L'ASPETTO NUTRIZIONALE DELL' IPF - Evidenze nella real life: esperienze con nintedanib a confronto
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
Evidenze nella real life: esperienze con nintedanib a confronto
L’ASPETTO NUTRIZIONALE DELL’ IPF
Stefano Marinari
UOSD PNEUMOLOGIA
CHIETI
CASO CLINICO: anamnesi Nome: T. M. Cognome: D’A. Data di nascita: 25/02/1939 Data riscontro patologia: 2017 Ex fumatore: 20 sig/die fino a 4 anni fa Professione: non esposto Anamnesi Farmacologica: neg Riferito dimagramento (circa 7 kg in un anno) Familiarità: negativa Screening autoanticorpale: Neg. BMI: 24,6 Comorbilità: Maculopatia; Nessuna altra comorbilità Altri farmaci: Macular (vit. D collirio), Ismigen
CASO CLINICO: Studio funzionale
Test cammino: SatO2: 91% → 89 % 73 items 13 domain- QoL 15 items- Impatto
Dispnea : 2 – 4 Borg ;Distanza percorsa 6’ : 320 mt
MRC: 2
GAP: 5 (16,2% mort ad 1 anno) Health Qual Life Outcomes 2010, Jul 31;
Chron Respir Dis 2017 May; 14 (2) ; 140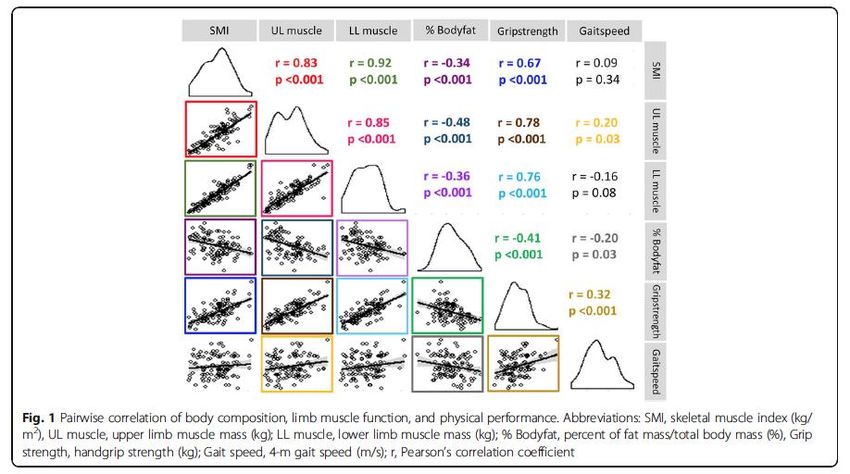
CASO CLINICO: quadro radiologico
Pattern HRCT: UIP
Conferma IPF in MD
(novembre 2018)
Nutrition. 2019 Jun;62:115-121. doi: 10.1016/j.nut.2018.12.008. Epub 2018 Dec 19. What are the best indicators to assess malnutrition in idiopathic pulmonary fibrosis patients? A cross-sectional study in a referral center. Jouneau S, Kerjouan M, Rousseau C, Lederlin M, Llamas-Guttierez F, De Latour B, Guillot S, Vernhet L, Desrues B, Thibault R. Abstract OBJECTIVES: Little is known about the indicators to assess malnutrition in patients with idiopathic pulmonary fibrosis (IPF). This study aimed to determine the following: 1) the prevalence of malnutrition in IPF patients; 2) the nutritional indicators predictive of low fat-free mass (FFM) as measured by bioimpedance analysis; 3) the IPF patients' characteristics associated with low FFM. METHODS: The IPF patients were consecutively recruited in a referral center for rare pulmonary diseases. Malnutrition was defined as a fat-free mass index (FFMI) = FFM (kg) / (height [m]2)
CASO CLINICO: valutazione nutrizionale
Questionario valutazione abitudini
alimentari e stile di vita (ISS): normale
attività ; dieta equilibrata
Altezza 170 cm Vita 92cm Rz 474
Peso 71 kg Addome 95 cm Xc 40
BMI 24.6 Fianchi 96 cm FFMI 19,9 kg/h2
RapportoV/F 0,95
Rapporto V/H 54
muscle atrophy/sarcopenia: BMI < 21 and FFMI ≤16 (men) or ≤15 (women)
CASO CLINICO: inizio terapia Data inizio trattamento: Novembre 2018 ⃝ Pirfenidone ⃝ Nintedanib 150 MG Consigli Nutrizionali Terapia di supporto: O2 terapia durante esercizio Consiglio Riabilitazione respiratoria
CASO CLINICO: Controllo a 6 mesi
Data di nascita: 25/02/1939
⃝ Pirfenidone ⃝ Nintedanib 150 mg
Data inizio trattamento: Gennaio 2018
Aderenza terapia: assunzione regolare
Test cammino (con O2 1l): SatO2: 92% → 87%
Dispnea : 3 – 5 Borg Distanza percorsa 3’ : 120 mt
(test interrotto per dispnea intensa)
MRC: 3
GAP: 6 (39,2% mort. ad 1 anno)
PFR: FVC: 69% vs 77%
DLCO 20% vs 31%
CASO CLINICO: Controllo a 6 mesi
