data
Insulin degludec phase 3a study programme:
meta-analysis
Rantner et al., Diab Obes Metab 2013Insulin degludec phase 3a study programme:
meta-analysis
70 Maintenance period
Full trial Maintenance
60
Overall Overall
50
Insulin dose (U)
Pooled T2D/T1D –9%* –16%* 40
Nocturnal
Nocturnal 30
Pooled T2D/T1D –26%* –32%* 20
IDeg OD
10 IGlar OD
Hypoglycaemia risk reduction IDeg versus IGlar
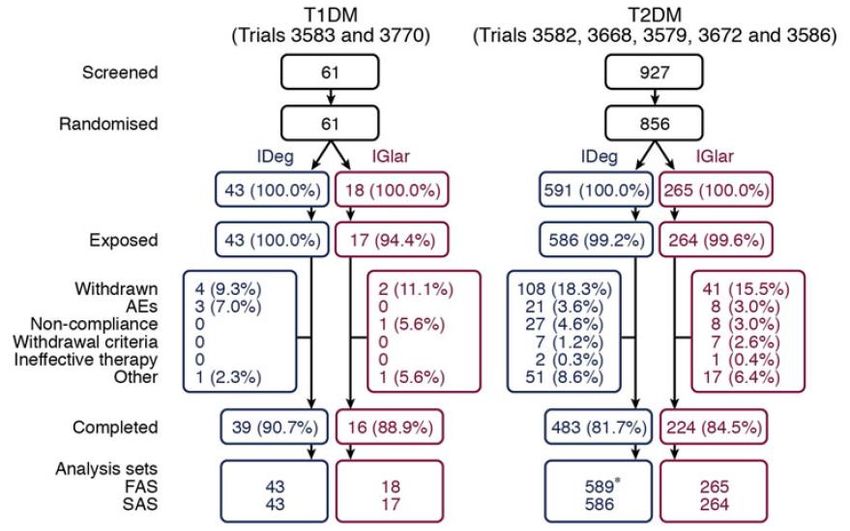
*Statistically significant, pInsulin Degludec: hypoglycaemia meta-analysis in elderly ❑ Hypoglycaemia data from patients ≥65 years of age with type 1 (T1DM) or type 2 (T2DM) diabetes from seven randomised, treat-to-target phase IIIa trials were used to compare IDeg and IGlar in a pre-planned meta-analysis ❑ Overall, 917/4345 (21 %) randomised patients in the seven trials were elderly (634 IDeg, 283 IGlar) ❑ Treatment comparisons of hypoglycaemia in T1DM patients were not performed due to Sorli et al., Drugs Aging 2013 low numbers of elderly patients with T1DM randomised (43 IDeg, 18 IGlar);
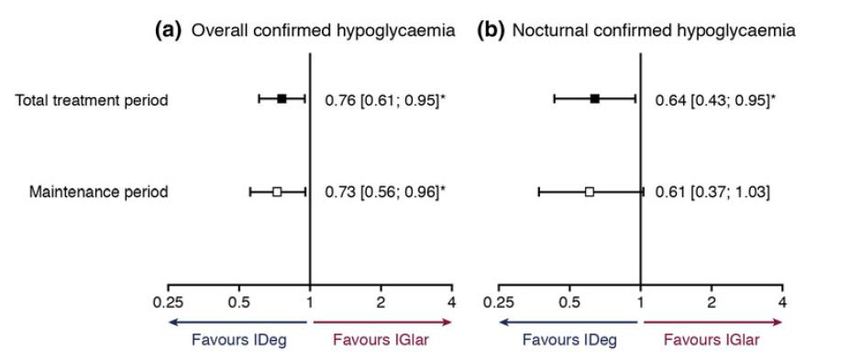
Insulin Degludec: hypoglycaemia meta-analysis in
elderly
Estimated rate ratios (IDeg/IGlar) with 95 % confidence
intervals in elderly patients >65 years of age with T2DM
❑ In elderly patients with T2DM, the
rate of overall confirmed
hypoglycaemia was significantly
lower with IDeg than IGlar
[estimated rate ratio (ERR) 0.76
(0.61; 0.95)95 % CI]; nocturnal
-24% -36% confirmed hypoglycaemia was also
significantly lower with IDeg [ERR
0.64 (0.43; 0.95)95 % CI]
-27% -39% ❑ Results of this pre-planned meta-
analysis in elderly patients with
diabetes demonstrate a significant
reduction in hypoglycaemic events
with IDeg relative to IGlar
Sorli et al., Drugs Aging 2013Clinical outcome assessment of the effectiveness of
insulin degludec in real-life
medical practice (CONFIRM): a comparative
effectiveness study of degludec and
insulin glargine 300 units/mL in
insulin-naïve patients with type 2 diabetes
Joseph Tibaldi, Steffen Haldrup, Viktor Sandberg,
Michael Lyng Wolden, Helena W. Rodbard
Tibaldi et al. ADA 2018, poster 98-LB IT/TRE/0618/0122COMFIRM: a comparative effectiveness study of degludec and insulin glargine 300 U/ml Tibaldi et al. ADA 2018, poster 98-LB
39 I punti chiave nella gestione della terapia insulinica nel paziente anziano possono essere così riassunti: 1) Utilizzare insuline che possano uniformarsi il più possibile al profilo fisiologico dell’insulino- secrezione (analoghi dell’insulina). 2) Utilizzare insuline con alta riproducibilità d’azione. 3) Utilizzare insuline con assente o basso rischio di indurre manifestazioni ipoglicemiche. 4) Utilizzare insuline prandiali ad azione “ultrarapida” in associazione basal-bolus
insulin aspart in the setting of
insulin
