Diabete e genere Alberto Maran
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
Diabete e genere Alberto Maran
Prevalenza globale del diabete e proiezioni 2025
33.0
19.2 47.8
36.2
13.8 27.6
42.8 79.5 26.4
3.4 55.9
11.5 9.8
27.3
Mondo 135.286 299.974 +120%
Paesi sviluppati 50.974 72.244 +40%
Paesi in via di sviluppo 84.313 227.725 +170%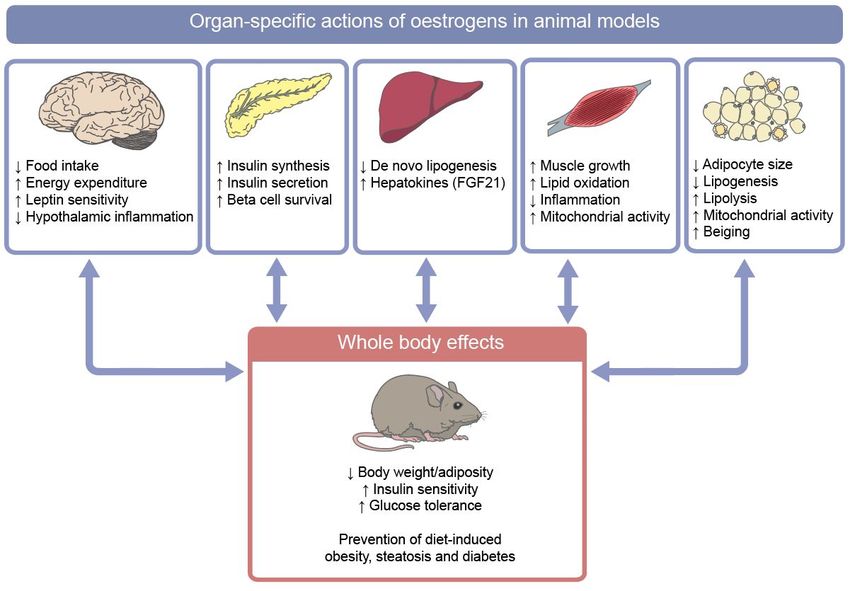
P I D E M I O LO G I A D E L D I A B E T E
Andamento della prevalenza del diabete in Italia nel
Figura 1 corso
Andamento degli
della anni
prevalenza del(2001-2014)
diabete in Italia nelsecondo i da<
corso degli anni ISTAT
(2001-2014) secondo i dati ISTAT (2).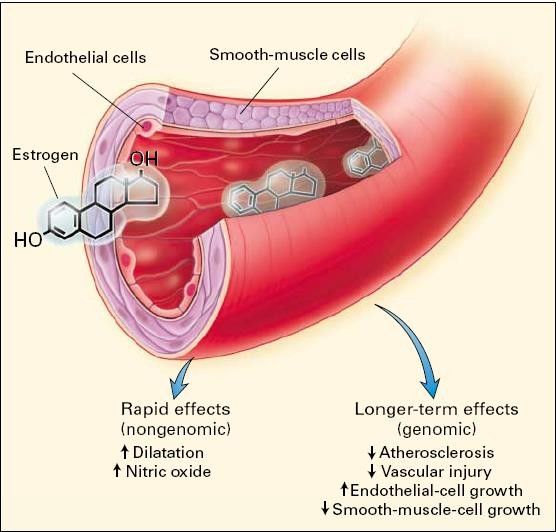
0,2 0,3 0,5
0
0-19 20-34 35-49 50-64 65-79 >=80 Totale
Classi di età
Prevalenza del diabete in funzione del sesso e dell’età
La prevalenza complessiva di diabete è del 6,2%
25
20
Prevalenza (%)
15
Maschi
Femmine
10
5
0
0
4
8
12
16
20
24
28
32
36
40
44
48
52
56
60
64
68
72
76
80
84
88
92
96
100
108
104
Osservatorio Arno Diabete 2018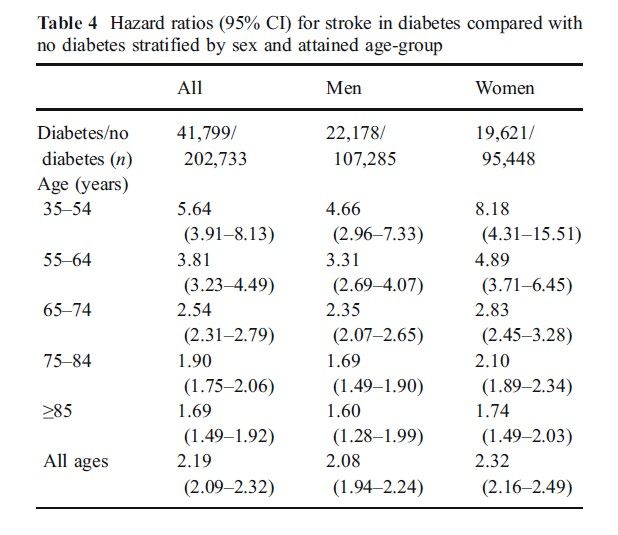
La sindrome Metabolica come «Cluster»
di Fattori di rischio
Obesità Addominale
Intolleranza
Glucosio/Resistenza Insulina
Diabete Ipertensione CVD
Dislipidemia Aterogena
Stato Proinfiammatorio/
Protrombotico
National Cholesterol Educational Program (NCEP), Adult Treatment Panel (ATP) III; 2001
Manuscript Cardiovascular disease, chronic kidney disease, and diabetes
mortality burden of cardio-metabolic risk factors between 1980
and 2010: comparative risk assessment
The Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration
Page 21
Summary
Author Manuscript
Background—Elevated blood pressure and glucose, serum cholesterol, and body mass index
(BMI) are risk factors for cardiovascular diseases (CVDs); some of these factors also increase the
risk of chronic kidney disease (CKD) and diabetes. We estimated CVD, CKD, and diabetes
mortality attributable to these four cardio-metabolic risk factors for all countries and regions
between 1980 and 2010.