Perdita di peso: 7kg (10% ca)
Quest. Att. Fis. e Ab. Al.: poco attivo ; non
riferite significative variazione della dieta
Effetti indesiderati:
⃝ nausea ⃝ cefalea
⃝ eruzione cutanea ⃝ dimi. appetito
⃝ diarrea ⃝ MRGE
⃝ dispepsia ⃝ vomito
Diuresi: Nella norma
Altezza 170 cm Vita 92 Rz 486
Peso 64kg Addome 94 Xc 32
BMI 22 kg/h2 Fianchi 89 FFMI 17,6 Kg/h2
BMI Prec 24,6 kg/h2 FFMIprec 19,9 kg/h2
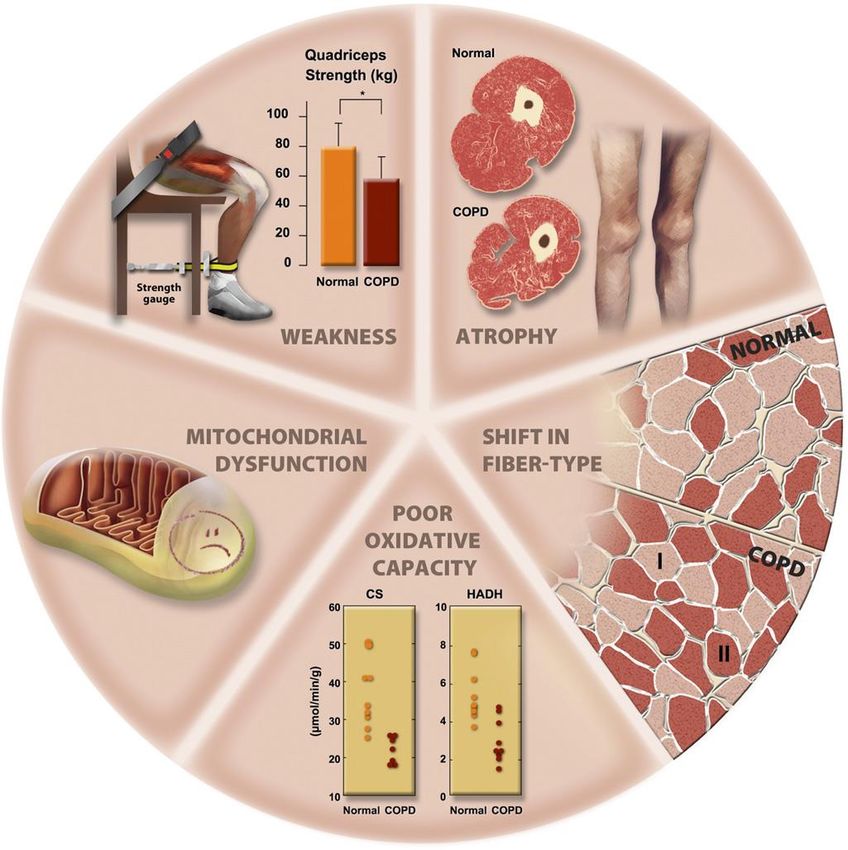
Malnutrizione e IPF (?)/ Disfunzione muscolare
Patogenesi AMERI CAN T HORACI C SOCI ET Y
DOCUMENT S
An Official American Thoracic Society/European Respiratory Society
Statement: Update on Limb Muscle Dysfunction in Chronic Obstructive
Pulmonary Disease
François Maltais, Marc Decramer, Richard Casaburi, Esther Barreiro, Yan Burelle, Richard Debigaré,
P. N. Richard Dekhuijzen, Frits Franssen, Ghislaine Gayan-Ramirez, Joaquim Gea, Harry R. Gosker, Rik Gosselink,
BPCO Fumo
Maurice Hayot, Sabah N. A. Hussain, Wim Janssens, Micheal I. Polkey, Josep Roca, Didier Saey, Annemie
M. W. J. Schols, Martijn A. Spruit, Michael Steiner, Tanja Taivassalo, Thierry Troosters, Ioannis Vogiatzis, and
Peter D. Wagner; on behalf of the ATS/ERS Ad Hoc Committee on Limb Muscle Dysfunction in COPD
THIS OFFICIAL STATEMENT OF THE AMERICAN THORACIC SOCIETY (ATS) AND THE EUROPEAN RESPIRATORY SOCIETY (ERS) WAS APPROVED BY THE ATS BOARD OF
DIRECTORS, NOVEMBER 2013, AND BY THE ERS EXECUTIVE COMMITTEE, SEPTEMBER 2013
Ipercapnia Dispnea Capacità ossidativa Ipossia Consumo O2 Infiammazione Background: Limb muscle dysfunction is prevalent in chronic Results: We identified important advances in our understanding
obstructive pulmonary disease(COPD) and it hasimportant clinical of theextent and nature of thestructural alterations in limb muscles
muscolare
implications, such as reduced exercise tolerance, quality of life, in patients with COPD. Since the last update, landmark studies
and even survival. Since the previous American Thoracic Society/ were published on the mechanisms of development of limb muscle
European Respiratory Society (ATS/ERS) statement on limb dysfunction in COPD and on thetreatment of this condition. We
muscle dysfunction, important progress has been made on the now have a better understanding of theclinical implications of limb
TNF
characterization of this problem and on our understanding of its muscle dysfunction. Although exercise training is themost potent
pathophysiology and clinical implications. intervention to address this condition, other therapies, such as
neuromuscular electrical stimulation, are emerging. Assessment of
Purpose: The purpose of this document is to update the 1999 limb muscle function can identify patients who are at increased risk
ATS/ERSstatement on limb muscle dysfunction in COPD. of poor clinical outcomes, such asexerciseintoleranceand premature
Catecolamine Farmaci OCB→ Effetto termogenico Leptina Methods: An interdisciplinary committee of experts from theATS
and ERSPulmonary Rehabilitation and Clinical Problems assemblies
mortality.
