BIOSIMILARI: INFLIXIMAB IN GASTROENTEROLOGIA - GOVERNO CLINICO E FARMACI BIOSIMILARI - Progetto Farmagood - 27 maggio 2015 - Auditorium ASL MB ...
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
GOVERNO CLINICO E FARMACI BIOSIMILARI
- Progetto Farmagood –
BIOSIMILARI: INFLIXIMAB IN GASTROENTEROLOGIA
27 maggio 2015 – Auditorium ASL MB, Monza
Dott.ssa Maria Milanese
UO Medicina Generale AO Desio e Vimercate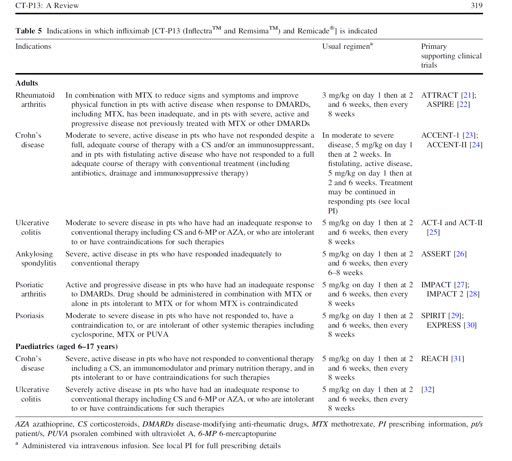
1) Morbo di Crohn (MC) e Colite ulcerosa (CU): definizioni e attività di malattia 2) Indicazione ad anti-TNF: linee guida europee (ECCO) ed italiane (SIGE-IGIBD) 3) Infliximab biosimilare (Remsima ed Inflectra): caratteristiche farmacologiche ed evidenze cliniche, estrapolazione da AR e SA 4) Conclusioni
Morbo di Crohn (MC):
malattia infiammatoria cronica intestinale, che può colpire
qualsiasi parte del tratto digerente, dalla bocca all’ano, in
maniera discontinua.
• Stenosante > restringimento dei
visceri che può portare ad
occlusione intestinale o modifica
delle dimensioni delle feci)
• Penetrante > crea passaggi
anomali – fistole - tra i visceri e
altre strutture
• Infiammatoria > causa
infiammazione, non stenosi/
fistole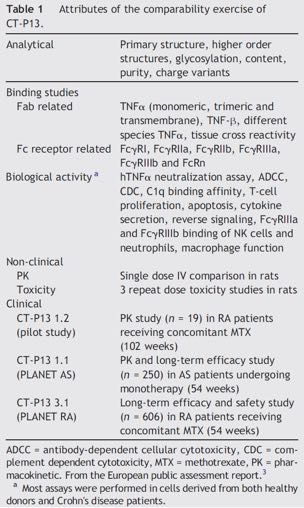
MC: ATTIVITA’ DI MALATTIA
-RISPOSTA: Δ CDAI ≥ 100 o Δ HBI ≥ 3 -REMISSIONE: CDAI < 150 o HBI < 4, senza steroide -RELAPSE: ricomparsa di sintomi con CDAI > 150 (Δ CDAI ≥ 70-100) o HBI > 4 in pz in remissione clinica -EARLY RELAPSE: ricomparsa di sintomi prima di 3 mesi dalla remissione -PATTERN OF RELAPSE: infrequente (≤ 1/anno), frequente (≥ 2/anno), continuo -RICORRENZA: comparsa di nuove lesioni tipiche dopo resezione curativa di malattia macroscopica, generalmente nel neo-ileo terminale e/o a livello anastomotico, rilevate endoscopicamente, radiologicamente o chirurgicamente -MC STEROIDO-REFRATTARIO: malattia attiva nonostante una dose ed una durata adeguata di terapia steroidea (prednisone 0.75-1 mg/Kg/die per os o eq per almeno 2 settimane -MC STEROIDO-DIPENDENTE: impossibilità di ridurre steroide al di sotto di 10mg/ die di prednisolone o budesonide sotto 3g/die entro 3 mesi dall’inizio, senza relapse di malattia o relapse entro 3 mesi dalla sospensione dello steroide
Colite ulcerosa (CU): COLITE ULCEROSA > condizione infiammatoria cronica che causa una continua infiammazione della mucosa del colon senza evidenza di granulomi alla biopsia, che colpisce il retto ed un'estensione variabile del colon senza soluzioni di continuità, caratterizzata da un decorso che alterna fasi di quiescenza e fasi di riaccensione IBD NON CLASSIFICATA > minoranza di casi nei quali non si può stabilire con chiarezza una distinzione tra MC, CU ed altre cause di colite in base alla storia, ai dati endoscopici, istopatologici e radiologici COLITE INDEETERMINATA > caratteristiche miste tra MC e CU a livello istopatologico DISTRIBUZIONE DELLA CU: proctite, left-sided, extensive
Colite ulcerosa (CU): ATTIVITA' DI MALATTIA

- REMISSIONE: ≤ 3 scariche/die senza sanguinamento o urgenza - RISPOSTA: : miglioramento clinico ed endoscopico in base all’indice di attività utilizzato - RELAPSE: ricomparsa di sintomi in pz in remissione clinica - EARLY RELAPSE: ricomparsa di sintomi prima di 3 mesi dalla remissione - PATTERN OF RELAPSE: infrequente (≤ 1/anno), frequente (≥ 2/anno), continuo - COLITE STEROIDO-REFRATTARIA: malattia attiva nonostante una dose ed una durata adeguata di terapia steroidea (prednisone 0.75-1 mg/Kg/die per os o eq per almeno 2 sett o metilprednisolone 1mg/Kg/die ev per un periodo di una settimana) - COLITE STEROIDO-DIPENDENTE: impossibilità di ridurre steroide al di sotto di 10mg/die di prednisolone o eq entro 3 mesi dall’inizio, senza relapse di malattia o relapse entro 3 mesi dalla sospensione