Methods—We used data on risk factor exposure by country, age group, and sex from pooled
analysis of population-based health surveys. Relative risks for cause-specific mortality were
obtained from pooling of large prospective studies. We calculated the population attributable
fractions (PAF) for each risk factor alone, and for the combination of all risk factors, accounting
for multi-causality and for mediation of the effects of BMI by the other three risks. We calculated
attributable deaths by multiplying the cause-specific PAFs by the number of disease-specific
Author Manuscript
deaths from the Global Burden of Diseases, Injuries, and Risk Factors 2010 Study. We propagated
the uncertainties of all inputs to the final estimates.
Findings—In 2010, high blood pressure was the leading risk factor for dying from CVDs, CKD,
and diabetes in every region, causing over 40% of worldwide deaths from these diseases; high
BMI and glucose were each responsible for about 15% of deaths; and cholesterol for 10%. After
accounting for multi-causality, 63% (10.8 million deaths; 95% confidence interval 10.1–11.5) of
HHS Public Access
deaths from these diseases were attributable to the combined effect of these four metabolic risk
Authorburden
factors, compared with 67% (7.1 million deaths; 6.6–7.6) in 1980. The mortality manuscript
of high
Lancet Diabetes
BMI and glucose nearly doubled between 1980 and 2010. At the country level, age-standardised Endocrinol. Author manuscript; ava
Author Ma
Published
death rates attributable to these four risk factors surpassed 925 deaths per in100,000
final edited form men
among as: in
Lancet Diabetes Endocrinol. 2014 August ; 2(8): 634–647. doi:10.1
Figure 3. Belarus, Mongolia, and Kazakhstan, but were below 130 deaths per 100,000 for women and below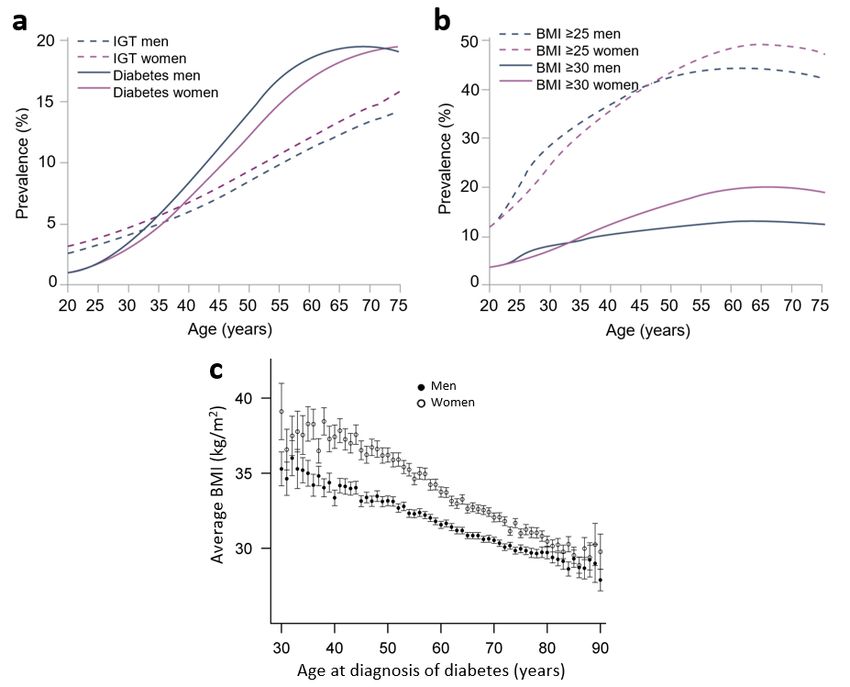
Le evidenze crescenti hanno contribuito a rimuovere fattori di rischio delle donne.
la falsa credenza che le donne fossero più protette dal Tra i dati prodotti e disponibili menzioniamo la pubbli-
rischio CV. cazione delle prime raccomandazioni cliniche specifi-
CAUSE DI MORTE
Questo ha assunto particolare rilievo sul piano epide- che per le donne riguardo alla prevenzione delle malat-
tie CV (American Heart Association 1999).
miologico, diagnostico e di programmazione sanitaria,
per un’aumentata consapevolezza dell’importanza di Un decennio più tardi (2011) fu sempre l’AHA a pubbli-
care lecardiovascolare
Rischio linee guida pereladifferenze
prevenzione delle malattie CV
di genere
una valutazione di genere del rischio CV. In effetti negli
nelle donne che ebbero il merito di porre l’attenzione
2
UOMO
anni passati c’è stata dispersione di risorse e danni in
DONNA
su importanti criticità specifiche del sesso femminile.
La donna infatti presenta alcune variabili ed eventi fi-
siologici della vita riproduttiva, quali la gravidanza e la
menopausa, che rappresentano importanti condizioni
di vulnerabilità per il rischio CV.
La gravidanza, in particolare, è un test di stress CV
Altre Malattia e metabolico che rappresentaAltre un’opportunità
cause, 20% coronarica, 20%
Malattia unica
per valutare il rischio CV nel corso
cause, 20% di coronarica,
tutta la vita.22%
È
importante sapere che la preeclampsia o il diabete ge-
Traumi
Traumi stazionale durante la gravidanza, e/o la nascita di un
e avvelenamenti, 13%
Ictus, 10% e avvelenamenti, 4%
neonato pretermine o di un bambino che è piccolo per
Malattie
la sua età gestazionale, o un sanguinamento nel terzo
Ictus, 15%
respiratorie, 6%
trimestre sono tutti fattori associati a un aumentato ri-
Malattie Altre malattie schio CV. Per questi motivi nelle linee guida troviamo
respiratorie, 7% CV, 12% Altre neoplasie,
raccomandata 10% accurata dell’anamnesi in
la raccolta
Altre neoplasie, 13% relazione alla presenza di complicanzeAltre malattie 3.
in gravidanza
Con la menopausa vengono meno alcuni CV,effetti
15% protet-
Cancro Cancro al seno, 3%
Cancro al polmone, 4% tivi esercitati dagli estrogeni, caratterizzati da:
allo stomaco,
2% Cancro al polmone, 2%
Cancro
Cancro Cancro colo-rettale, 2%
colo-rettale, 2%
allo stomaco, 1%
-
tensina aldosterone (sistema RAA);
FIGURA 1. FIGURA 2.
