LE POLMONITI NELL'ANZIANO - 11 MAGGIO 2018 ANDREA CRUCITTI GRUPPO DI RICERCA GERIATRICA, BRESCIA JOURNAL CLUB - GRG
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
LE POLMONITI
NELL’ANZIANO
11 maggio 2018
Andrea Crucitti
Gruppo di Ricerca Geriatrica, Brescia
Journal Club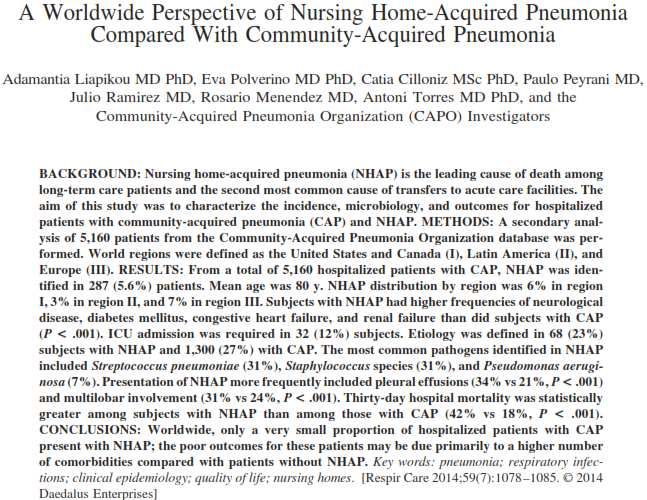
POLMONITE Reazione infiammatoria del parenchima polmonare ad agenti infettivi

DIAGNOSI
Comparsa o peggioramento di un infiltrato
polmonare ad esame radiologico
+
Evidenza della sua origine infettiva:
- Febbre di nuova insorgenza
- Espettorato purulento
- Leucocitosi
- Desaturazione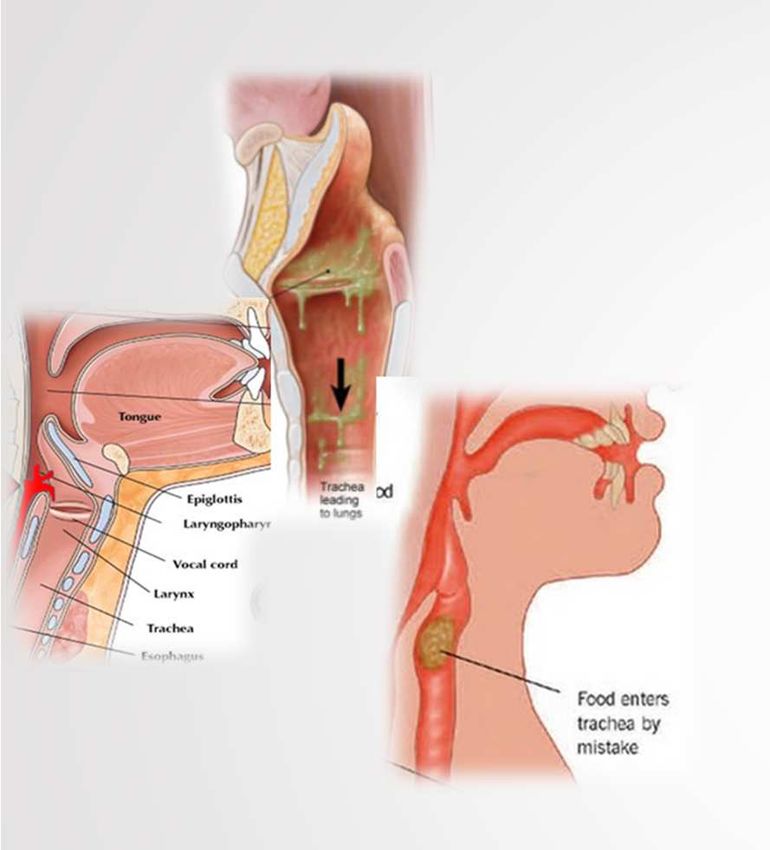
RX TORACE
- Opacità/addensamenti localizzati o multipli o
consolidamento lobare (forme batteriche tipiche)
- Infiltrati interstizio-alveolari, anche
bilaterali (forme batteriche atipiche e virali)
ATTENZIONE!