determined that thescopeof thisdocument should belimited to Conclusions: Limb muscle dysfunction is a key systemic
dell’attività limb muscles. Committee members conducted focused reviews of the
literatureon several topics. A librarian alsoperformed aliteraturesearch.
consequenceof COPD. However, therearestill important gapsin our
knowledge about themechanisms of development of this problem.
An ATSmethodologist provided adviceto thecommittee, ensuring that Strategies for early detection and specific treatments for this
themethodological approach wasconsistent with ATSstandards. condition are also needed.
Overview dysfunction have been identified (e.g., Thepurposeof thisdocument isto update
deconditioning), much needs to be learned the 1999 American Thoracic Society/European
Limb muscle dysfunction is an important about the impact of other potential Respiratory Society (ATS/ERS) statement
systemic consequence of chronic obstructive contributors to this clinical manifestation in on limb muscle dysfunction. We intend to
Spesa energetica Apporto energetico/consumo
pulmonary disease (COPD) because of its COPD. Limb muscle dysfunction can be provide researchers and clinicians with the
impact on physical activity, exercise prevented and improved, in part, with recent advances in this field, with emphasis
tolerance, quality of life, and even survival in exercise training, but it is clear that novel on the following areas: (1) structural and
this disease. Although some mechanisms therapies are needed to better address this metabolic alterations found in limb muscles,
underlying the development of limb muscle problem. (2) consequences and clinical evaluation of
DEPLEZIONE NUTRIZIONALE
F.M. holds a CIHR/GSK Research Chair on COPD at Universit é Laval. R.C. holds the Grancell/Burns Chair in the Rehabilitative Sciences. E.B.’s contribution to
this statement was supported by CIBERES, FIS 11/02029, 2009-SGR-393, SEPAR 2010, FUCAP 2011, FUCAP 2012, and Marat ó TV3 (MTV3-07-1010)
(Spain) and by the ERS COPD Research Award 2008. M.I.P.’s contribution to this statement was supported by the NIHR Respiratory Disease Biomedical
Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College London, who partially fund his salary.