Mortalità per cause in uomini di tutte le età (da European Mortalità
colesterolo-LDL, riduzione
per cause in deitutte
donne di livelliledietà
LP(a),
(da APO
European
Cardiovascular Disease Statistics, 2012, mod.) . 1
A1 - APO.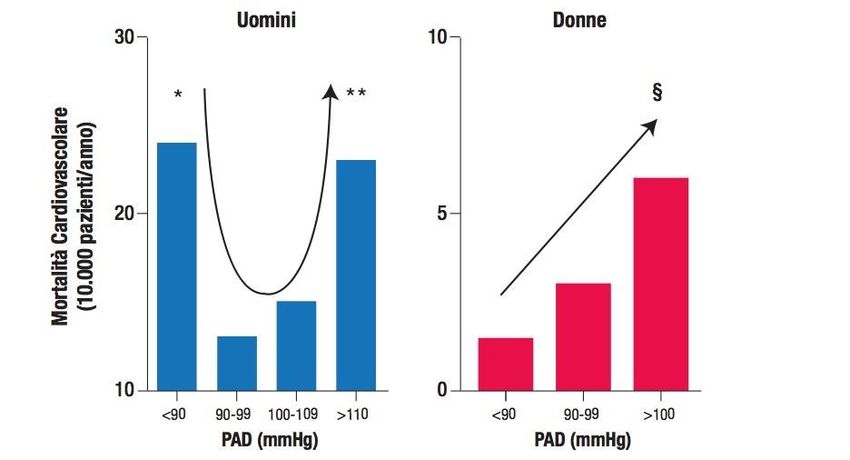
The natural history of non insulin-dependent
diabetes mellitus
Onset of
diabetes
Environmental Complications
factors
nutrition
obesity Disability
physical inactivity
DEATH
Genetic IGT e.g.
susceptibility
Insulin resistence Hyperglycaemia Retinopathy Blindness
Hyperinsulinaemia HDL¯ Nephropathy Renal failure
HDL Atherosclerosis Coronary heart
Neuropathy disease
Amputation
WHO 94390
HDL,high-density lipoprotein; IGT, impaired glucose tolerance
INTERHEART: Risk of Acute Myocardial Infarction
associated with self-reported diabetes
Overall and
Region-by-Region
Odds ratio after adjusting
for age, sex and smoking
Colhoun HM et al. Lancet 2004;364:685-696.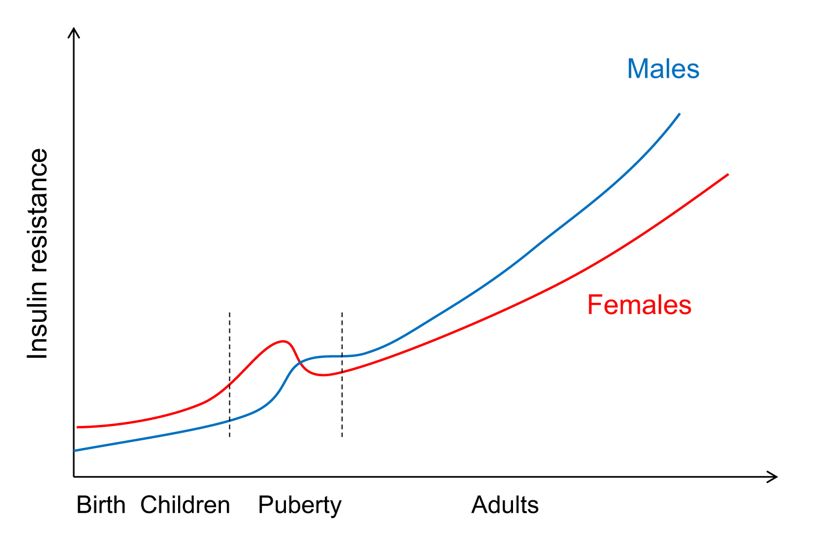
Associa'on of risk factors with acute myocardial infarc'on in men and women a6er
adjustment for age, sex, and geographic region
INTERHEART. Lancet 2004Mortalità cardiovascolare in uomini e donne con diabete
Uomini Donne
60 60
50 Diabete 50
Mortalità per 1000
Mortalità Per 1000
No Diabete 2x
40 40
30 30 4-5x
20 20
10 10
0 0
0-3 4-7 8-11 12-1516-1920-23 0-3 4-7 8-11 12-1516-1920-23
Anni di Durata del follow-up (anni) Anni di durata del follow-up (anni)
Modificata da Krolewski AS, et al. Am J Med 1991 (ref. 19 )Rela
Rela
Sex differences in the effects of
33 Page 4 of 8 diabetes on vascular outcome Curr Diab Rep (2018) 18: 33
Fig. 2 Results from prior meta-analyses of sex differences in the effects of diabetes on vascular outcomes, summarised through the ratios of women-to-
Peters,
men adjusted relative risks (and 95% confidence intervals) pooled across cohort Current Diabetes Reports (2018) 18: 33
studiesLe donne con T2DM hanno anche un aumentato rischio di Stroke Age-adjusted HR for stroke in DM2 subjects vs non diabetic subjects was: - 2.08 (95%CI:1.94-2.24) in men - 2.32 (95%CI: 2.16-2.49) in women. The increase in risk attributable to diabetes was highest - in young women (HR 8.18; 95%CI 4.31-15.51) and decreased with age.