2) INDICAZIONE AD ANTI-TNF: linee guida europee (ECCO) ed italiane (SIGE-IGIBD) •Opzione valutabile in induzione (“top down approach” in pz selezionati > malattia estesa, severa malattia rettale, giovane età, severa malattia perianale alla diagnosi, necessità di steroide alla diagnosi) e mantenimento della remissione in MC steroido- refrattario o –dipendente •Prima scelta in fistole perianali complesse in associazione a chirurgia •Possibile in induzione e mantenimento in CU moderata-severa steroido-refrattaria o in pz steroido-dipendenti intolleranti/refrattari a tiopurine •Riduce il tasso di colectomia entro 3 mesi in CU severa steroido- refrattaria, controindicati in malattia complicata
• Considerabili come prevenzione della ricorrenza post-chirrugica in pazienti altamente selezionati (malattia fistolizzante, localizzazione ileale, fumo di sigaretta, giovane età, precedente resezione, estensione delle lesioni e tipo di anastomosi) • Suggerito in artrite assiale e/o periferica in caso di fallimento della terapia standard; trattamento di scelta in SA • Uso precoce valutabile in pioderma gangrenoso • Considerabili in casi resistenti di uveite • Opzione in pouchite refrattaria
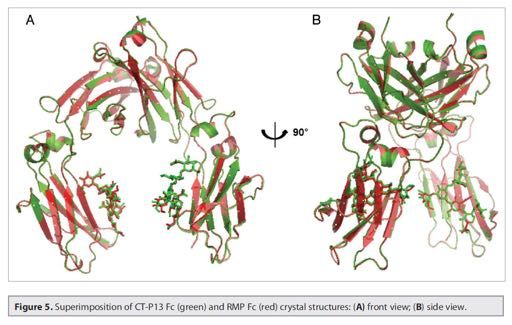
3) Infliximab biosimilare (CT-P13 - Remsima e Inflectra): caratteristiche farmacologiche ed evidenze cliniche, estrapolazione da AR e SA Caratterizzazione fisico-chimica di Remsima
Remsima EMA/CHMP/363689/2013
Perchè può essere opportuno extrapolare?
European Medicines Agency sull’ extrapolazione
“The primary rationale for extrapolation is to avoid
unnecessary studies in the target population for
ethical reasons, for efficiency, and to allocate
resources to areas where studies are the most
needed.“1
EMA Concept paper on extrapolation of efficacy and safety in medicine development (Final). EMA/129698/2012, 2013La pratica dell’extrapolazione è peraltro usata
tutti i giorni nella nostra pratica clinica
Dal$trial$clinico$all’a,vità$clinica$quo1diana$
Da$modelli$sperimentali$ad$uomo$ Terapie$in$gravidanza$
Da$volontari$sani$a$pazien1$
AFMC Website: http://phprimer.afmc.ca/Part2-MethodsStudyingHealth/Chapter5AssessingEvidenceAndInformation/BiasCross-immunogenicity: antibodies to infliximab in Remicade-treated patients with IBD similarly recognise the biosimilar Remsima
Patie Description
Study nts
S t u d y C T- P 1 3 RA Long term follow-up of phase I study in CT-P13 patients
1.2
S t u d y C T- P 1 3 AS open-label, single-arm extension of CT-P13 patients in study CT-
1.3 P13 1.1
S t u d y C T- P 1 3 RA open-label, single-arm extension of CT-P13 patients in study CT-
3.2 P13 3.1
S t u d y C T- P 1 3 RA Phase III equivalence study vs. Remicade (MTX) (Russia)
3.3
S t u d y C T- P 1 3 RA Double blind parallel group study vs. Remicade (MTX) (Japan)
101
Registry CT-P13 RA Safety (TB and Serious infections) and Efficacy of Inflectra (EU
4.2 and Korea)(targeted enrollment 3100 patients)
Registry CT-P13 C D / prospective cohort study to evaluate the safety (TB and serious
4.3 UC infections) )(targeted enrollment 3100 patients) and efficacy (EU
and Korea)
S t u d y C T- P 1 3 CD Randomized, Double-Blind, Parallel-Group, Phase 1/3 Study
3.4 efficacy, safety and PK of CT-P13 vs. Remicade in (Global)Kang YS, Moon HH, Lee SE, Lim YJ, Kang HW. Dig Dis Sci. 2015 Apr;60(4):951-6.