Am J Respir Crit Care Med Vol 189, Iss 9, pp e15–e62, May 1, 2014
Copyright © 2014 by the American Thoracic Society
DOI: 10.1164/rccm.201402-0373ST
Internet address: www.atsjournals.org
American Thoracic Society Documents e15
European Respiratory Monograph , vol 8 Monografia 24, March 2003; pag. 11-22CASO CLINICO: terapia Data inizio trattamento: Novembre 2018 ⃝ Pirfenidone ⃝ Nintedanib 150 MG Consigli Nutrizionali Terapia di supporto: O2 terapia durante esercizio Consiglio Riabilitazione respiratoria Iniziato supporto nutraceutico Ravvicinato controllo per monitoraggio (3 mesi) Controllo TC torace HR
Take Home Messages • La valutazione nutrizionale è un aspetto necessario per una completa valutazione prognostica (nuovi indici prognostici); • L’utilizzo di metodi di valutazione della composizione corporea (BIA) permettono di evidenziare la presenza di malnutrizione anche in presenza di normo o sovrappeso; • La presenza di malnutrizione deve essere considerata nella valutazione della terapia sia farmacologica (effetti collaterali) che di supporto (riabilitazione, supporto nutraceutico)
FIBROSI POLMONARE IDIOPATICA
PERDITA DI PESO e PROGNOSI
• 210 pazienti con IPF
• 40 (19%) con perdita di peso
(>5%);
• 6,1% di perdita di peso predice
mortalità indipendentemente
dal declino FVCFIBROSI POLMONARE IDIOPATICA
DISFUNZIONE MUSCOLARE E
SOPRAVVIVENZA
• 131 PAZIENTI CON IPF E 43 CON FIBROELASTOSI PLEUROPARENCHIMALE
• AREA SEZIONE E DENSITA’ MUSCOLO ERECTOR SPINAE (TC TORACE)ETA’ BMI PERDITA DI PESO RAPPORTO
(aa) (kg/m^2) (kg) WAIST/HIPS
TOTALE 70 ± 8.8 26.94 ± 2.3 4.4 ± 4.1 0.97 ± 0.1
PZ
(n=34)
Pirfen. 71.60 ± 8.5 25.94 ± 3.0 3.80 ± 4.1 0.98 ± 0.0
(n=20)
Ninted 73.14 ± 10.7 25.12 ± 2.8 8.00 ± 5.4 0.91 ± 0.1
(n=14)
P< NS NS 0.01 0.02
FVC% DLCO% 6MWT (m) Δ SAT% DISPNEA PRE DISPNEA
(Borg) POST (Borg)
TOTALE 87.17 ± 51.59 ± 340.67 ± 4.27 ± 0.77 ± 0.7 2.10 ± 1.9
PZ 25.7 16.8 83.2 2.7
(n=34)
Pirfen. 90.29 ± 55.41 ± 360.24 ± 3.65 ± 0.79 ± 0.6 1.56 ± 1.3
(n=20) 28.2 20.0 66.5 3.6
Ninted 82.71 ± 46.02 ± 321.92 ± 4.38 ± 0.62 ± 0.7 2,15 ± 1.9
(n=14) 20.7 19.4 90.5 3.1
P< NS NS NS NS NS NS34 pazienti che eseguivano esame BIA dopo il riscontro di perdita
di peso (> 5%): tendenza alla MN : 13 pz. (38%ca) MN: 3 (9%ca)
BIA T0 BIA T1 T0
T1
(6mesi)La perdita di massa magra (in termini di ridotto FFMI e Angolo di fase), e non il BMI, correla
con la riduzione della capacità di diffusione (a T0: riscontro di calo ponderale);
Pirfenidone Nintedanib
I pazienti MN hanno una
significativa minore capacità di
esercizio (pRelationship between body mass index (BMI)
and decline in FVC in patients with IPF
• Poster to be presented by Stéphane Jouneau at the European Respiratory Society
Congress, Madrid, Spain, 28 September–2 October 2019Introduction and Aim
– There is some evidence that lower BMI is associated with a worse
prognosis in patients with IPF, although this has not been
observed in all studies1–4
– We assessed whether BMI at baseline was associated with disease
progression or influenced the treatment effect of nintedanib in
the INPULSIS trials
1. Alakhras M et al. Chest 2007;131:1448–53; 2. Snyder L et al. Respir Res 2019;20:105; 3. Kishaba T et al. J Thorac Dis 2016;8:3596–604; 4. Nishiyama O et al.
Respirology 2017;22:480–5; 5. Richeldi L et al. N Engl J Med 2014;370:2071–82.Methods (1/2)
• Analyses were conducted post-hoc using pooled data from patients in the INPULSIS
trials who received ≥1 dose of study drug
• The following outcomes were assessed over 52 weeks in subgroups by BMI below
and at least the median at baseline:
– Annual rate of decline in FVC (mL/year)
– Absolute changes from baseline in FVC
– Absolute change from baseline in SGRQ total score
– Time to absolute decline in FVC ≥10% predicted or death
– Time to first investigator-reported acute exacerbation
– Time to death
SGRQ, St George’s Respiratory Questionnaire.