Long-term survival aMer AMI in men and women with diabetes
Crowley et al. Am Heart J 2003PERCHE’ ??? Rispetto all’uomo: 1. La donna è “più complicata” 2. Menopausa ed assetto ormonale 3. La donna vive più a lungo 4. Poco considerata (scientificamente)
La donna è “più complicata”
Possible causes of high CVD in women with diabetes
Rivellese et al. NMCD 2010La donna è “più complicata”
Differenze strutturali e/o funzionali dell’albero
cardiovascolare
1. Sintomi anginosi piu’ sfumati, dolore toracico atipico, sintomi
Shortness of Breaking out in
aspecifici, si reca dal medico più tardi -> Spesso cardiopatia
breath a cold sweat ischemica silente
2. Minore sensibilità ai test diagnostici
3. Coronaropatia colpisce i vasi piu’ piccoli (meno
rivascolarizzabili)
4. Le complicanze legate al trattamento sono maggiori (per es.
Light-headedness or Nausea (feeling sick sanguinamenti) e vengono trattate meno intensamente
sudden dizziness to the stomach)
Unusual or
unexplained
Trattamento TARDIVO
fatigue
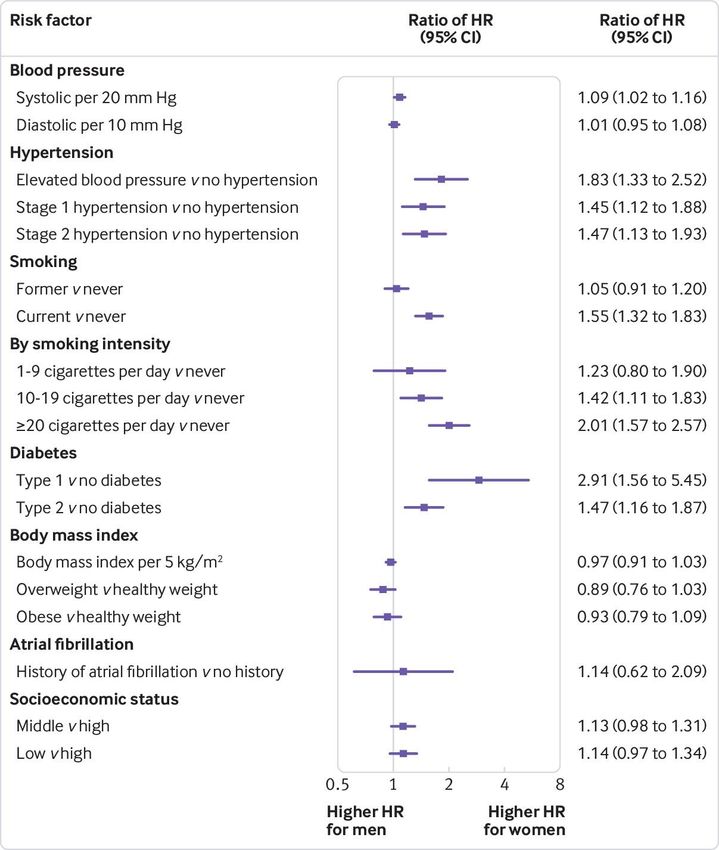
(tiredness) PROGNOSI PEGGIOREAdjusted women-to-men ratios of hazard ratios for association between risk factors and incident
myocardial infarction.
©2018 by British Medical Journal Publishing Group
Elizabeth R C Millett et al. BMJ 2018;363:bmj.k4247Smoking and Mortality among Women
with Type 2 Diabetes
Nurses’ Health Study - 20 Years of follow-up - 121.046 women
Nondiabetic women
Diabetic Women
Mortality rates (per 100.000 person-years)
2500
2000
1500
1000
500
0
Never Past 1-14 15-34 >35
cig/day cig/day cig/day
Al-Delaimy WK et al., Diabetes Care 24: 2043-2048, 2001.Effetti favorevoli degli estrogeni nella donna
FAVOREVOLE
↓ Colesterolo LDL
Lipidi
↑ Colesterolo HDL
Coagulazione ↓ Fibrinogeno
↓ Molecole di adesione
Infiammazione
↓ Attività dell’enzima
ACE
↑ Sintesi Ossido Nitrico
Funzione endoteliale e pressione ↓ Endotelina-1
arteriosa ↓ Proliferazione delle
cellule muscolari lisce
Rivellese et al. NMCD 2010Tissue-specific actions of oestrogens on energy balance and metabolic regulation in rodent models Tramunt et al (2020) Diabetologia DOI 10.1007/s00125-019-05040-3 ©The Authors 2019. Distributed under the terms of the CC BY 4.0 Attribution License (http://creativecommons.org/licenses/by/4.0/)
Le cellule endoteliali e le cellule
muscolari lisce esprimono i
recettori per gli estrogeni ERs-
alpha and ERs-beta.
Gli estrogeni hanno a breve
termine un effetto
vasodilatante e a lungo
termine una azione di
inibizione verso il danno
vascolare e di prevenzione
dell’aterosclerosiFattori di rischio cardiovascolare: differenze di genere
Diabete
• Gli estrogeni hanno un effetto protettivo in quanto promuovono la
produzione di NO! vasodilatazione endotelio dipendente maggiore nelle
donne rispetto agli uomini
• L’obesità è associata ad una riduzione della vasodilatazione endoteliale in
entrambi i sessi
• Nel diabete, mentre gli uomini non subiscono un’ulteriore compromissione
della funzione endoteliale, nelle donne vi è una notevole riduzione della
funzione endoteliale che diventa simile agli uomini
Circulation 2000; 201:2040-2046EPC e gradiente intersesso di rischio cardiovascolare
Il livello delle EPC circolanti (vasculoprotettive) è più alto nelle donne in età fertile rispetto
agli uomini di pari età.
Tale differenze viene abolita nelle donne post-menopausali rispetto agli uomini coevi.
Women Age-matched men
120 30 12 0,9
* *
.
†
100
†
25 10 * † 0,8
†
*†
.
0,7
CD34+KDR+ cells
.
.
80 20 8 0,6
%FMD
c-IMT
%KDR
6 0,5
60 15
0,4
40 10 4 0,3
20 5 0,2
2
0,1
0 0 0 0
Fertile Post- Fertile Post-
1 2
Fertile Post-
1 2
Fertile Post-
1 2
1 2
menopausal menopausal menopausal menopausal
I meccanismi di rigenerazione vascolare rispecchiano il gradiente intersesso della funzione
endoteliale (FMD), del rimodellamento vascolare (IMT) e del di rischio cardiovascolare
Fadini et al. ATVB 2008EPC e gradiente intersesso di rischio cardiovascolare.