METHODS: Seventeen subjects diagnosed with Crohn's disease (CD, n = 8) or ulcerative colitis (UC, n = 9) who were administered CT-P13 from November 2012 to October 2013 at Dongguk University Ilsan Hospital were retrospectively enrolled. Medical records analyzed included patients' characteristics, previous history of anti- tumor necrosis factor administration, response and remission to this biosimilar antibody, disease flare-up, and adverse drug reaction. RESULTS: Male-female ratio was 1.8. Mean age was 35.4 years (range 15-57). Mean number of CT-P13 administrations was 4.2 ± 1.9. Induction treatments were done in five UC and three CD patients. Clinical response and remission at 8 weeks were achieved in seven patients (five UC and two CD). One CD patient did not respond to CT-P13. Nine patients in maintenance with the originator were interchanged with CT- P13 (four UC and five CD patients). One UC patient experienced arthralgia and CT- P13 was discontinued. One patient experienced loss of response during the study period. CONCLUSIONS: CT-P13 may have biosimilarity and interchangeability with its originator in inflammatory bowel disease. A large, randomized, double-blind, prospective study is needed.
Efficacy and safety of CT-P13, a biosimilar of infliximab, in patients
with inflammatory bowel disease: A retrospective multicenter study.
METHODS: This was a retrospective multicenter study including both anti-TNF naïve
patients and patients who switched from the biologic originator to CT-P13.
RESULTS:
In anti-TNF naïve CD patients (n=32), clinical response and remission rates were 90.6% and
68.8% at week 2, 90.6% and 84.4% at week 8, 95.5% and 77.3% at week 30, and 87.5% and
75.0% at week 54, respectively. In anti-TNF naïve UC patients (n=42), clinical response and
remission rates were 76.2% and 19.0% at week 2, 81.0% and 38.1% at week 8, 91.3% and
47.8% at week 30, and 100% and 50.0% at week 54, respectively, while mucosal healing rates
were 58.3% at week 8, 66.7% at week 30, and 66.7% at week 54. The efficacy of CT-P13 was
maintained in 92.6% (25/27) of CD patients and in 66.7% (6/9) of UC patients after switching
from its originator. Adverse events related to CT-P13 occurred in 11.8% of UC patients.
CONCLUSIONS:
CT-P13 appears to have comparable efficacy, safety, and interchangeability with its
originator in the treatment of IBD. Further prospective studies with long-term follow-up
periods will be needed to confirm the biosimilarity of CT-P13.
J Gastroenterol Hepatol. 2015 May 14, Jung YS1 et alABSTRACT 10th Congress of ECCO, Barcelona P691 Budget impact analysis of introducing biosimilar infliximab for the treatment of gastro intestinal disorders in five European countries Poster presentations: Epidemiology (2015) P456 First observations of the use of biosimilar infliximab for treatment of ulcerative colitis in paediatric population. Poster presentations: Clinical: Therapy & observation (2015) P295 Preliminary assessment of efficacy and safety of switching between originator and biosimilar infliximab in paediatric Crohn disease patients. Poster presentations: Clinical: Therapy & observation (2015) P314 Biosimilar infliximab in inflammatory bowel diseases: first interim Results from a prospective nationwide observational cohort Poster presentations: Clinical: Therapy & observation (2015) P430 Assessment of safety and efficacy of biosimilar infliximab in children with Crohn disease: a preliminary report. DOP078. Are IBD specialists aware of biosimilar monoclonal antibodies? Results from a survey among ECCO members DOP Session 9 - Therapy today
P505 Biosimilar but not the same Poster presentations: Clinical: Therapy & observation (2015) P565. An experience of anti-TNF biosimilar, CT-P13 use: clinical efficacy, safety and interchangeability in inflammatory bowel disease; a pilot study Poster presentations: Clinical: Therapy & observation (2014) P540 Efficacy and safety of infliximab's biosimilar (REMSIMA) for IBD Poster presentations: Clinical: Therapy & observation (2015) P137 5 year budget impact analysis of CT-P13 (Infliximab) for the treatment of Crohn's Disease in UK, Italy and France Poster presentations: Clinical: Diagnosis & outcome (2015) P603 Efficacy of the new infliximab biomarker CT-P13 induction therapy on mucosal healing in ulcerative colitis patients Poster presentations: Clinical: Therapy & observation (2015)
! P456 First observations of the use of biosimilar infliximab for treatment
of ulcerative colitis in paediatric population.