• Poster to be presented by Stéphane Jouneau at the European Respiratory Society Congress, Madrid, Spain, 28 September–2
October 2019Methods (2/2)
• Annual rate of decline in FVC was analysed using a random coefficient
regression model
• Absolute changes were analysed using a mixed model for repeated
measures analysis and time to event analyses were based on Cox
regression analysis
• Interaction p-values were calculated to assess potential heterogeneity in
the effect of nintedanib versus placebo between the subgroups, with no
adjustment for multiple testing
• Poster to be presented by Stéphane Jouneau at the European Respiratory Society Congress, Madrid, Spain, 28 September–2
October 2019Change from baseline in FVC (mL) over 52 weeks by baseline
BMI below and at least the median
Nintedanib; BMI >= 27 kg/m2 Placebo; BMI >= 27 kg/m2
40
Nintedanib; BMIAdverse events in subgroups of patients by baseline BMI
below and at least the median (1/2)
Baseline BMIConclusions
• In the INPULSIS trials, the rate of decline in FVC over 52 weeks was
greater in placebo-treated patients with BMI below than above the
median at baseline (Indipendente dal trattamento)
• The decline in FVC in patients treated with nintedanib was similar in
patients with baseline BMI below and above the median
• Patients with IPF should receive appropriate supportive care, including
nutritional interventions when required, and a proactive approach
should be taken to the management of gastrointestinal adverse events
associated with antifibrotic therapies
• Poster to be presented by Stéphane Jouneau at the European Respiratory Society Congress, Madrid, Spain, 28 September–2
October 2019Association between weight loss and
decline in FVC in patients with IPF
• Poster to be presented by Bruno Crestani at the European Respiratory Society
Congress, Madrid, Spain, 28 September–2 October 2019Introduction and Aim
– Weight loss has been associated with an increase in FVC in obese
individuals1, in the general population2, and in patients with IPF3,
but it remains unclear whether small weight reductions have an
impact on FVC in patients with IPF
– We investigated whether weight loss over 52 weeks was associated
with disease progression or a difference in the treatment effect of
nintedanib in the INPULSIS trials
1. Womack CJ et al. J Gerontol A Biol Sci Med Sci 2000;55:M453–57; 2. Fenger RV et al. BMC Pulm Med 2014;14:208; 3. Nakatsuka Y et al. Respiration
2018;96:338–47Methods (1/2)
• Analyses were conducted post-hoc using pooled data from patients in the INPULSIS
trials who received ≥1 dose of study drug and had a weight measurement at week 52
• Rate of decline in FVC (mL/yr) over 52 weeks was assessed in subgroups based on
change in weight over 52 weeks:
– Weight gain or ≤5% weight loss; >5% weight loss
– Weight gain/no weight loss; >0 to ≤5% weight loss; >5 to ≤10% weight loss; >10%
weight loss
• The following outcomes were also assessed in subgroups by weight gain or ≤5% weight
loss versus >5% weight loss over 52 weeks:
– Absolute change from baseline in FVC; time to first investigator-reported acute
exacerbation; absolute change from baseline in SGRQ total score; time to absolute
decline in FVC ≥10% predicted or death; time to death
SGRQ, St George’s Respiratory Questionnaire.
• Poster to be presented by Bruno Crestani at the European Respiratory Society Congress, Madrid, Spain, 28 September–2
October 2019Methods (2/2)
• Annual rate of decline in FVC was analysed using a random coefficient
regression model
• Absolute changes were analysed using a mixed model for repeated
measures analysis and time to event analyses were based on a Cox
regression analysis
• Interaction p-values were calculated to assess potential heterogeneity
in the effect of nintedanib versus placebo between the subgroups, with
no adjustment for multiple testing
• Adverse events are presented descriptively
• Poster to be presented by Bruno Crestani at the European Respiratory Society Congress, Madrid, Spain, 28 September–2
October 2019Change from baseline in FVC (mL) in subgroups by weight loss
≤5% and >5% over 52 weeks
Nintedanib; >5% weight loss Placebo; >5% weight loss
40 Nintedanib; ≤5% weight loss Placebo; ≤5% weight loss
Mean (SE) absolute change from
0
-40
baseline in FVC (mL)
-80
-120
-160
-200
-240
-280
-320
-360
-400
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54
Number of patients Week
>5% weight loss
Nintedanib 226 226 224 221 220 219 213 195
Placebo 83 82 81 81 82 82 79 70
≤5% weight loss
Nintedanib 409 400 392 392 384 368 356 324
Placebo 338 335 327 326 321 313 304 275
• Poster to be presented by Bruno Crestani at the European Respiratory Society Congress, Madrid, Spain, 28 September–2
October 2019La perdita di peso è associata a maggiori effetti collaterali GI (NS)
Adverse events in subgroups by weight loss ≤5% and >5% over 52 weeks
Weight loss ≤5% Weight loss >5%
Nintedanib Placebo Nintedanib Placebo
(n=409) (n=338) (n=226) (n=83)
Adverse events 388 (94.9) 299 (88.5) 219 (96.9) 79 (95.2)
Most frequent adverse events*
Diarrhoea 220 (53.8) 56 (16.6) 172 (76.1) 22 (26.5) ??!!
Progression of IPF† 34 (8.3) 41 (12.1) 29 (12.8) 20 (24.1)
Dyspnoea 21 (5.1) 38 (11.2) 28 (12.4) 10 (12.0)
Nausea 90 (22.0) 19 (5.6) 66 (29.2) 9 (10.8)
Pneumonia 24 (5.9) 17 (5.0) 9 (4.0) 9 (10.8)
Nasopharyngitis 47 (11.5) 57 (16.9) 40 (17.7) 11 (13.3)
Decreased appetite 27 (6.6) 12 (3.6) 41 (18.1) 12 (14.5)
Cough 56 (13.7) 46 (13.6) 29 (12.8) 11 (13.3)
Bronchitis 45 (11.0) 33 (9.8) 22 (9.7) 12 (14.5)
Vomiting 42 (10.3) 9 (2.7) 32 (14.2) 2 (2.4)
Upper respiratory tract infection 39 (9.5) 35 (10.4) 19 (8.4) 7 (8.4)
Abdominal pain 33 (8.1) 8 (2.4) 23 (10.2) 2 (2.4)
Weight decreased 18 (4.4) 3 (0.9) 44 (19.5) 12 (14.5)
Data are n (%) of patients with ≥1 such adverse event reported over 52 weeks plus a 4-week post-treatment follow-up period. *Adverse events by MedDRA preferred
term reported in ≥10% of patients in ≥1 of the subgroups shown. †Corresponds to MedDRA term ‘IPF’, which included disease worsening and acute exacerbations.