Effetto dei fattori di rischio
F M
120
*
.
100
CD34+KDR+ cells 80
60
40
20
0
0-1 2+
La compresenza di 2+ faJori di rischio CV abolisce il gradiente intersesso di EPCs
Fadini et al. ATVB 2008Sex differences in insulin resistance across the life span Huebschmann et al (2019) Diabetologia DOI 10.1007/s00125-019-4939-5 © Elsevier. Adapted with permission from Sattar
Obesity levels are higher among women than men at the time of
type 2 diabetes diagnosis
Huebschmann et al (2019) Diabetologia DOI 10.1007/s00125-019-4939-5Fattori di rischio cardiovascolare:
differenze di genere
Ipertensione Arteriosa
Forme specifiche di ipertensione nella donna, come l’ipertensione gravidica e
l’eclampsia (10% delle gravidanze), sono associate ad un rischio di malattia
cardiovascolare futura nella donna tra 2 e 8 volte superiore, e richiedono pertanto
attente misure di valutazione, terapia e prevenzione secondariaDifferences in HDL and ApoAI by diabe'c status in women and men
The Strong Heart Study, Diabetes Care 1998Differences in LDL size and fibrinogen by diabetic status in women and men
The Strong Heart Study, Diabetes Care 1998CONTROLLO dei
FDR CARDIOVASCOLARE (donne)
NHANES III study
(Third National Health and Nutrition Examination Survey)
< 7.5%
of the Female population
met six of the seven key CVD
health metrics:
Not smoking
Eating a healthy diet
Being physically active
Normal weight
Normal blood pressure
Normale glucose level
Normal cholesterol levelsCardiovascular Disease in Type 2 Diabetes: A
Cardiovascular Disease in Type 2 Diabetes: A
Review of Sex-Related Differences in
Review of Sex-Related
Predisposition Differences in
and Prevention
Predisposition and
Abdallah Al-Salameh, Prevention
MD; Philippe Chanson, MD; Sophie Bucher, MD, PhD;
Virginie Ringa, MD, PhD; and Laurent Becquemont, MD, PhD
Abdallah Al-Salameh, MD; Philippe Chanson, MD; Sophie Bucher, MD, PhD;
Virginie Ringa, MD, PhD; and Laurent Becquemont, MD, PhD
Abstract
• Women with type 2 diabetes had higher levels of low-density lipoprotein
Type 2 diabetes mellitus is a major risk factor for cardiovascular disease. However, compiled data
cholesterol,
Abstract suggestandthatthey
type 2 are less
diabetes likely
affects to ofreceive
the risk statin
cardiovascular therapy
disease when
differentially compared
according to sex. In with
their
Type 2male counterparts.
recent
diabetes
years, large meta-analyses have confirmed that women with type 2 diabetes have a higher
mellitus is a major risk factor for cardiovascular disease. However, compiled data
relative risk of incident coronary heart disease, fatal coronary heart disease, and stroke compared with
suggest thattheir
typemale
2 diabetes affectsThe
counterparts. thereasons
risk of for
cardiovascular
these disparities disease
are notdifferentially
completely according
elucidated. to sex. In
A greater
• Women with
recent years, type
large
burden 2 diabetes
ofmeta-analyses
cardiometabolic riskhad
have to putwas
confirmed
in women onproposed
that moreaswith
women weight typeto
a partial develop
2 diabetes
explanation. havediabetes.
Indeed, higher This
a several
relative riskstudies
of incident
suggestcoronary
that womenheart disease,afatal
experience largercoronary heartindisease,
deterioration and stroke compared
major cardiovascular risk factors withand
excess weight
their male put is
counterparts. associated
on more weight Thethan with
do men
reasons a
forduringgreater
thesetheir deterioration
transitionare
disparities fromnotnormoglycemiain
completely tocardiovascular
overt type 2Adiabetes.
elucidated. risk
greater
factors’
burden oflevels,
This endothelial
excess
cardiometabolic weight risk indysfunction,
is associated with
women was proposed low-grade
higher levels of inflammation,
biomarkers
as a partial explanation. and
of endothelial dysfunction,
Indeed, several
inflammation, and procoagulant state. Moreover, sex differences in cardiovascular risk use
the prescription and of some
hypercoagulability
studies suggest that women state in women
experience a largeras compared
deterioration inwith
majormen.
cardiovascular drugs may compound an “existing” disparity. We searched PubMed for articles
factors and
put on more weight than do men during their transition from normoglycemia to overt type 2 diabetes.
published in English and French, by using the following terms: (“cardiovascular diseases”) AND
This excess(“diabetes
weight mellitus”)
is associated with disparity”
AND (“sex higher levels
OR “sex of differences”
biomarkersORof“sex endothelial dysfunction,
related differences” OR
• Women
inflammation,with andtype 2 diabetes
procoagulant state. have
Moreover, been sex underrepresented
differences in the in
prescription most
“sex-related differences” OR “sex disparities”). In this article, we review the available literature on theand clinical
use of trials
some
that focused
cardiovascular on the
drugs
sex aspects may
of impact
primary andof
compound drug
secondary interventions
an “existing”
prevention disparity. (statin
We searched
of cardiovascular therapy,
disease PubMed
in newer
people for articles
with type 2
published in English
diabetes, andpredisposition
in the French, bytousing the following
cardiovascular disease in terms: (“cardiovascular
those people, diseases”)
and in the control AND
of diabetes
antidiabetic drugs)
and associated
(“diabetes mellitus”) AND
on the occurrence
cardiovascular risk factors.
(“sex disparity”
of cardiovascular disease.
