Elotuzumab, lenalidomide, and dexamethasone as salvage therapy for patients with multiple myeloma: Italian, multicenter, retrospective clinical ...
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
Published Ahead of Print on February 27, 2020, as doi:10.3324/haematol.2019.241513.
Copyright 2020 Ferrata Storti Foundation.
Elotuzumab, lenalidomide, and dexamethasone as salvage
therapy for patients with multiple myeloma: Italian, multicenter,
retrospective clinical experience with 300 cases outside of
controlled clinical trials
by Massimo Gentile, Giorgina Specchia, Daniele Derudas, Monica Galli, Cirino Botta, Stefano Rocco,
Concetta Conticello, Catello Califano, Nicola Giuliani, Silvia Mangiacavalli, Enrico Attingenti,
Alessandra Lombardo, Marino Brunori, Elena Rossi, Elisabetta Antonioli, Roberto Ria, Renato Zam-
bello, Nicola Di Renzo, Giuseppe Mele, Gianpaolo Marcacci, Pellegrino Musto, Silvana Capalbo, Ni-
cola Cascavilla, Claudio Cerchione, Angelo Belotti, Clelia Criscuolo, Giuseppina Uccello, Paola Curci,
Ernesto Vigna, Vincenzo Fraticelli, Donatella Vincelli, Angela Bonalumi, Agostina Siniscalchi, Raffaella
Stocchi, Massimo Martino, Stelvio Ballanti, Dominella Gangemi, Alfredo Gagliardi, Barbara Gamberi,
Alessandra Pompa, Anna Grazia Recchia, Giovanni Tripepi, Annalisa Pitino, Ferdinando Frigeri, Ugo
Consoli, Sara Bringhen, Elena Zamagni, Francesca Patriarca, Valerio De Stefano, Francesco Di Rai-
mondo, Salvatore Palmieri, Maria Teresa Petrucci, Massimo Offidani, Mario Boccadoro, Michele Cavo,
and Fortunato Morabito
Haematologica 2020 [Epub ahead of print]
Citation: Massimo Gentile, Giorgina Specchia, Daniele Derudas, Monica Galli, Cirino Botta, Stefano Rocco,
Concetta Conticello, Catello Califano, Nicola Giuliani, Silvia Mangiacavalli, Enrico Attingenti, Alessandra
Lombardo, Marino Brunori, Elena Rossi, Elisabetta Antonioli, Roberto Ria, Renato Zambello, Nicola Di
Renzo, Giuseppe Mele, Gianpaolo Marcacci, Pellegrino Musto, Silvana Capalbo, Nicola Cascavilla,
Claudio Cerchione, Angealo Belotti, Clelia Criscuolo, Giuseppina Uccello, Paola Curci, Ernesto Vigna,
Vincenzo Fraticelli, Donatella Vincelli, Angela Bonalumi, Agostina Siniscalchi, Raffaella Stocchi, Massimo
Martino, Stelvio Ballanti, Dominella Gangemi, Alfredo Gagliardi, Barbara Gamberi, Alessandra Pompa,
Anna Grazia Recchia, Giovanni Tripepi, Annalisa Pitino, Ferdinando Frigeri, Ugo Consoli, Sara Bringhen,
Elena Zamagni, Francesca Patriarca, Valerio De Stefano, Francesco Di Raimondo, Salvatore Palmieri,
Maria Teresa Petrucci, Massimo Offidani, Mario Boccadoro, Michele Cavo, and Fortunato Morabito.
Elotuzumab, lenalidomide, and dexamethasone as salvage therapy for patients with multiple myeloma:
Italian, multicenter, retrospective clinical experience with 300 cases outside of controlled clinical trials
Haematologica. 2020; 105:xxx
doi:10.3324/haematol.2019.241513
Publisher's Disclaimer.
E-publishing ahead of print is increasingly important for the rapid dissemination of science.