! Methods: Six patients starting treatment with biosimilar infliximab Remisma (5 mg/kg) was assessed at
week 10 after receiving 3 doses at weeks 0, 2 and 6. Disease activity (PUCAI) and laboratory values (CRP,
ESR, platelet count) was assessed at the start of the biological therapy and at week 10. Mean and range of
clinical values is reported.
! Results: Median age of 6 patients was 12.3 years (range 8.5-17.5). Mean PUCAI before infliximab
initiation was 47.5 (range 5-80). Mean (range) CRP, ESR and platelet count before initiation were 1.8 mg/
dL (0.03-8.1), 24 mm (5-33) and 370x109/L (260-530x109). For one patient it was the second course of
biological treatment (3 doses of the reference INF received 9 months ago. For 2 patients (33%) treatment
was discontinued, in 1 due to lack of response after first dose (disease flare), in second due to anaphylactic
reaction during dose 3 infusion. For the latter patient that was the second course of infliximab treatment.
As of November 2014 3 patients (50%) received 3 doses and were evaluated at week 10. For these patients
initial values of PUCAI, CRP, ESR and platelet count were not different than for all 6 patients. After 3
doses of biosimilar infliximab PUCAI values decreased to 28.3 (range 5-50). CRP, ESR and platelet count
were 0.3 (0.02-0.68), 20 (10-28) and 418x109 (236-706), respectively.
! Conclusion: Initial observations point to efficacy and safety of biosimilar infliximab in the treatment of
pediatric patients with ulcerative colitis. Further studies with larger patient groups are required. Data for
more patients and longer observation time will be collected and presented.! P295 Preliminary assessment of efficacy and safety of switching between
originator and biosimilar infliximab in paediatric Crohn disease patients.
Methods: Thirty-two paediatric patients with diagnosis of CD from 3 academic hospitals who were switched
from originator to biosimilar infliximab (CT-P13) were included in the study. Patient characteristics,
disease history, disease severity (PCDAI), laboratory values (CRP, ESR, platelet count, haemoglobin level)
were recorded. Mean, median and range values were calculated. Adverse events were recorded before and
after the switch.
Results: Mean age of patients at diagnosis of CD was 11.1 years (range 2.7-15.3). Six patients had been
previously treated with a biologic: infliximab (5) or adalimumab (1). Mean time from CD diagnosis to the
start of current biological treatment was 1.8 years (range: 1 week - 5 years). Mean number of originator
INF infusions before the switch to biosimilar was 9.9 (median 8.0; range 4-29). Disease activity (PCDAI)
and laboratory values at the beginning of originator INF treatment, before switch and after first dose
after switch are presented in the Table as mean (median; range). Number of patients may vary due to lack
of data at given time point.Disease activity (PCDAI) and laboratory values at the beginning of originator
INF treatment, before switch and after first dose after switch are presented as mean (median; range).
There were no infusion reaction after originator of biosimilar INF treatment. The occurrence of sporadic
mild adverse events did not differ significantly when were measured before and after switching and was
consistent with INF molecule safety profile. Additionally, at weeks 16, 24, 32 after switch 16, 5 and 4
patients were evaluated with no disease flare or unexpected adverse events.