OR “sex differences” OR “sex related differences” OR
This precludes firm
conclusions about the
“sex-related differences” effects
OR “sex ª of
2018 many
disparities”). drug
Mayo Foundation
In this for treatments
Medical
article, Education
we review in women
and Research
the with
n Mayo Clin Proc.
available type 2
2019;94(2):287-308
literature on the
diabetes.
sex aspects of primary and secondary prevention of cardiovascular disease in people with type 2
D
iabetes mellitus is a major risk diabetes. Modern studies show that CVD
diabetes, in the predisposition to cardiovascular disease in those people, and in the control of diabetes
factor for cardiovascular disease is responsible for 24% to 30% of hospitaliza-
and associated cardiovascular
(CVD).
risk factors.
Its prevalence is tions2 and around one-third of deaths3,4 in From Centre de
recherche en Epidémiolo-
increasing worldwide,ª and
2018 this
Mayotrend
Foundation for Medical
is pro- Education
people withanddiabetes.
Research n Despite
Mayo Clin Proc. 2019;94(2):287-308
improve- gie et Santé desPercentuale di donne arruolate in trial randomizzati
controllati sullo scompenso cardiaco sul totale
Heiat, A. et al. Arch Intern Med2002;162:1682-688.performed separately in individuals below and over 75 groups (Figure 2). However, the most striking finding
years of age, gender disparities were still documented in of this study was that, unlike men, T2DM women were
younger people,
Gender but they
diffwere
erencesmore markedin type in elderly
2 diabetes not (Italy)
able to reach the recommended LDL-C targets, in
patients , in spite of diabetic treatment.
17
spite of a similar rate in the use of medications and the
Valeria Manicardi , Maria Chiara Rossi , Elisabetta L same
1 2
Romeo use3
, Annalisa
of statinsGiandalia
(41.2% 3of , Mariella
women Calabrese
and of men). 4
, Fur-
Elena Cimino , Daniela Antenucci , Paola Bollati , Patrizia
5 6 7
Li Volsi 8
, Ada Maff ettone 9
, Guglielmina
thermore, it was demonstrated that women with type 2 Speroni 10
,
Concetta Suraci11, Elisabetta Torlone12, Giuseppina Russo3 (on behalf of Gruppo Donna AMD)
Gender differences in lipid profile diabetes have an HDL-C subpopulations profile shifted
1. Department of Internal Medicine, Hospital of Montecchio, AUSL of Reggio Emilia, Italy; 2. CORESEARCH - Center for Outcomes
Research and Epidemiology srl, Pescara, Italy; 3. Department of Clinicaltoward small Medicine,
and Experimental dense –University
and hence less
of Messina, atheroprotective
Messina, Italy;
The lipid profile is worse in women: total cholester-
4. Diabetology Department, Prato, Italy; 5. Diabetology, Hospital of – particles, similar to the finding in diabetic men who
Niguarda, Milan, Italy; 6. Endocrinology, Lanciano (Chieti), Italy;
7. Department of Internal Medicine and Diabetology, San Carlo Hospital, Milan, Italy; 8. Diabetology Department, AAS5, Pordenone, Italy;
ol levels are higher,Unit,
9. Metabolic andHospital
moreof women (+7.2%)
Monaldi, Naples, do
Italy; 10. not ofhave
Department suffered
Internal Medicine and myocardial
Diabetology,infarction
22
.
Hospital of Codogno (ASST
Lodi), Italy; 11. Diabetology, San Paolo Hospital, Civitavecchia (Rome), Italy; 12. AO MISEM, Perugia, Italy.
Received 2 March 2016; accepted 11 March 2016.
Summary. The impact of diabetes on cardiovascular risk ci sono differenze di genere nell’utilizzo di questi farmaci.
is particularly evident in women who are most affected by Molti fattori biologici, e non solo, non ancora del tutto cono-
major cardiovascular events, especially myocardial infarc- sciuti, sottendono queste differenze e vanno esplorati.
tion, and have a higher mortality, confirming the loss of Parole chiave: genere, diabete di tipo 2, rischio cardiova-
protection by estrogens in childbearing age. Italian data scolare.
from the AMD Annals have documented that the achieve-
ment of targets for the major CV risk factors is systemati-
cally unfavorable to women with diabetes T2: women are
more obese, have a worse control of diabetes and especial- Gender differences in cardiovascular disease
ly a worse lipid profile, and a higher frequency of reduction morbidity and mortality in type 2 diabetic
in glomerular filtration rate. Other studies, such as Riace subjects
Figure 1. Favorable outcomes in diabetic men and women and age (AMD Annals). The intermediate outcomes (target of HbA1c, PA,
andsystematically
C-LDL, BMI) are Mind It, confirminthis.
favorIn of
themen,
world, women with diabe-
independently of age.
tes are systematically under-treated with drugs for CV risk The widely recognized association between type 2
factors, such as ASA, ACE-I, β-blockers, statins, and hypo- diabetes and cardiovascular disease (CVD) has a dif-
glycemic agents, and this may explain the failure to achieve ferent significance according to sex, being stronger in
Table 1. Clinical characteristics
the targets. and
On the contrary, treatment, bydata
the- IlItalian
- Copyright Pensierosex and
are age.
Scientifico Modifi
bucking
Editore ed from
diabetic
downloaded Rossi
women MC compared
et Mon,
by IP 147.162.241.198 al, 2013 .
17 .2020, 13:31:37
with
11 May men. Diabetic women
the trend by showing that there are gender differences in seem to lose their female advantage toward CVD, be-
the use of these medications.