Haematologica is, therefore, E-publishing PDF files of an early version of manuscripts that
have completed a regular peer review and have been accepted for publication. E-publishing
of this PDF file has been approved by the authors. After having E-published Ahead of Print,
manuscripts will then undergo technical and English editing, typesetting, proof correction and
be presented for the authors' final approval; the final version of the manuscript will then
appear in print on a regular issue of the journal. All legal disclaimers that apply to the
journal also pertain to this production process.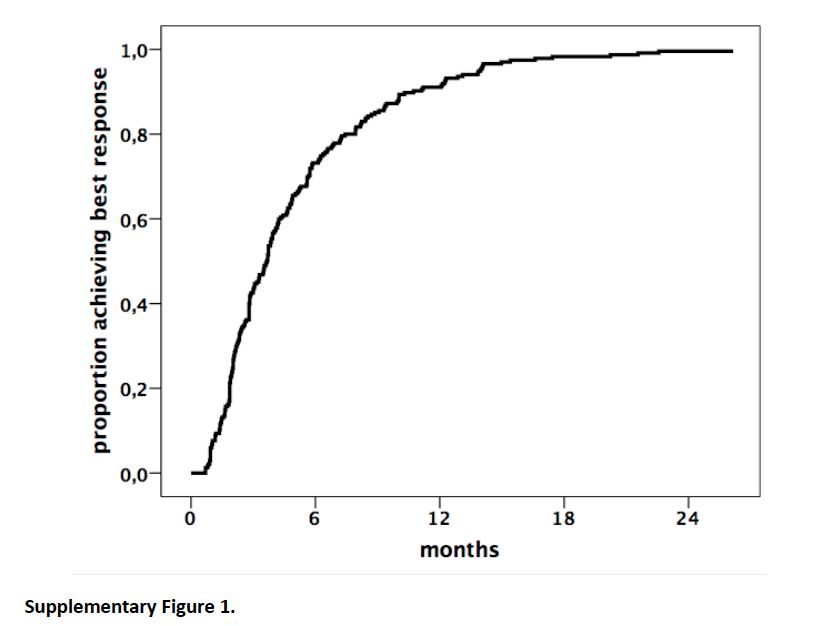
Elotuzumab, lenalidomide, and dexamethasone as salvage therapy for
patients with multiple myeloma: Italian, multicenter, retrospective clinical
experience with 300 cases outside of controlled clinical trials
Massimo Gentile1,2, Giorgina Specchia3, Daniele Derudas4, Monica Galli5, Cirino
Botta1,2, Stefano Rocco6, Concetta Conticello7, Catello Califano8, Nicola Giuliani9, Silvia
Mangiacavalli10, Enrico Attingenti11, Alessandra Lombardo12, Marino Brunori13, Elena
Rossi14, Elisabetta Antonioli15, Roberto Ria16, Renato Zambello17, Nicola Di Renzo18,
Giuseppe Mele19, Gianpaolo Marcacci20, Pellegrino Musto21, Silvana Capalbo22, Nicola
Cascavilla23, Claudio Cerchione24, Angelo Belotti25, Clelia Criscuolo26, Giuseppina
Uccello27, Paola Curci3, Ernesto Vigna1,2, Vincenzo Fraticelli1,2, Donatella Vincelli28,
Angela Bonalumi29, Agostina Siniscalchi30, Raffaella Stocchi31, Massimo Martino32,
Stelvio Ballanti33, Dominella Gangemi34, Alfredo Gagliardi35, Barbara Gamberi36,
Alessandra Pompa37, Anna Grazia Recchia2, Giovanni Tripepi38, Annalisa Pitino39,
Ferdinando Frigeri11, Ugo Consoli27, Sara Bringhen40, Elena Zamagni41, Francesca
Patriarca31, Valerio De Stefano14, Francesco Di Raimondo7, Salvatore Palmieri6, Maria
Teresa Petrucci42, Massimo Offidani43, Mario Boccadoro40, Michele Cavo41, Fortunato
Morabito2,44.