Conclusion:Switching form originator to biosimilar infliximab in children with CD seems to be safe$$ Inizio$tra;amento$$ Penul1ma$ Ul1ma$ Prima$ Seconda$
con$IFX$originator$ infusione$di$IFX$ infusione$di$IFX$ infusione$di$IFX$ Infusione$di$IFX$
originator$ originator$ biosimilare)$ biosimilare$
Se,mana$ D$ WkD16$ WkD8$ Wk0$ Wk+8$
N.$pazien1$ 32$ 25$ 31$ 32$ 25$
PCDAI$medio$ 48$(53;$2,5–65)$ 7$(3,8;$0–30)$$ 5,9$(2.5;$0–30)$$ 8,5$(5;$0–35)$ 7,5$(5;$0–23)$
(mediana;$
range)$
PCR$ 5,1$(1,1;$0–65)$ 1,5$(0,3;$0,1D20)$ $$ 1,2$(0,4;$0–23)$ $$ 1,2$(0,35;$0–19)$ 0,6$(0,4;$0–2,1)$
VES$ 28$(23;$3–80)$ 13$(7;$2–66)$ $$ 15$(10;$2–59)$ $$ 14$(9;$2–63)$ 13$(8;$1–55)$
Piastrine$ 391$(298;$169– 306$(298;$156– 302$(294;$171–654)$$ 304$(282;$183–804)$ 305$(309;$175–529)$
630)$ 543)$
Hb$ 12$(12.3;$10,3– 13,3$(13.1;$11,6– 13,2$(12.8;$10,3– 13,1$(13,4;$10,4– 13,3$(13,3;$11,4–15,1)$
14,4)$ 16,7)$ 15,6)$$ 16,4)$! P314 Biosimilar infliximab in inflammatory bowel diseases: first interim
Results from a prospective nationwide observational cohort
! Methods: A prospective, nationwide, multicentre, observational cohort was designed to examine the safety
and efficacy of CT-P13 infliximab biosimilar in induction and maintenance of remission in Crohn's
disease (CD, 108 weeks follow-up) and ulcerative colitis (UC, 54 weeks follow-up). Demographic data were
prospectively collected at inclusion and a harmonized, tight monitoring strategy was applied in terms of
clinical scores (CDAI, PDAI, MAYO/pMAYO each visit), biochemical markers (incl. CRP, at least every 3
months) and endoscopic/imaging (at least every 12 months) as requested by the National Health Fund.
Sera is collected for drug through and antibody measurement at 0, 12, 24 and 52 weeks. Safety data was
meticulously registered during follow-up
! Results: 90 consecutive IBD patients were included in the present cohort (57 CD patients (27 males) and
33 UC patients (16 males)) Age at disease onset was 26.0 (SD:10.9) years in CD and 30.5 (SD:14.1) years in
UC. In CDileocolonic and perianal disease was present in 40.4% and 37.5%, respectively. 55.2% of UC
patients had extensive colitis. 21.4% of CD patients had previous surgery. In CD and UC, 60.4%/50% and
55.2%/74.2% of patients received concomitant immunosuppressives and steroids, while 30.4% of CD and
16.1% of UC patients received previous anti-TNFs. At induction, mean CDAI was 289(SD:107), while
MAYO/pMAYO scores were 8.8(SD 3.1) and 6.4(SD 2.6) in UC. There was a significant decrease in CDAI
after 2 and 6 weeks of treatment compared to baseline p! P430 Assessment of safety and efficacy of biosimilar infliximab in children
with Crohn disease: a preliminary report.
! Methods:A total of 12 children diagnosed and treated at 3 Polish hospitals with Crohn disease who started
therapy with BI were assessed. Patients received BI 5 mg/kg at weeks 0, 2, and 6. Pediatric Crohn disease
activity index (PCDAI) and laboratory values (CRP, ESR, platelet count) were assessed at qualification
for the biological treatment and after induction treatment at week 10. Due to small number of cases,
median and range of clinical values are reported for descriptive purposes only.
! Results: Median age was 15.1 years (range 2-18). At BI start median PCDAI was 52.5 (range 5-65); CRP,
ESR, platelet count values were 0.9 mg/dL (0.15-6.4), 18 mm (10-93), 327x109/L (235-602x109),
respectively. Five out of 12 patients were previously treated with a biologics (4 with reference infliximab, 1
with adalimumab). Time of previous treatment was 6-59 months with biologic-free interval of 7-72
months. Treatment was discontinued in 2/12 patients (17%) after first BI dose due to lack of response,
accompanied by adverse event in one patient and withdrawal of consent in second patient. In 10/12
patients (83%) response was observed as assessed by significant PCDAI and inflammation markers
decrease. As of November 2014, 6 out of 12 patients (50%) received all 3 induction doses. For those
patients, median initial PCDAI was 52.5 (15-62.5) and decreased to 5 (2.5-10) . Before treatment and at
week 10 CRP, ESR and platelet count were 1.0 (0.15-6.4), 28 (16-93), 309x109 (255-553) and 0.2
(0.04-0.82), 16 (8-29), 263x109 (220-340), respectively. Adverse events during infusion were observed in
2/12 patients (17%) : one anaphylactic reaction leading to treatment discontinuation and one blood
pressure rise that resolved after infusion rate lowering. In the latter case patient received all 3 doses of BI.