Comparsa di reperti più tardivi in pazienti anergici,
neutropenici, etilisti, IRC, diabetici (ripetere RX a 24-48 ore)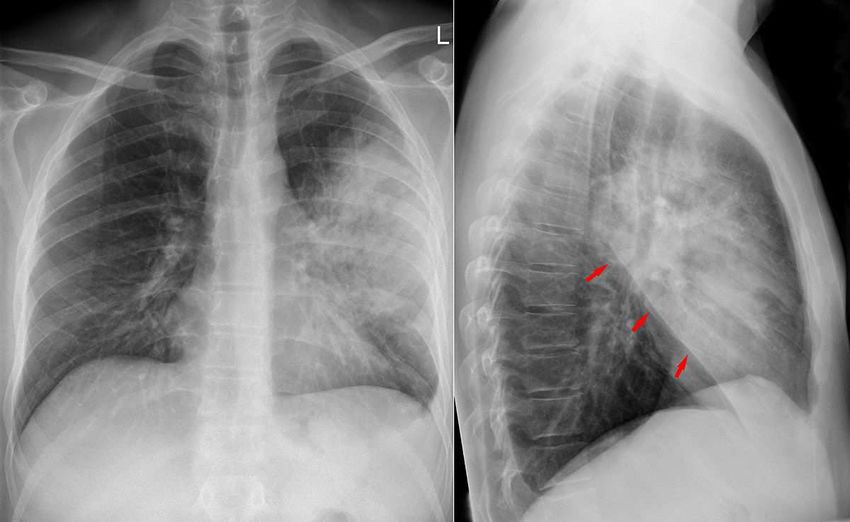
QUALI ACCERTAMENTI?
SATURIMETRIA
Desaturazione periferica
EMOGASANALISI ARTERIOSA
PARAMETRI VITALI
FC, FR, PA, ECG, TC
ESAMI EMATOCHIMICI
Emocromo con formula, PCR, funzionalità renale ed epatica,
elettroliti
CLASSIFICAZIONE
Polmonite acquisita in comunità (CAP)
Esordio in un paziente non ospedalizzato o entro 48 h dal
ricovero
Polmonite nosocomiale (HAP)
Esordio o peggioramento di un infiltrato polmonare dopo
almeno 48 h dal ricovero
(Se esordio dopo 48 h dall’inizio della ventilazione meccanica – VAP)
HCAP – NHAP …
LE POLMONITI
NELL’ANZIANO
Come "invecchia"
l’apparato respiratorio
Janssens JP, Krause KH. Lancet Infect Dis. 2004; 4: 112-24

CON L’INVECCHIAMENTO CAMBIA LA MECCANICA RESPIRATORIA:
A) Ridotta elasticità del polmone (alterazioni nel parenchima polmonare:
aumento del diametro alveolare, "enfisema senile", diminuzione del
diametro delle piccole vie aeree)
B) Ridotta compliance della parete toracica (irrigidimento della parete,
alterazioni strutturali della gabbia toracica e cambiamenti nella forma del
torace con cifosi dorsale e aumento del diametro antero-posteriore –
conseguenze di osteoporosi e fratture vertebrali)
C) Ridotta forza dei muscoli respiratori (stato nutrizionale, sarcopenia)
CONSEGUENZE:
A) ↑ Capacità Funzionale Residua, ↓ Volumi Espiratori Forzati e Picco di
Flusso Espiratorio
B) Aumento del lavoro di respirazione
C) Disfunzione dei muscoli respiratori che, in corso di polmonite, può portare
a ipoventilazione e insufficienza respiratoria ipercapnica
Janssens JP, Krause KH. Lancet Infect Dis. 2004; 4: 112-24
INOLTRE, NELL’ANZIANO SI OSSERVA:
- Tosse meno efficace
- Inefficace clearance delle secrezioni delle vie aeree
- Minore sensibilità dei centri respiratori all'ipossia o
all'ipercapnia
→ diminuita e ritardata risposta ventilatoria in caso di
malattia acuta
↓ RISERVA FUNZIONALE
l'apparato respiratorio rimane in grado di mantenere un
adeguato scambio di gas durante l'intera vita, a meno
di patologie acute che lo colpiscono…
INSUFFICIENZA RESPIRATORIA ACUTA
Janssens JP, Krause KH. Lancet Infect Dis. 2004; 4: 112-24Meyer KC. Semin Respir Crit Care Med 2010;31:561–574
LE POLMONITI NELL’ANZIANO Epidemiologia
INCIDENZA
CAP. Dopo i 65 anni, 25–44 casi per 1000 persone l’anno (maggiore
di 4 volte che nei pazienti < 65 anni).