60 Review
Further studies are needed to ing more exposed to this Ital complication irrespective
J Gender-Specific Med of
2016; 2(2): 60-68
investigate biological and non-biological Overallfactors, underly- AgeTabella 4 bis
Costi assistenziali (basati sulle tariffe: DRG, nomenclatore,
ecc.) Confronto femmine e maschi
N N
Osservatorio Arno Diabete 2018Singole prestazioni specialistiche
Tabella 15bis più utilizzate nei soggetti
con e senza diabete
Confronto femmine-maschi
Emocromocitometrico
Creatinina
90.09.2
Osservatorio Arno Diabete 2018Gender differences in type 2 diabetes (Italy)
Valeria Manicardi1, Maria Chiara Rossi2, Elisabetta L Romeo3, Annalisa Giandalia3, Mariella Calabrese4,
Elena Cimino5, Daniela Antenucci6, Paola Bollati7, Patrizia Li Volsi8, Ada Maffettone9, Guglielmina Speroni10,
Concetta Suraci11, Elisabetta Torlone12, Giuseppina Russo3 (on behalf of Gruppo Donna AMD)
1. Department of Internal Medicine, Hospital of Montecchio, AUSL of Reggio Emilia, Italy; 2. CORESEARCH - Center for Outcomes
Research and Epidemiology srl, Pescara, Italy; 3. Department of Clinical and Experimental Medicine, University of Messina, Messina, Italy;
4. Diabetology Department, Prato, Italy; 5. Diabetology, Hospital of Niguarda, Milan, Italy; 6. Endocrinology, Lanciano (Chieti), Italy;
7. Department of Internal Medicine and Diabetology, San Carlo Hospital, Milan, Italy; 8. Diabetology Department, AAS5, Pordenone, Italy;
9. Metabolic Unit, Hospital of Monaldi, Naples, Italy; 10. Department of Internal Medicine and Diabetology, Hospital of Codogno (ASST
Lodi), Italy; 11. Diabetology, San Paolo Hospital, Civitavecchia (Rome), Italy; 12. AO MISEM, Perugia, Italy.
Received 2 March 2016; accepted 11 March 2016.
Gender-differences have been reported in diabetic patients: in Italy they are less pronounced
than in other countries, but it exists despite equal access to specialist care.
Summary. The impact of diabetes on cardiovascular risk ci sono differenze di genere nell’utilizzo di questi farmaci.
■ The likelihood to reach metabolic targets (HbA1c,Molti
is particularly evident in women who are most affected by LDL-C,
fattoriBMI, PA)eisnon
biologici, systematically
solo, non ancora del unfavorable
tutto cono-
major cardiovascular events, especially myocardial infarc- sciuti, sottendono queste differenze e vanno esplorati.
in diabetic women as compared with men.
tion, and have a higher mortality, confirming the loss of Parole chiave: genere, diabete di tipo 2, rischio cardiova-
protection by estrogens in childbearing
■ Diabetic women have a worse lipid profile than men, age. Italian data scolare.and have a 2-fold higher CHD risk
from the AMD Annals have documented that the achieve-
compared with for
ment of targets men. Myocardial
the major infarction
CV risk factors occurs earlier and has higher mortality in women with
is systemati-
DMcally
compared
unfavorable with men.with diabetes T2: women are
to women
more obese, have a worse control of diabetes and especial- Gender differences in cardiovascular disease
■ Diabetic women
ly a worse lipid profile,are
andsystematically
a higher frequencyundertreated
of reduction with CV therapy,
morbidity such asinASA,
and mortality type 2ACE – I, β-
diabetic
blockers, hypoglycemic agents, but not in Italy.
in glomerular filtration rate. Other studies, such as Riace subjects
and Mind It, confirm this. In the world, women with diabe-
■ Pathophysiological factors are
tes are systematically under-treated involved
with drugs for in CVthe
risk greater Thedifficulty to reachassociation
widely recognized LDL-C targets between in type 2
factors, such as ASA, ACE-I, β-blockers, statins, and hypo- diabetes and cardiovascular disease (CVD) has a dif-
diabetic women, despite the same drug
glycemic agents, and this may explain the failure to achieve
treatment in Italy.
ferent significance according to sex, being stronger in
the targets. On the contrary, the- IlItalian
- Copyright Pensierodata are bucking
Scientifico diabetic
Editore downloaded women compared
by IP 147.162.241.198 with
Mon, 11 May 2020, men.
13:31:37Diabetic women
the trend by showing that there are gender differences in seem to lose their female advantage toward CVD, be-
the use of these medications.
60 Review
Further studies are needed to ing more exposed to this Ital complication irrespective
J Gender-Specific Med of
2016; 2(2): 60-68
investigate biological and non-biological factors, underly- menopausal status . 1,2
ing these differences. Accordingly, in newly diagnosed diabetic subjectsCardiovascular Disease
Cardiovascular DiseaseininType
Type22 Diabetes:
Diabetes: AA
Review of Sex-Related
Review of Sex-RelatedDifferences
Differences in
Predisposition andand
Predisposition Prevention
Prevention
AbdallahAbdallah Al-Salameh,
Al-Salameh, MD; Philippe
MD; Philippe Chanson,
Chanson, MD;MD;Sophie
SophieBucher,
Bucher, MD,
MD, PhD;
PhD;
Virginie Ringa, MD, PhD; and Laurent Becquemont, MD, PhD
Virginie Ringa, MD, PhD; and Laurent Becquemont, MD, PhD
Abstract
Abstract
Type 2 diabetes mellitus is a major risk factor for cardiovascular disease. However, compiled data
Type 2 diabetes
suggest thatmellitus is a major
type 2 diabetes risk
affects thefactor
risk of for cardiovascular
cardiovascular diseasedisease. However,
differentially compiled
according to sex. Indata
recent
suggest that typeyears, large meta-analyses
2 diabetes affects the riskhaveofconfirmed
cardiovascularthat women
diseasewith type 2 diabetes
differentially have a to
according higher
sex. In
• More research is needed to understand biological mechanisms
relative risk of incident coronary heart disease, fatal coronary heart disease,
recent years, large meta-analyses have confirmed that women with type 2 diabetes have a higher and stroke compared with
theirofmale counterparts.
coronaryThe reasons for these disparities heart
are notdisease,
completely
and elucidated. A greater
underlying the sex differences in the risk of cardiovascular dis-
relative risk incident heart disease, fatal coronary
burden of cardiometabolic risk in women was proposed as a partial explanation. Indeed, several
their male counterparts. The reasons for these disparities are not completely elucidated. A greater
stroke compared with
studies suggest that women experience a larger deterioration in major cardiovascular risk factors and
ease in people with type 2 diabetes.
burden ofputcardiometabolic
studies suggest
on more weight than
that women
riskdoinmen
experience
women
during was proposedfrom
their transition as anormoglycemia
partial explanation. Indeed,
to overt type several
2 diabetes.