degludec-treated type 1 diabetes:
efficacy and safety from a randomized
double-blind trial
Buse JB et al. DOM 2018Aim and trial design
Aim: to evaluate the efficacy and safety of faster aspart, administered at mealtime or post-meal, versus
mealtime insulin aspart, both in combination with insulin degludec, in subjects with T1D
Key inclusion criteria: Primary endpoint:
• T1D ≥12 months • Change from baseline in HbA1c 26 weeks after randomization
• Male or female ≥18 years
Confirmatory secondary endpoints:
(for Japan and Taiwan: ≥20 years)
• Basal–bolus insulin ≥12 months • Change from baseline in 1-h PPG increment 26 weeks after randomization (meal test)
• Basal insulin analogs ≥4 months • Change from baseline in 1,5-anhydroglucitol 26 weeks after randomization
• HbA1c 7.0–9.5% (53–80 mmol/mol; both inclusive)
• BMI ≤35.0 kg/m2
Double-blind
Faster aspart (mealtime) + insulin degludec†
Patients with Insulin aspart
T1D on basal– (mealtime) Insulin aspart (mealtime) + insulin degludec†
bolus treatment + insulin degludec
Faster aspart (post-meal) + insulin degludec‡
8 weeks 26 weeks FU*
Run-in Randomization (1:1:1) End of treatment
†Double-blind
arm; ‡open-label arm; *follow-up (7–30 days)
BMI, body mass index; faster aspart, fast-acting insulin aspart; FU, follow-up; PPG, postprandial plasma glucose; T1D, type 1 diabetesPR
Buse JB et al. DOM 2018PPG increment at week 26 (meal test) Faster aspart
(mealtime)
Faster aspart
(post-meal)
Mealtime comparison
Insulin aspart
(mealtime)
2-h ETD [95% CI]
7 −0.35 mmol/L [−0.98;0.27] 126
–6.4 mg/dL [−17.60;4.84]
6 108
PPG increment (mmol/L)
*
PPG increment (mg/dL)
5 90
4 * 72
3 1-h ETD [95% CI]* 54
Superiority
−0.90 mmol/L [−1.36;−0.45]
–16.2 mg/dL [–24.4; –8.1] confirmed
2 36
30-min ETD [95% CI]*
1 −0.52 mmol/L [−0.83;−0.20] 18
–9.3 mg/dL [−14.99;–3.67]
0 0
0 30 60 120 180 240
Bolus
dose Time (min)
0.1 U/kg
*pSevere or BG-confirmed hypoglycemia during
26 weeks of treatment
ERR [95% CI] Faster aspart (mealtime)
MT: 0.84 [0.70;1.01]
45 PM: 0.97 [0.81;1.16] Faster aspart (post-meal)
40.1
39.4 Insulin aspart (mealtime)
Hypoglycemia rate (episodes/PYE)
40
34.1
35
30
25 Meal-related severe or BG-confirmed hypoglycemia
20
ERR [95% CI] ERR [95% CI] ERR [95% CI] ERR [95% CI]
15 MT: 1.09 [0.73;1.63] MT: 0.75 [0.53;1.07] MT: 0.86 [0.64;1.15] MT: 0.72 [0.54;0.96]*
PM: 1.26 [0.84;1.89] PM: 0.99 [0.70;1.40] PM: 1.20 [0.89;1.60] PM: 1.00 [0.76;1.32]
ERR [95% CI]
10 MT: 1.01 [0.58;1.78]
PM: 0.74 [0.40;1.35]
4.4 4.0 4.0
5 2.6 2.4 3.0 3.6 2.8
1.5 1.6 1.3 1.8
0.3 0.2 0.3
0
Overall Severe 0–1
0-1 h >1–2
>1-2 hh >2–3
>2-3hh >3–4
>3-4hh
*p=0.024
Ratios estimated using a negative binomial model. Treatment-emergent is defined as an event that has onset up to 1 day after last day of randomized