! Conclusion: In this preliminary report BI appears to be safe and efficacious in inducing remission in
Crohn disease paediatric patients. No unexpected safety and product quality issues were identified! DOP078. Are IBD specialists aware of biosimilar monoclonal antibodies?
Results from a survey among ECCO members
! Methods: A 15-question anonymous web survey was conducted with the logistic support of ECCO.
Randomly selected ECCO members were invited by to participate. Information on gender, job position,
country and mAb experience were collected.
! Results: Of 272 responders, 69% worked in a University Hospital, 33% as consultants, 88%
autonomously prescribe mAb for >2 years. Two thirds were aware that biosimilar mAbs are not the same
molecules as their originators (69%) and agreed that biosimilars should carry distinct International
Nonproprietary Names. Most responders regarded cost-sparing (89%) as the main advantage of
biosimilars, immunogenicity (69%) as their main concern, and estimated that post-marketing
pharmacovigilance, well-designed RCT and further study of risk profile were needed (54%, 66%, 63%
resp.). For prescription, 85% disagreed with automatic replacement of the originator with a biosimilar by
a pharmacist, although 18% would support substitution for new prescriptions. Most clinicians thought
that medical societies should promote information about biosimilars (median 66%), collaborate with
health institutions to develop rules (78%) and guidelines (57%) on the use of biosimilars, and create
multispecialty safety registries (80%). Most responders (73%) thought that patient organizations should
be involved in these processes. Only 6% of responders thought that the originator and biosimilar mAb
were interchangeable, although 28% would replace scheduled originator therapy with a biosimilar. If
equivalence was shown by RCTs in IBD, 49% of responders thought a biosimilar should be first choice
because of costs, although 27% thought the savings would be marginal. Most (63%) felt little or not
confident in the use of biosimilar mAb.
! Conclusion: IBD specialists are generally informed on biosimilars, but think they are not interchangeable
with the originator, unless strong evidence is shown about similarity for each indication. Most clinicians
do not feel confident on the use of biosimilars in clinical practice.! P505 Biosimilar but not the same
– Methods: In this descriptive study, 14 consecutive patients who were commenced on Inflectra
from January to July 2014 are compared to 22 consecutive patients commenced on Infliximab
(Remicade) from Dec 2011 to Dec 2013. A direct comparison and statistical analysis was
performed investigating surgery rates, readmission rates, use of steroids, disease activity and
CRP trends.
– Results: Demographics of both patient cohorts were comparable.
29% of patients in Inflectra group required surgery versus 0% in the Inflixiamb group (p= 0.02).
80% of the inflectra group required hospital readmission versus 5% of the infliximab (remicade)
group. (p=0.00004).
60% of patients in the Inflectra group needed steroid augmentation of standard steroid tapering
protocol with 50% requiring multiple increases in steroid dose versus 8% of patients in the
Infliximab (p-value = 0.0007).
Over the course of 8 weeks, 93% of patients in the Inflectra group had an increase in CRP with 7%
remaining unchanged whereas 100% of patients in the infliximab group had a decrease in CRP
(p=! P565. An experience of anti-TNF biosimilar, CT-P13 use: clinical efficacy,
safety and interchangeability in inflammatory bowel disease; a pilot study
! Methods: A total of 17 subjects, who were diagnosed with ulcerative colitis (UC) or Crohn's disease (CD)
and were administered CT-P13 from November 2012 to October 2013 at Dongguk University Ilsan
Hospital, were retrospectively enrolled. We analyzed medical records including the patients'
characteristics, previous history of anti-TNF administration, response and remission to this biosimilar,
disease flare-up and adverse drug reaction (ADR).
! Results: Male to female ratio was 1.8. Mean age was 35.4 years (range, 15 to 57). Patients with UC was 9
cases and those with CD was 8 cases. Mean number of CT-P13 administrations was 4.2±1.9. The induction
treatments in 4 UC and 2 CD patients was done. Clinical response and remission at 8 week were achieved
in 4 (3 UC, 1 CD) and 3 patients (3 UC). One UC patient experienced severe skin rash and was
discontinued with CT-P13. One CD patent did not respond to CT-P13. Twelve patients in maintenance
with originator, were interchanged with CT-P13. Eleven patients experienced no ADR or loss of response
during study period. In one CD patient, disease flare-up was observed.