• Poster to be presented by Bruno Crestani at the European Respiratory Society Congress, Madrid, Spain, 28 September–2
October 2019Conclusions
– In the INPULSIS trials, the rate of decline in FVC was greater in placebo-treated
patients who had >5% than ≤5% weight loss over 52 weeks
– The rate of decline in FVC in patients treated with nintedanib was similar in
patients with >5% and ≤5% weight loss
– The adverse event profile of nintedanib was similar in patients who had >5% and
≤5% weight loss
– Patients with IPF should receive appropriate supportive care, including
nutritional interventions when required, and a proactive approach should be
taken to the management of gastrointestinal adverse events associated with
antifibrotic therapies
• Poster to be presented by Bruno Crestani at the European Respiratory Society Congress, Madrid, Spain, 28 September–2
October 2019Efficacy and safety of nintedanib in the
elderly patient with IPF
• Poster to be presented by Elisabeth Bendstrup at the European Respiratory
Society Congress, Madrid, Spain, 28 September–2 October 2019Introduction
– IPF is a progressive fibrosing interstitial lung disease that
predominantly affects individuals over the age of 60 years1
– Elderly patients with IPF are more likely to be frail, have
comorbidities, and experience side-effects from medications;2
thus older age may be a barrier to initiating antifibrotic therapy
1. Raghu G et al. Am J Respir Crit Care Med 2018;198:e44–e68; 2. Jo HE et al. Drugs Aging 2016;33:321–34.Baseline characteristics by age
Adverse events by age
Adverse events leading to treatment discontinuation by
ageConclusions
– In an analysis of pooled data from 1690 patients with IPF from five
placebo-controlled trials, nintedanib had the same benefit on reducing
FVC decline in patients aged ≥75 years as in patients agedMalnutrizione e Fibrosi Polmonare Idiopatica
L’esempio della BPCOApplicazione del grafico Bivariato (Z-score) in un gruppo
di pazienti con BPCO moderato-grave
Z(Xc)
4
n. 81 pazienti BPCO con
3 ostruzione moderata/grave
2
Età: 71.2 ± 7.7 anni
1
95% tolerance BMI: 26.1 ± 5.1
75% tolerance
50% tolerance
0
□
Group 6
FEV1: 41.2 ± 14.4 % pred.
-4 -3 -2 -1 0 1 2 3 4
Z(R)
-1 PaO2: 68.6 ± 12.1 mmHg
-2 6’WT: 340.1 ± 159.1 mtr
-3
-4Medie vettori BIA in pazienti BPCO
(R/Xc graph)
60 60
50 50
40 40
Xc/H, Ohm/m
Xc/H, Ohm/m
30 30
20 20
10 10
0 0
0 100 200 300 400 500 600 0 100 200 300 400 500 600
R/H, Ohm/m R/H, Ohm/m
97 soggetti sani normopeso (nero), BPCO normopeso:
38 pazienti BPCO normopeso (rosso), 13 moderata (rosso),
30 Tumori polmonari (IV stadio)(verde); 25 grave (verde)
Hotelling’s T2 test: pNON E’ solo una questione di peso!