This excess weight is associated awith
largerhigher
deterioration
levels of in major cardiovascular
biomarkers of endothelialrisk factors and
dysfunction,
put on more weight than
inflammation, and do men during
procoagulant their
state. transition
Moreover, sex from normoglycemia
differences to overt
in the prescription andtype
use 2ofdiabetes.
some
This excess weight isdrugs
cardiovascular associated with higher
may compound levels of
an “existing” biomarkers
disparity. of endothelial
We searched PubMed for dysfunction,
articles
• More effort is needed to reduce the gap between the sexes in
published
inflammation, and inprocoagulant
English and state.
French,Moreover,
by using the sex following
differencesterms: (“cardiovascular
in the prescriptiondiseases”)
and use of AND some
terms of the use of evidence-based treatment and
(“diabetes
published“sex-related
in English
mellitus”) AND
differences”
(“sex
OR “sex
and French,
disparity”
by disparities”).
OR “sex differences”
cardiovascular drugs may compound an “existing” disparity. We searched PubMed for articles
In this article,
using the following
OR
we review
terms:
“sex related differences”
the available literature
(“cardiovascular diseases”)
OR
on the
AND
participation in clinical trials.
sex aspects of primary and secondary prevention of cardiovascular disease in people with type 2
(“diabetes mellitus”) AND (“sex disparity” OR “sex differences” OR “sex related differences” OR
diabetes, in the predisposition to cardiovascular disease in those people, and in the control of diabetes
“sex-related differences” OR “sex disparities”). In this article, we review the available literature on the
and associated cardiovascular risk factors.
sex aspects of primary and secondary prevention of cardiovascular disease in people with type 2
ª 2018 Mayo Foundation for Medical Education and Research n Mayo Clin Proc. 2019;94(2):287-308
diabetes, in the predisposition to cardiovascular disease in those people, and in the control of diabetes
D
and associated cardiovascular riskis factors.
iabetes mellitus a major risk diabetes. Modern studies show that CVD
factor for cardiovascular
ª 2018 Mayo Foundation is responsible
disease for Medical Education for
and 24% to 30%
Research of hospitaliza-
n Mayo Clin Proc. 2019;94(2):287-308
(CVD). Its prevalence is tions2 and around one-third of deaths3,4 in From Centre de
recherche en Epidémiolo-I Fattori di rischio
• Non modificabili
• Età
• Sesso
• Razza
• Familiarità
• Modificabili
– Maggiori
• Fumo
• Ipertensione arteriosa
• Iperdislipidemia
• Diabete / iperinsulinemia / resistenza insulinica
• Obesità / sindrome metabolica
• Sedentarietà fisica
– Meno documentati
• Dieta / abuso di bevande alcoliche
• Iperomocisteinemia
• Ipercoagulabilità / Infiammazione
• Contraccettivi orali / terapie ormonali
Goldstein et al., Circulation 2001; 103:163• Prospective cohort of 2357 healthy men (mean age, 72 years)
enrolled in the Physicians’ Health Study
• 970 men (41%) survived >90 years
• The probability of surviving >90 years was 54% in the absence
of:
– Smoking
– Diabetes
– Obesity
– Hypertension
– Sedentary life styleCaratteristiche peculiari della macroangiopatia diabetica nella donna Fisiopatologiche " maggior interessamento del microcircolo " erosione di placca, vasospasmo, dissezione coronarica e cardiomiopatia stress- correlata piuttosto che rottura di placca Cliniche " ritardato accesso al pronto soccorso, " sintomi di presentazione atipici, incerti valori di riferimento della troponina " maggior incidenza di complicazioni periprocedurali durante angioplastica " peggior outcome dopo by-pass aorto-coronarico " eccesso di mortalità durante fibrinolisi Epidemiologiche " età di insorgenza della coronaropatia e dell’arteriopatia obliterante più tardiva " minor trend alla riduzione della mortalità da malattie CVD negli ultimi 10 anni Razziali " elevata prevalenza di infarto tra le donne afro-americane Sociali " minor accesso delle donne delle minoranze a programmi riabilitativi " minor riduzione del fumo
ve data and prospective controlled progestin-only contraception for women with a history of
Summary of important sex and gender differences
fy the best method. Metabolic and
ording to combinations, specific
gestational diabetes or diabetes, while other forms of contra-
ception, especially intrauterine and subcutaneous types
and challenges in T2DM management.
s, underlining complexity of the should be preferred choices in insufficiently controlled
Vomen vs men
portant sex and gender differences and challenges in T2DM management.
! High risk of missing early diagnosis based on fasting glucose measurements only
! Greater impact of reproductive factors and silent inflammation
! Higher rates of obesity contributing to complications and influencing therapeutic choice
! Greater risk of stigmatisation of obese young women channelling treatment options
! Better attendance at structured diabetes education
! Lower success of glucose-lowering therapy and greater risk of failure of dual therapy
! Potentially higher degree of worriedness and uncertainty related to insulin therapy
! Higher risk of hypoglycemia on insulin treatment
! Dyslipidemia more closely related to CVD
! Worse control of cardiovascular risk factors and monitoring of complications
! Lower adherence of evidence based cardiovascular therapy
! Greater relative risk of CHD, stroke as well as CV and total mortality
! More side effects and lower drug adherence in women regarding use of statins
! Higher rates of depression further aggravating therapeutic success
! Depression and psychosocial stress show greater impact on CVD
! More comorbidities and thus higher risk of polypharmacy
! Missing data of sex differences of potential drug efficacy on complications
! Missing information on sex-specific effects and adverse events for most available drugs
! Studies in pregnancy missing, some common drugs (e.g. RAS blockers, statins) teratogenic
diabetes research and clinical prac/ce 131 (2017) 230–241•Informarsi ma soprattutto educarsi alla salute •Seguire strategie per uno stile di vita adeguato e corretto •Partecipare alla gestione della propria salute insieme agli operatori sanitari competenti della salute
Puoi anche leggere