RSA. 33-114 casi per 1000 persone l’anno, ed aumenta con l’età.
MORTALITÀ:
Tassi di mortalità tra gli anziani ricoverati per CAP > 30%.
Per polmoniti acquisite in RSA, la mortalità può raggiungere il 57%.
Janssens JP, Krause KH. Lancet Infect Dis. 2004; 4: 112-24UO MEDICINA
Periodo 2015-2016
Nr totale pazienti: 1549
Polmonite No polmonite
Nr pazienti 353 (22.8 %) 1196 (77.2 %)
Età media, aa 81.98 0.025 80.1
Degenza media, gg 11.7 0.000 9.7
Sesso, F (%) 54.1 % 59 %
Mortalità, in Osp. 19 % 0.000 8.8 %
Dimesso a casa 54.7 % 67.6 %
Riab. 9.1 % 6.2 %
RSA 7.9 % 9.4 %Clinical Infectious Diseases 2017;64(11):1486–93
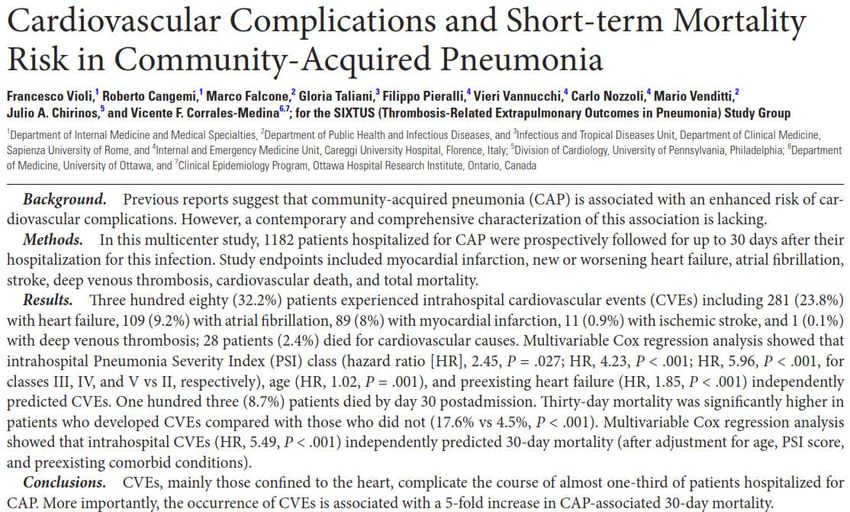
CVEs complicate a substantial
proportion of hospitalized CAP
cases and that their occurrence
significantly increases the mortality
associated with this infection.
This suggests that CAP should be
regarded not only as a disease
limited to the lung but also as a
systemic illness that commonly
and negatively affects the
cardiovascular system.
Clinical Infectious Diseases 2017;64(11):1486–93Factors associated with 30-day readmission in
patients hospitalized with CAP
PREVENTABLE FACTORS
Thirty-day readmission post-discharge is usually used as an
indicator of vulnerability.
- Influenza and pneumococcal vaccination
- Use of hospital care protocols
This study shows that 11.39% of patients aged ≥ 65 years initially
- Discharge planning and postdischarge follow-up (adequate
hospitalized for CAP were readmitted within 30 days after
discharge planning, including patient stability and destination, has
discharge.
been associated with reduced readmission)
Rehospitalization was associated with preventable and non-
NON-PREVENTABLE FACTORS
preventable factors.
- Initial severity of CAP
- Individual patient characteristics (age, sex, socioeconomic status,
education and comorbidities)
Toledo D, et al. BMJ Open 2018;8:e020243CAP-unrelated causes - 49.5% of readmissions
Comorbidities in 91% of readmitted patients
The reason for readmission is generally destabilization of comorbidities.
Pneumonia often occurs in patients with underlying comorbidities and
often results in a worsening of such underlying conditions.
Toledo D, et al. BMJ Open 2018;8:e020243Gait speed and walking abilities may be used as clinical indicators of frailty in older subjects. Functional status can predict clinical outcomes (e.g. clinical recovery, re-hospitalization and mortality), and is considered a clinical outcome itself; its deterioration can be triggered by an acute illness, such as pneumonia. In-hospital mortality depends not only on the severity of the acute illness and age, but also on preexisting conditions, such as loss of functional independence, severe and moderate cognitive impairment and low body mass index. Therefore, we suggest screening all elderly patients for the presence of delirium and acute mobility impairment both on admission and systematically during the hospitalization.