treatment and excluding the events occurring in the run-in period. BG-confirmed: PG valueConclusions
• Compared with mealtime IAsp in the setting of insulin degludec-
treated T1D
• Faster aspart (mealtime and post-meal) provides effective glycemic control
(non-inferiority confirmed)
• Mealtime faster aspart provides superior control over 1-h PPG excursions
• Faster aspart has a similar overall safety profile
• Administration of faster aspart up to 20 min after the start of a meal,
although less favorable compared with mealtime administration, may
be considered for some people with T1D under certain circumstances.
Faster aspart, fast-acting insulin aspart; IAsp, insulin aspart; PPG, postprandial plasma glucose; T1D, type 1 diabetes
Buse JB et al. DOM 2018Abbiamo parlato di insuline ma………………. Non dimentichiamo una valida alternativa al basal bolus
IDegLira: a once-daily, titratable, fixed-ratio
combination
1.8 mg 50 Maximum dose
dose steps
IDegLira is dosed in dose steps, with
component
Liraglutide
Fixed-ratio
1 dose step equivalent to:
1 dose step
STARTING DOSES
1 U insulin degludec =
0.58 mg 16 +
Patients uncontrolled on
1 U insulin degludec
+
0.036 mg liraglutide
basal insulin or GLP-1RA
dose steps 0.036 mg liraglutide
0.36 mg 10 Patients uncontrolled
dose steps on OAD(s)
10 units 16 units 50 units
Insulin degludec component
GLP-1 RA, glucagon-like peptide-1 receptor agonist; IDegLira, insulin degludec/liraglutide; OAD, oral antidiabetic drug
Summary of Product Characteristics (SmPC), 2017DUAL VII
Study design IDegLira
Starting dose: 16 dose steps
IDegLira + metformin Maximum dose: 50 dose steps
Subjects with T2D (n=252) IGlar U100
uncontrolled on Starting dose: Pre-trial dose
Maximum dose: None
basal insulin IGlar U100 + IAsp (≤4 times) +
IAsp
(N=506) metformin (n=254) Starting dose: 4U†
Maximum dose: None
Screening Randomisation 1:1 (open label) End of trial 1st FU 2nd FU
–2 0 Week 26 27 30
Inclusion criteria IDegLira Iglar U 100 + IAsp
• Type 2 diabetes
• Age ≥18 years BMI, kg/m2 31,7 31,7
• HbA1c 7.0–10.0%
• IGlar U100 20–50 U + metformin Duration of diabetes, years 13,2 13,3
• BMI ≤40 kg/m2 HbA1c, % 8,2 8,2
BG, blood glucose; BMI, body mass index; FU, follow-up; HbA1c, glycosylated haemoglobin; IAsp, insulin aspart; IDegLira, insulin degludec/liraglutide
combination; IGlar U100, insulin glargine 100 units/mL; PG, plasma glucose; T2D, type 2 diabetes; U, units.
Billings et al. ADA 2017;136-OR.DUAL VII
Key clinical findings
HbA1c Hypoglycaemia† Body Weight
IDegLira IGlar U100 IDegLira IGlar U100 IDegLira IGlar U100
Change in body weight (kg)
+ IAsp + IAsp + IAsp
0,0 3
Change in HbA1c (%)
10
Hypoglycaemia rate
-0,5 2
(episodes/yr)
8
8,17
-1,0 1
6
-1.48 -1.46
4 0
-1,5
-0,93
ETD: 2 1,07 -1
-2,0 –0.02% [–0.16; 0.12]95% CI,
pGrazie per l’attenzione
Puoi anche leggere