! Conclusion: CT-P13 may have biosimilarity and interchangeability with its originator in IBD. Large,
randomised, double-blind, prospective study about this issue is needed! P540 Efficacy and safety of infliximab's biosimilar (REMSIMA)
for IBD
! Methods: This was a retrospective multicenter study including IBD patients who received at least one
Remsima infusion. Both anti-TNF naïve patients and patients who switch from Remicade or Humira to
Remsima were included. Short- term clinical outcomes and adverse events of Remsima were evaluated.
! Results: A total of 55 Crohn's disease (CD) patients (23 anti-TNF naïve patients and 32 patients who
switch to Remsima) and 51 ulcerative colitis (UC) patients (41 anti-TNF naïve patients and 10 patients
who switch to Remsima) were included. In anti-TNF naïve CD patients, the rates of clinical response and
remission were 91% and 78% at week 8. In anti-TNF naïve UC patients, the rates of clinical response,
clinical remission, and mucosal healing were 87%, 31%, and 54% at week 8. Three patients (2.8%)
discontinued Remsima because of an adverse event. The efficacy of Remsima was maintained in 86% of
patients with CD and in 67% of patients with UC after switching from Remicade.
! Conclusion: Remsima showed an excellent short-term clinical response and a good safety in both
moderate to severe CD and UC. Further prospective studies with long-term follow up are needed to
confirm the efficacy of Remsima! P137 5 year budget impact analysis of CT-P13 (Infliximab) for the
treatment of Crohn's Disease in UK, Italy and France
! Methods: We aimed to evaluate the cost benefits of the introduction of CT-P13 (infliximab) in treatment
of Crohn's disease from the payer and the patient perspectives by using an Excel based budget-
impact model over a five-year time horizon. The model calculated patients eligible for infliximab
treatment based on the prevalence of Crohn's disease, total population, and annual population
growth rate in 3 major EU countries; UK, Italy, and France. The acquisition cost of comparator
infliximab was assumed not to change after the introduction of biosimilar mAb. The price of the CT-P13
(infliximab) is currently unknown, therefore three different discount scenarios (10%, 20%, and 30%)
were applied to evaluate the budget impact. Market uptake growth was also varied in each of the
scenarios at 20%, 30%, and 40%, respectively. The market share was assumed to be 25% in the first
year in all scenarios
! Results: The total budget saving for the 10% price discount scenario for all three countries throughout
the years 2015, 2016, 2017, 2018, and 2019 was 10,210,000, 12,240,000, 14,730,000, 17,670,000, and
21,220,000 euros, respectively. The total budget saving for the 20% price discount scenario throughout
the years 2015, 2016, 2017, 2018, and 2019 was 20,420,000,26,560,000, 34,570,000, 44,930,000, and
58,440,000 euros, respectively. The total budget saving for the 30% price discount scenario across the
years 2015, 2016, 2017, 2018, and 2019 was 30,640,000, 42,900,000, 60,120,000 84,180,000, and
117,890,000 euros, respectively. The total budget saving over the five year period (2015 -2019) for all three
countries was 76,070,000, 184,920,000, and 335,730,000 euros for the 10%, 20%, and 30% price discount
scenarios, respectively.
! Conclusion: The introduction of the CT-P13 (infliximab) as a treatment option for patients with
Crohn's disease could achieve substantial cost savings. In the scenarios tested, the total 5 year
saving across UK, Italy and France ranged from 76 million to 336 million eurosP137
L'introduzione$di$IFX$biosimilare$come$opzione$di$traAamento$per$i$pazienB$con$malaCa$
di$Crohn$potrebbe$generare$risparmi$considerevoli$per$il$SSN.$Negli$scenari$esaminaB,$il$
risparmio$totale$a$5$anni$in$Regno$Unito,$Italia,$Francia$varia$da$76$a$336$milioni$di$Euro$
IFX$ biosimilare$ 120%$ vs$ $ IFX$
originator$
Risparmio$2015$D$2019:$$
€$20.420.000$–$58.440.000$
Anno$1$ Anno$2$ Anno$3$ Anno$4$ Anno$5$
(2015)$ (2016)$ (2017)$ (2018)$ (2019)$
IFX$ biosimilare$ 130%$ vs$ $ IFX$
originator$
Risparmio$2015$–$2019:$
€$30.640.000$–$117.890.000$
Anno$1$ Anno$2$ Anno$3$ Anno$4$ Anno$5$
(2015)$ (2016)$ (2017)$ (2018)$ (2019)$
1.J. Kim et al, 5 Year Budget Impact Analysis of Biosimilar Infliximab for The Treatment of Crohn’s disease in UK, Italy and France, Presented at the 10th Congress of
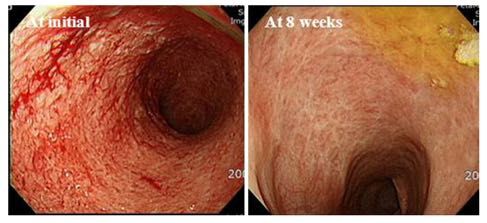
ECCO Spain, Poster No.137! P603 Efficacy of the new infliximab biomarker CT-P13 induction therapy
on mucosal healing in ulcerative colitis patients.