1
Hematology Unit, Azienda Ospedaliera of Cosenza, Cosenza, Italy; 2Biotechnology
Research Unit, AO di Cosenza, Italy; 3Hematology Section, University of Bari, Italy;
4
Department of Hematology, Businco Hospital, Cagliari, Italy; 5Hematology and Bone
Marrow Transplant Unit, Azienda Socio-Sanitaria Territoriale-Papa Giovanni XXIII,
Bergamo, Italy; 6Hematology Unit, Ospedale Cardarelli, Napoli, Italy; 7Department of
medical and surgical specialties, Hematology Section, University of Catania, Catania,
8
Italy; Onco-hematology Unit, Ospedale Umberto I, Nocera Inferiore, Italy;
9 10
Hematology Unit, Parma University Hospital, Italy; Hematology Division,
Department of Hematology-Oncology, IRCCS Fondazione Policlinico San Matteo,
11
Pavia, Italy; UOC Ematologia a Indirizzo Oncologico, AORN “Sant’Anna e San
Sebastiano”, Caserta, Italy; 12Onco-hematology Unit Azienda Ospedaliera Santa Maria
of Terni, Italy; 13Internal Medicine, Ospedale S. Croce, Azienda Ospedaliera Ospedali
14
Riuniti Marche Nord, Presidio of Fano, Italy; Istituto di Ematologia, Università
15
Cattolica, Fondazione Policlinico Gemelli IRCCS, Roma, Italy; Hematology Unit,
116
Careggi Hospital, Florence, Italy; Department of Biomedical Science, University of
Bari "Aldo Moro" Medical School, Internal Medicine "G. Baccelli", Policlinico, Bari,
Italy; 17Department of Medicine, Hematology and Clinical Immunology Section, Padua
18
University School of Medicine, Padua, Italy; Hematology Unit, Lecce, Italy;
19 20
Hematology Unit, Brindisi, Italy; Hematology and Bone Marrow Transplant Unit,
21
Istituto Nazionale Tumori, Fondazione 'G. Pascale', IRCCS, Napoli, Italy; Unit of
Hematology and Stem Cell Transplantation, IRCCS-CROB, Referral Cancer Center of
22
Basilicata, Rionero in Vulture (Pz), Italy; Department of Hematology, Hospital
23
University Riuniti, Foggia, Italy; Department of Hematology and Bone Marrow
Transplant, IRCCS Casa Sollievo della Sofferenza, San Giovanni Rotondo, Italy;
24
Hematology Unit, IRCCS - Istituto Scientifico Romagnolo per lo Studio e la Cura dei
25
Tumori, Meldola, Italy; Hematology Unit, A.O. Spedali Civili, Brescia, Italy;
26
Hematology Unit, AO S.G. Moscati, Aversa (CE), Italy; 27Hematology Department, G.
Garibaldi Hospital, Catania, Italy; 28Hematology Unit, Department of Hemato-Oncology
and Radiotherapy, Great Metropolitan Hospital "Bianchi-Melacrino-Morelli", Reggio
29
Calabria, Italy; Section of Hematology, Department of Medicine, University of
30
Verona, Verona, Italy; Hematology Unit and Pathology Department, S. Eugenio
31 32
Hospital Rome, Rome, Italy; Hematology, DISM, University of Udine, Italy; Stem
Cell Transplantation Unit, Department of Hemato-Oncology and Radiotherapy, Great
Metropolitan Hospital "Bianchi-Melacrino-Morelli", Reggio Calabria, Italy; 33Institute
of Haematology and Stem Cell transplantation, Ospedale Santa Maria della
34
Misericordia, University of Perugia, Perugia, Italy; Hematology Unit, Fabrizio
Spaziani Hospital, Frosinone, Italy; 35Complex Operative Unit of Hematology, S. Maria
36
di Loreto Nuovo Hospital, Napoli, Italy; Hematology Unit, AUSL-IRCCS, Reggio
37
Emilia, Italy; Hematology Unit, Fondazione IRCCS Ca' Granda, Ospedale Maggiore
38
Policlinico, Milano, Italy; Nephrology Center of National Research Institute of
39
Biomedicine and Molecular Immunology, Reggio Calabria, Italy; CNR-IFC, Roma,
40
Italy; Division of Hematology, University of Torino, AOU Città della Salute e della
41
Scienza di Torino, Italy; Seràgnoli Institute of Hematology and Medical Oncology,
42
University of Bologna, Bologna, Italy; Department of Cellular Biotechnologies and
43
Hematology, Sapienza University of Rome, Italy; Hematology Unit, AOU Ospedali
44
Riuniti di Ancona, Italy; Hemato-Oncology Department, Augusta Victoria Hospital of
Jerusalem, Israel.
2Correspondence: Massimo Gentile, MD, Hematology Unit, AO of Cosenza, Italy; 87100
Cosenza, Italy; e-mail: massim.gentile@tiscali.it; ph: +39-0984-681329; fax: +39-0984-
681329.
Text word count: 1500; Table: 2; Figure: 1; Online Supplementary Table: 1; Online
Supplementary Figures: 5; Supplementary References 2.
References: 15.
Article Type: Letter to the Editor
Running title: An Italian real-life experience on EloRd for RRMM
Keywords: Elotuzumab, lenalidomide, dexamethasone, multiple myeloma, salvage therapy.