Davydow S, et al. Am J Med. 2013 ; 126: 615–624.e5
LE POLMONITI
NELL’ANZIANO
Caratteristiche clinicheSEGNI E SINTOMI DELLA POLMONITE
• DOLORE TORACICO
(pleuritico)
• TOSSE
• DISPNEA
• FEBBRE
• LEUCOCITOSI
Eur J Intern Med. 2014; 25: 312-319SEGNI E SINTOMI DELLA POLMONITE
NELL’ANZIANO
• •DOLORE
CADUTE TORACICO
•(pleuritico)
CAMBIAMENTO ACUTO
• TOSSE
DELLO STATO FUNZIONALE
• •DISPNEA
INAPPETENZA
• •FEBBRE
INCONTINENZA URINARIA
• •LEUCOCITOSI
CONFUSIONE/DELIRIUM
Eur J Intern Med. 2014; 25: 312-319CAP COULD BE A DIFFERENT ENTITY IN THE ELDERLY BECAUSE OF AN ATYPICAL
CLINICAL PRESENTATION, MORE SEVERE SYMPTOMS AND HIGHER LONG-TERM
MORTALITY IN COMPARISON TO YOUNGER PATIENTS
7.803 patients with CAP
Comorbidity present in
only half of the younger
patients
(46.6% versus 88.2%)
Eur Respir J. 2012; 39: 1156-1161POLMONITE AB-INGESTIS
La polmonite ab-ingestis (aspiration
pneumonia) è definita come una polmonite in
un individuo con fattori di rischio per
aspirazione (alimentare o di secrezioni
orofaringee) nelle vie aeree inferiori, con
episodio di aspirazione dimostrato o
sospettato.
Maggiore severità clinica e tasso di mortalità.
MAGGIORE PROBABILITÀ SE: riscontro radiografico di addensamenti polmonari
in segmenti declivi dove per anatomia e gravità è più facile il passaggio di
secrezioni o residui alimentari:
- nel caso di pazienti allettati, i segmenti posteriori dei lobi superiori e i
segmenti superiori dei lobi inferiori;
- in generale i lobi inferiori, soprattutto a destra.POLMONITE AB-INGESTIS
Circa 50% di tutti gli adulti sani aspirano piccole quantità di secrezioni
orofaringee durante il sonno.
FATTORI PROTETTIVI FATTORI PREDISPONENTI
- bassa carica batterica delle - colonizzazione oro-faringea
secrezioni; - ridotta clearance muco-ciliare;
- valido riflesso della tosse; - alterata funzione orale e
- adeguata funzione muco- neurologica;
ciliare; - alterata meccanica
- normali meccanismi respiratoria;
immunitari - comorbilità
Alta incidenza di aspirazione silente negli anziani con polmonite: 71% dei
pazienti anziani con CAP.
Janssens JP, Krause KH. Lancet Infect Dis. 2004; 4: 112-24Distinguishing anaerobic pleuropneumonia due to aspiration from
classic CAP may be very difficult.
Absence of shaking chills and the development of lung abscess are
features more common in aspiration pneumonia. Aspiration
pneumonia has a more indolent course (slightly longer time before
presentation to the hospital, 4.5 vs 2.6 days).
Journal of Critical Care. 2015; 30 : 40-48POLMONITE AB-INGESTIS
Una maggiore frequenza di aspirazione si riscontra nei pazienti con
demenza e con patologia cerebrovascolare
L’ultilizzo di presidi per nutrizione enterale non protegge dalla
broncoaspirazione (SNG, PEG, PEJ)
La flora batterica orale negli anziani più fragili può diventare più
virulenta
Potenziali patogeni respiratori che colonizzano il cavo orale sono
Staphylococcus aureus (24.5%), Klebsiella pneumoniae (18.1%),
Pseudomonas aeruginosa (18.1%) e Enterobacter cloacae (11.6%)
Sumi Y, et al - Arch Gerontol Geriatr 2007; 44: 119–124
Janssens JP, Krause KH. Lancet Infect Dis. 2004; 4: 112-24La colonizzazione batterica del tratto respiratorio superiore più che all’età si
correla alla gravità delle condizioni cliniche.
Colonizzazione da parte di batteri Gram-negativi può riguardare il 60-73% dei
pazienti anziani in un reparto di Medicina e il 22-37% di quelli istituzionalizzati.