! Methods: Patients diagnosed with UC, who were administered CT-P13 from June 2014 at the First
Department of Medicine, University of Szeged, were prospectively enrolled. Medical records analyzed
included patients' characteristics, previous history of infliximab administration, response to CT-
P13, concomitant medications, and adverse drug reaction. Serum activity markers, trough levels and
antibody titers have been measured. Sigmoideoscopy was performed at the end of the induction therapy
in patients who agreed.
! Results: Twelve UC patients were treated with CT-P13 between June and November 2014 at our centre.
The indication of the therapy was acute, severe flare up and chronic, refractory activity in 6-6 patients.
Male-female ratio was 5:7. Mean age was 34 years (range 20-68). Induction treatments have been done in
9 patients until now. Two patients discontinued the therapy after the second infusion: one, who was
previously treated with infliximab and developed high antibody level, because of hypersensitivity reaction
and one because of septic complications. Clinical response and remission at week 6 were achieved in 2 and
5 patients. Two patients did not respond to CT-P13 at week 6 (one previously treated with infliximab).
Sigmoideoscopy was performed in 9 of the 12 patients. Severe activity was detected in 2 patients; one of
them discontinued the therapy after the 2nd infusion and the other did not show response at week 6.
Seven patients (four with eMayo score of 1 and three with eMayo score of 0) showed mucosal healing at
the end of the induction therapy.
! Conclusion: This was the first study examining the efficacy of CT-P13 induction therapy on mucosal
healing in UC. CT-P13 induction therapy showed clinical response and remission in 58% of the UC
patients. Mucosal healing was revealed in 78% of the patients during or after the induction therapy.
Although the number of the enrolled patients is not so high yet, our results indicate that the induction
with CT-P13 can result mucosal healing in similar proportion as the originator infliximabOur survey showed that most IBD experts have a good understanding of the definition of biosimilars. However, there is still a proportion of IBD specialists with a misconception of these molecules, viewing them as “generic” copies of original biological agents, or as additional follow-on agents of the class of their originators. Biosimilars are expected to be cost-sparing for 90% of respondents, but only half of them believe in a significant reduction in healthcare costs, and 15% remain dubious on this aim. Immunogenicity remains the major concern for the majority of respondents, who claim due to this reason for pharmacovigilance and postmarketing measures to monitor equivalence in terms of safety of biosimilars compared with originator. This monitoring demand that the nomenclature allows for each biosimilar to be distinguished from its originator, by carrying distinct International Nonproprietary Names, by an accurate postmarketing pharmacovigilance for each product, and by well-designed trials with validated endpoints in each medical specialty is also required. The majority of responders expect a primary role for medical societies to improve knowledge, to develop appropriate guidelines and pharmacovigilance registries, and to collaborate with patients’ association to clarify unmet needs in the use of biosimilars. Extrapolation of data across indications and interchangeability between biosimilar and originator remain key issues. The majority of respondents are reluctant to accept data from clinical trials conducted in rheumatologic indications as valid for IBD and wish to base their opinion on disease-specific evidence. Similarly, less than 10% would replace the originator with a biosimilar for a patient already under treatment, while 25% would consider interchangeability only for new prescriptions. At the moment, confidence in prescribing biosimilars in IBD remains low among clinicians, although they seem to be adequately informed. IBD-specific data on the comparison for efficacy, safety, and immunogenicity are thus urgently needed.
Dati futuri sulle IBD $ (studi in corso) $ $
4) Conclusioni " In Italia la posizione dell’AIFA chiarisce che i medicinali biologici e biosimilari non possono essere considerati sic et simpliciter alla stregua dei prodotti equivalenti, escludendone quindi la vicendevole sostituibilità terapeutica automatica. Proprio perché i medicinali biologici di riferimento ed i biosimilari sono medicinali simili, ma non identici, l’AIFA ha deciso di non includere i medicinali biosimilari nelle liste di trasparenza che consentono la sostituibilità automatica tra prodotti equivalenti. " Di conseguenza, la scelta di trattamento con un farmaco biologico di riferimento o con un biosimilare rimane una decisione clinica affidata al medico specialista prescrittore. $ $
Puoi anche leggere