3Recently, monoclonal antibodies (mAbs) directed to antigens expressed by plasma cells
demonstrated major clinical activity in multiple myeloma (MM), thus gaining a relevant role
in the treatment of MM patients (1). Two mAbs targeting signaling lymphocytic activation
molecule F7 (SLAMF7/CS1) and CD38 have been increasingly included in relapse/refractory
(RR) MM (RRMM) therapeutic regimens (2). Among them, Elotuzumab (Elo), targets the
glycoprotein receptor SLAMF7 causing on one side activation of natural killer cells and on
the other side, myeloma cell death through antibody-dependent cellular cytotoxicity (ADCC)
(3,4). Surprisingly, Elo failed to demonstrate significant anti-tumor activity as single-agent
(5), ultimately refining its anti-myeloma action in combination with IMiDs such as
lenalidomide (R). A randomized phase 3 clinical trial comparing the clinical benefits of R
plus dexamethasone (Rd) versus Rd plus Elo (EloRd) resulted in a longer progression-free
survival (PFS) in patients allocated to the experimental arm (6). Moreover, extended
assessments at 3-(7), 4- (8), and 5-year follow-ups (9) showed a significantly higher overall
response rate (ORR) for EloRd as compared to the Rd regimen. Accordingly, the addition of
Elo to Rd significantly reduced death risk by 27% (8).
Here we report data of an Italian real-life experience on EloRd as therapy for RRMM patients
treated outside of controlled clinical trials, after marketing approval in Italy on April 2017.
Overall, 300 RRMM patients treated with EloRd, according on marketing approved schedule,
between April 2017 and April 2019 at 40 Italian centers entered this study (Online
Supplementary Methods). Baseline characteristics are shown in Table 1. Approximately one
fourth of patients (24.3%) had resistance to their most recent line of therapy, symptomatic
relapse was observed in 171 patients (57%) and a biochemical relapse in 56 (18.7%). Over
one third (38.3%) received autologous stem cell transplant (ASCT), while 26% of patients
had received prior lenalidomide treatment. FISH data were available in only 64 patients; 10
patients showed high-risk abnormalities. Thirty patients with mild renal impairment received
4R at the starting dose of 10 mg, while 24 with severe renal impairment at the staring dose of
15 mg every other day; 123 elderly patients (>75 years) received d at a weekly dose of 20 mg.
At the time of last database update, the median number of courses administered was 12 (range
1–43). A total of 188 (62.7%) patients stopped EloRd treatment at the time of the cutoff date
[median follow-up: 19 months (range 1–36 months)] mainly owing to disease progression
(151 cases), 13 patients for toxicity (9 infections, 2 lenalidomide-related severe skin rash, 1
dexamethasone-related psychosis, and 1 lenalidomide-related hepatotoxicity), 22 patients due
to therapy-unrelated deaths, while 2 patients underwent ASCT. Infusion reactions occurred in
19 patients (6.3%, all grade 1-2) and were promptly resolved in all patients (no
discontinuation reported). Major adverse events (AEs) are depicted in Table 2 and included
grade 3/4 neutropenia (19%), anemia (15.7%), lymphocytopenia (12.7%), and
thrombocytopenia (10%) while infection rates and pneumonia were roughly 34% and 16%,
respectively. Notably, the incidence of AEs was not significantly different between younger
(75 years. Of note, no significant
5differences in terms of AEs incidence were documented between younger (
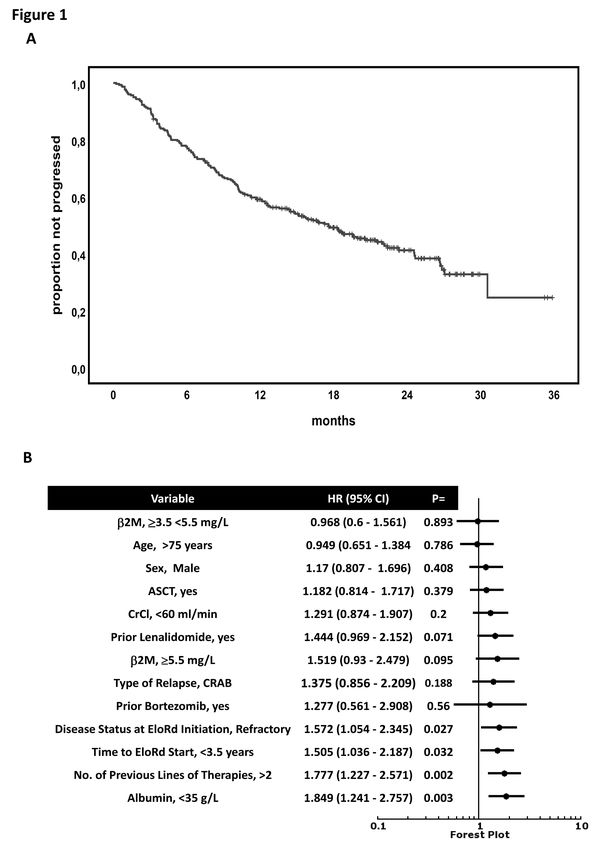
the 1-year PFS was 59.1% (Figure 1A), both results were very similar to the 19.4 months and 68% determined in the Eloquent-2 trial (6). Univariate Cox analyses showed that refractory disease status at EloRd initiation (HR:1.572, 95%CI 1.054-2.345, P=0.027), a shorter time (i.e.