FATTORI FAVORENTI COLONIZZAZIONE VIE RESPIRATORIE
• Terapie antibiotiche
• Intubazione endotracheale
• Fumo
• Malnutrizione
• Interventi chirurgici
• Ridotta salivazione (da farmaci, ad es. antidepressivi, antiparkinsoniani,
diuretici, antipertensivi e antistaminici)
• Malattie/Igiene cavo orale
Nei pazienti istituzionalizzati il rischio di polmonite è ridotto da un'adeguata
igiene orale (e negli individui edentuli).
Janssens JP, Krause KH. Lancet Infect Dis. 2004; 4: 112-24POLMONITE AB-INGESTIS
Eur J Intern Med. 2014; 25: 312-319POLMONITE NOSOCOMIALE La diagnosi di polmonite nosocomiale (Hospital-acquired pneumonia – HAP) in età molto avanzata è spesso difficile a causa di presentazioni cliniche atipiche e paucisintomatiche (delirium, mancata risposta febbrile, tosse assente, esame obiettivo scarsamente suggestivo). Talvolta la diagnosi viene formulata in seguito ad approfondimenti richiesti in presenza di cambiamenti non altrimenti giustificati nelle prestazioni cognitive, peggioramento di patologie croniche, nuova comparsa di dispnea, tachipnea, tachicardia, ridotta saturazione di ossigeno arteriosa.
EPIDEMIOLOGIA HAP-VAP
EZIOLOGIA E FATTORI DI RISCHIO
Respiratory Care. 2014; 59: 1078-1085
Many studies have attributed these findings to a nosocomial etiology.
Further investigation on microbial composition and MDR infections
risk factors of HCAP are needed
Semin Respir Crit Care Med 2009; 30: 239–248LE POLMONITI NELL’ANZIANO In Pronto Soccorso…
PNEUMONIA SEVERITY INDEX FOR COMMUNITY-ACQUIRED PNEUMONIA
Scores and models can help the identification of the most adequate setting of
care for patients with CAP,
BUT
objective criteria should always be supplemented with physician evaluation of
subjective factors when deciding the setting of care, including:
- the ability to safely and reliably take oral medication;
- availability of outpatient support resources and caregivers in case of
dependent patients;
- other medical or psycho-social needs (such as homelessness and poor
functional status);
- lack of response to previous adequate empiric antibiotic therapy.
Three possible scenarios must be taken into account when evaluating the
severity of a patient with pneumonia:
1) onset of severe sepsis;
2) onset of acute respiratory failure;
3) presence of decompensated comorbidities.
Clinical Infectious Diseases 2007; 44: S27–72ICU ADMISSION DECISION
• Direct admission to an ICU is required for patients with
septic shock requiring vasopressors or with acute
respiratory failure requiring intubation and mechanical
ventilation
• Direct admission to an ICU or high-level monitoring unit
is recommended for patients with 3 of the minor criteria
for severe CAP
Clinical Infectious Diseases 2007; 44: S27–72In some studies, a significant percentage of patients with CAP are
transferred to the ICU in the first 24–48 h after hospitalization.
Mortality and morbidity among these patients appears to be
greater than those among patients admitted directly to the ICU.
Clinical Infectious Diseases 2007; 44: S27–72Acute respiratory failure can be treated with different levels of
intensity of care, including non-invasive ventilation (NIV) and
mechanical ventilation (MV).
However, despite the lack of evidence that these mechanisms of
support are less effective in elderly patients, they are often
undertreated in clinical practice.
Elderly patients (>75 years) had a similar duration of MV, ICU and
hospital stay, and in-hospital mortality (38% vs. 31%), but lower cost of
care when compared to younger patients.
It does not seem appropriate to restrict intensive care and ventilatory
support only on the basis of chronologic age.LE POLMONITI NELL’ANZIANO Terapia
DIAGNOSI EZIOLOGICA:
(SE CAP SEVERA, RICOVERO IN ICU o COMORBIDITÀ)
- Coltura dell’espettorato/tracheoaspirato/BAL
- Emocolture se febbre
- Antigeni urinari per Pneumococco e Legionella
- Sierologie per Chlamydia spp. e Mycoplasma
pneumoniae (++ se infiltrati interstizio- alveolari)
NB. Avviare antibiotico-terapia dopo esecuzione di
emocolture e raccolta di campioni microbiologiciE l’antibiotico?