=Malnutrizione e BPCO/ Disfunzione muscolare
Patogenesi AMERI CAN T HORACI C SOCI ET Y
DOCUMENT S
An Official American Thoracic Society/European Respiratory Society
Statement: Update on Limb Muscle Dysfunction in Chronic Obstructive
Pulmonary Disease
François Maltais, Marc Decramer, Richard Casaburi, Esther Barreiro, Yan Burelle, Richard Debigaré,
P. N. Richard Dekhuijzen, Frits Franssen, Ghislaine Gayan-Ramirez, Joaquim Gea, Harry R. Gosker, Rik Gosselink,
BPCO Fumo
Maurice Hayot, Sabah N. A. Hussain, Wim Janssens, Micheal I. Polkey, Josep Roca, Didier Saey, Annemie
M. W. J. Schols, Martijn A. Spruit, Michael Steiner, Tanja Taivassalo, Thierry Troosters, Ioannis Vogiatzis, and
Peter D. Wagner; on behalf of the ATS/ERS Ad Hoc Committee on Limb Muscle Dysfunction in COPD
THIS OFFICIAL STATEMENT OF THE AMERICAN THORACIC SOCIETY (ATS) AND THE EUROPEAN RESPIRATORY SOCIETY (ERS) WAS APPROVED BY THE ATS BOARD OF
DIRECTORS, NOVEMBER 2013, AND BY THE ERS EXECUTIVE COMMITTEE, SEPTEMBER 2013
Ipercapnia Dispnea Capacità ossidativa Ipossia Consumo O2 Infiammazione Background: Limb muscle dysfunction is prevalent in chronic Results: We identified important advances in our understanding
obstructive pulmonary disease(COPD) and it hasimportant clinical of theextent and nature of thestructural alterations in limb muscles
muscolare
implications, such as reduced exercise tolerance, quality of life, in patients with COPD. Since the last update, landmark studies
and even survival. Since the previous American Thoracic Society/ were published on the mechanisms of development of limb muscle
European Respiratory Society (ATS/ERS) statement on limb dysfunction in COPD and on thetreatment of this condition. We
muscle dysfunction, important progress has been made on the now have a better understanding of theclinical implications of limb
TNF
characterization of this problem and on our understanding of its muscle dysfunction. Although exercise training is themost potent
pathophysiology and clinical implications. intervention to address this condition, other therapies, such as
neuromuscular electrical stimulation, are emerging. Assessment of
Purpose: The purpose of this document is to update the 1999 limb muscle function can identify patients who are at increased risk
ATS/ERSstatement on limb muscle dysfunction in COPD. of poor clinical outcomes, such asexerciseintoleranceand premature
Catecolamine Farmaci OCB→ Effetto termogenico Leptina Methods: An interdisciplinary committee of experts from theATS
and ERSPulmonary Rehabilitation and Clinical Problems assemblies
mortality.
determined that thescopeof thisdocument should belimited to Conclusions: Limb muscle dysfunction is a key systemic
dell’attività limb muscles. Committee members conducted focused reviews of the
literatureon several topics. A librarian alsoperformed aliteraturesearch.
consequenceof COPD. However, therearestill important gapsin our
knowledge about themechanisms of development of this problem.
An ATSmethodologist provided adviceto thecommittee, ensuring that Strategies for early detection and specific treatments for this
themethodological approach wasconsistent with ATSstandards. condition are also needed.
Overview dysfunction have been identified (e.g., Thepurposeof thisdocument isto update
deconditioning), much needs to be learned the 1999 American Thoracic Society/European
Limb muscle dysfunction is an important about the impact of other potential Respiratory Society (ATS/ERS) statement
systemic consequence of chronic obstructive contributors to this clinical manifestation in on limb muscle dysfunction. We intend to
Spesa energetica Apporto energetico/consumo
pulmonary disease (COPD) because of its COPD. Limb muscle dysfunction can be provide researchers and clinicians with the
impact on physical activity, exercise prevented and improved, in part, with recent advances in this field, with emphasis
tolerance, quality of life, and even survival in exercise training, but it is clear that novel on the following areas: (1) structural and
this disease. Although some mechanisms therapies are needed to better address this metabolic alterations found in limb muscles,
underlying the development of limb muscle problem. (2) consequences and clinical evaluation of
DEPLEZIONE NUTRIZIONALE
F.M. holds a CIHR/GSK Research Chair on COPD at Universit é Laval. R.C. holds the Grancell/Burns Chair in the Rehabilitative Sciences. E.B.’s contribution to
this statement was supported by CIBERES, FIS 11/02029, 2009-SGR-393, SEPAR 2010, FUCAP 2011, FUCAP 2012, and Marat ó TV3 (MTV3-07-1010)
(Spain) and by the ERS COPD Research Award 2008. M.I.P.’s contribution to this statement was supported by the NIHR Respiratory Disease Biomedical
Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College London, who partially fund his salary.
Am J Respir Crit Care Med Vol 189, Iss 9, pp e15–e62, May 1, 2014
Copyright © 2014 by the American Thoracic Society
DOI: 10.1164/rccm.201402-0373ST
Internet address: www.atsjournals.org
American Thoracic Society Documents e15
European Respiratory Monograph , vol 8 Monografia 24, March 2003; pag. 11-221998:158 Normal COPD
Possibili implicazioni terapeutiche
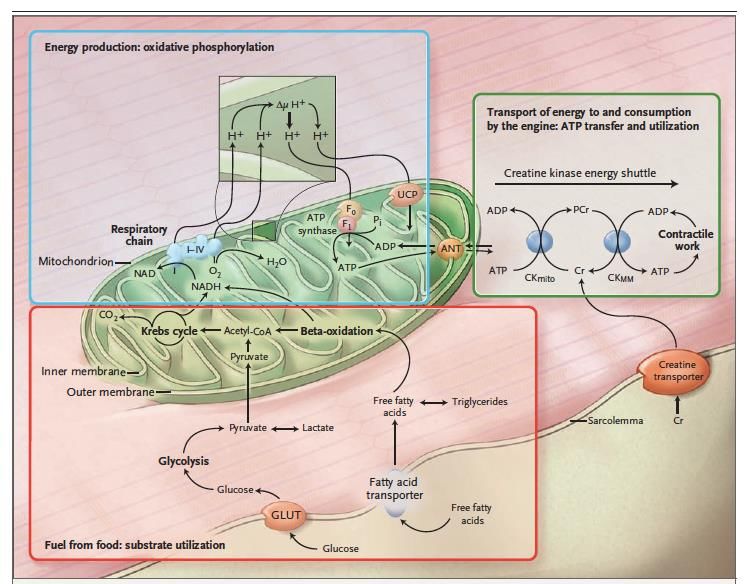
Energy Metabolism
Q10 (CoQ10):
• is a component of the electron transport chain and is
associated with inner mitochondrial complex III Q10
protein participates in aerobic cellular respiration
• a protective effect against mitochondria mediated
apoptosis and cell death
• reduction in mitochondrial-free radical generation
Creatine
Its use in humans as a therapeutic
agent was proved unsatisfactory, most
likely because of its poor solubility in
water, its limited solubility in lipids,
and its relatively high molecular weight
(863 g/mol), all result in poor oral A Synergic Action
bioavailability when combinedDOUBLE BLIND, RANDOMISED, MULTICENTER CLINICAL STUDY Multicenter study, longitudinal, prospective, randomized, controlled, double-blind versus placebo, conducted on two parallel groups: ➢ Eufortyn –Active group (47 pts) ➢ Placebo group (45 pts) in addition to standard therapy. A single cycle of integrative supplementation lasting 8 weeks, followed by an observational period (44 weeks) for a total of 52 wks Endpoints: - Primary: Exercise tolerance (6MW test) - Secondary: Body composition (by bioelectrical impedance)
Primary Endpoint: 6MW-Test
6MWT (m)
300
200
= V2-V1
0
• 6MWD significantly increased in Active
280
group (from 214±143 to 265±127 m;
-200 pSecondary Endpoint: Body Cell Mass %
BCM (%)
28
20 BCM definition:
= V2-V1
10
27 - the total mass of all the
0
cellular elements in the body,
-10 i.e. all the metabolically
26 active tissue of the body
Active Plac
- muscle tissue accounts for
approximately 60%, organ
25
tissue accounts for 20%, with
the remaining 20% made up of
24 red cells and tissue cells
23
Active
Placebo
22
V1 V2
The increment of BCM% in the Active group is
significantly greater (p=0.043) than that observed
in Placebo groupOther Secondary Endpoint
La REATTANZA (XC) è una misura indiretta dall’integrità delle
membrane cellulari ed è proporzionale alla massa cellulare corporea.
L'ANGOLO DI FASE (pHA) parametra nella diagnostica
bioimpedenziometrica l'integrità delle membrane cellulari e della
massa magra. L'angolo di fase rappresenta un importante indice
prognostico per monitorare la presenza e l'evoluzione dei processi
infiammatori cronici. L’aumento registrato nel gruppo attivo ha
permesso di passare a condizioni di normalità del parametro stesso.
* marks a significant change from V1 to V2 (paired Student t-test p-valueOBIETTIVO SECONDARIO DI CINETICA The plasma concentration of CoQ10 change positively in Active group.
Conclusioni 1 ✓Gli studi pubblicati sembrerebbero identificare un ruolo prognostico sfavorevole della perdita di peso e della riduzione della massa muscolare; ✓Gli effetti collaterali della terapia antifibrotica possono incidere significativamente sulla perdita di peso, soprattutto nella fase iniziale della terapia (incidendo soprattutto sulla massa grassa), l’influenza del peggioramento della malattia sembra incidere (sulla massa muscolare) ✓In ogni caso la presenza di malnutrizione proteico-calorica e la perdita di massa magra sono correlati con malattia più avanzata (DLCO) e minore capacità di esercizio.
Conclusioni 2 ✓La terapia antifibrotica (nintedanib) riduce il declino funzionale sia in pazienti con ridotto BMI all’esordio della malattia che nei pazienti con maggior perdita di peso. ✓Il ridotto BMI e la maggiore perdita di peso influenzano negativamente l’evoluzione funzionale indipendentemente dal trattamento (nintedanib) ✓Il monitoraggio dello stato nutrizionale nel paziente con fibrosi polmonare idiopatica, in particolare in presenza di calo ponderale , può fornire utili indicazioni soprattutto in senso prognostico. ✓Molto c’è ancora da chiarire sul possibile ruolo di diete personalizzate che possano mitigare gli effetti collaterali della terapia e, in alcuni casi evitarne la interruzione. ✓Non esistono dati relativi al possibile trattamento farmacologico o nutraceutico della malnutrizione nei pazienti con fibrosi idiopatica
Puoi anche leggere