Polmonite acquisita in comunità (CAP)
Esordio in un paziente non ospedalizzato o entro 48 h dal
ricovero
Polmonite nosocomiale (HAP)
Esordio o peggioramento di un infiltrato polmonare dopo
almeno 48 h dal ricovero
Polmonite associata alla ventilazione (VAP)
Esordio dopo 48 h dall’inizio della ventilazione meccanicaClinical Infectious Diseases 2007; 44: S27–72 Clin Microbiol Infect 2011; 17(Suppl. 6): E1–E59
Terapia empirica CAP
Per es:
AMOXICILLINA / CLAVULANATO
+
AZITROMICINA
Oppure:
LEVOFLOXACINA
Elevata resistenza pneumococchi
a CIPROFLOXACINA
Clinical Infectious Diseases 2007; 44: S27–72 N Engl J Med 2014;371:1619-28
Clin Microbiol Infect 2011; 17(Suppl. 6): E1–E59Terapia empirica CAP
Clinical Infectious Diseases 2007; 44: S27–72 N Engl J Med 2014;371:1619-28
Clin Microbiol Infect 2011; 17(Suppl. 6): E1–E59Terapia empirica CAP
Clinical Infectious Diseases 2007; 44: S27–72 N Engl J Med 2014;371:1619-28
Clin Microbiol Infect 2011; 17(Suppl. 6): E1–E59DE-ESCALATION
QUANDO ISOLAMENTO e ANTIBIOGRAMMA DISPONIBILE:
Da terapia empirica ad ampio spettro a terapia mirata
Da terapia di associazione a monoterapia
SE PAZIENTE STABILE, IN MIGLIORAMENTO CLINICO
(TC< 37,5 °C, parametri vitali e funzione gastrointestinale normale)
Da terapia endovenosa a terapia per os
DURATA TERAPIA ANTIBIOTICA
- Almeno 5 giorni, fino a 10-14 giorni nelle CAP severe
- Paziente sfebbrato da almeno 48 ore
- Stabilizzazione clinica
NON INDICATO CONTROLLO RADIOGRAFICO A FINE TERAPIAE l’antibiotico?
Polmonite acquisita in comunità (CAP)
Esordio in un paziente non ospedalizzato o entro 48 h dal
ricovero
Polmonite nosocomiale (HAP)
Esordio o peggioramento di un infiltrato polmonare dopo
almeno 48 h dal ricovero
Polmonite associata alla ventilazione (VAP)
Esordio dopo 48 h dall’inizio della ventilazione meccanicaTo minimize patient harm and exposure to unnecessary antibiotics and reduce antibiotic resistance, we recommend that the antibiogram data be utilized to decrease the unnecessary use of dual gram-negative and empiric methicillin-resistant Staphylococcus aureus (MRSA) antibiotic treatment. We also recommend short-course antibiotic therapy for most patients with HAP or VAP independent of microbial etiology, as well as antibiotic de-escalation.
Terapia empirica HAP
Clin Infect Dis. 2016; 63: 575-82Clin Infect Dis. 2016; 63: 575-82
For patients with suspected HAP/VAP, we recommend
using clinical criteria alone,
rather than using serum PCT or PCR or Pulmonary
Infection Score plus clinical criteria,
to decide whether or not to initiate antibiotic therapy
We recommend that all hospitals regularly generate and
disseminate a local antibiogram, ideally one that is
specific to their intensive care population if possible
(empiric treatment regimens guided by the local distribution of
pathogens associated and their antimicrobial susceptibilities).
Clin Infect Dis. 2016; 63: 575-82HEALTHCARE-ASSOCIATED PNEUMONIA (HCAP)
The rationale for inclusion of the HCAP designation with the HAP/VAP
guidelines in 2005 was that patients with HCAP were thought to be at high
risk for MDR organisms by virtue of their contact with the healthcare
system.
THERE IS INCREASING EVIDENCE FROM A GROWING NUMBER OF
STUDIES THAT MANY PATIENTS DEFINED AS HAVING HCAP ARE
NOT AT HIGH RISK FOR MDR PATHOGENS.
Furthermore, although interaction with the healthcare system is potentially
a risk for MDR pathogens, underlying patient characteristics are also
important independent determinants of risk for MDR pathogens.
RECOMMENDATIONS REGARDING COVERAGE FOR MDR
PATHOGENS AMONG COMMUNITY-DWELLING PATIENTS WHO
DEVELOP PNEUMONIA WOULD LIKELY BE BASED ON VALIDATED
RISK FACTORS FOR MDR PATHOGENS
Clin Infect Dis. 2016; 63: 575-82– Cosa prendi per la
tosse?
-Generalmente un po’ di
freddo.Grazie
Puoi anche leggere