80.1% (HR:1, reference group), 59% (HR:2.15, 95%CI 1.46–3.16, P
Conflict-of-interest disclosure: Nothing to disclose
9REFERENCES
1. Touzeau C, Moreau P, Dumontet C. Monoclonal antibody therapy in multiple
myeloma. Leukemia. 2017;31(5):1039-1047.
2. Durer C, Durer S, Lee S, et al. Treatment of relapsed multiple myeloma: Evidence-
based recommendations. Blood Rev. 2020; 39:100616.
3. Collins SM, Bakan CE, Swartzel GD, et al. Elotuzumab directly enhances NK cell
cytotoxicity against myeloma via CS1 ligation: evidence for augmented NK cell function
complementing ADCC. Cancer Immunol Immunother. 2013;62(12):1841-1849.
4. Hsi ED, Steinle R, Balasa B, et al. CS1, a potential new therapeutic antibody target
for the treatment of multiple myeloma. Clin Cancer Res. 2008;14(9):2775-2784.
5. Zonder JA, Mohrbacher AF, Singhal S, et al. A phase 1, multicenter, open-label,
dose escalation study of elotuzumab in patients with advanced multiple myeloma.
Blood. 2012;120(3):552-559.
6. Lonial S, Dimopoulos M, Palumbo A, et al. Elotuzumab Therapy for Relapsed or
Refractory Multiple Myeloma. N Engl J Med. 2015;373(7):621-631.
7. Dimopoulos MA, Lonial S, White D, et al. Elotuzumab plus
lenalidomide/dexamethasone for relapsed or refractory multiple myeloma: ELOQUENT-
2 follow-up and post-hoc analyses on progression-free survival and tumour growth. Br J
Haematol. 2017;178(6):896-905.
8. Dimopoulos MA, Lonial S, Betts KA, et al. Elotuzumab plus lenalidomide and
dexamethasone in relapsed/refractory multiple myeloma: Extended 4-year follow-up
and analysis of relative progression-free survival from the randomized ELOQUENT-2
trial. Cancer. 2018;124(20):4032-4043.
9. Lonial S, Dimopoulos MA, Weisel K, et al. Extended 5-y follow-up (FU) of phase 3
ELOQUENT-2 study of elotuzumab + lenalidomide/dexamethasone (ELd) vs Ld in
relapsed/refractory multiple myeloma (RRMM). J Clin Oncol. 2018;36(15_suppl):8040.
10. Willan J, Eyre TA, Sharpley F, Watson C, King AJ, Ramasamy K. Multiple myeloma
in the very elderly patient: challenges and solutions. Clin Interv Aging. 2016;11:423-435.
11. Offidani M, Corvatta L. A review discussing elotuzumab and its use in the second-
line plus treatment of multiple myeloma. Future Oncol. 2018;14(4):319-329.
12. Moreau P, San Miguel J, Sonneveld P, et al. Multiple myeloma: ESMO Clinical
Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol.
2017;28(suppl_4):iv52-iv61.
13. Network NCC. multiple myeloma (version 4.2018). [cited 9 Aug 2018]; Available
from: http://www.nccn.org/
14. Dimopoulos MA, Dytfeld D, Grosicki S, et al. Elotuzumab plus Pomalidomide and
Dexamethasone for Multiple Myeloma. N Engl J Med. 2018;379(19):1811-1822.
15. Thomas SK, Shah JJ, Morphey AN, et al. Updated Results of a Phase II Study of
Lenalidomide-Elotuzumab As Maintenance Therapy Post-Autologous Stem Cell
Transplant (AuSCT) in Patients (Pts) with Multiple Myeloma (MM). Blood.
2018;132(Suppl 1):1982.
10Table 1. Main characteristics of patients at baseline
No. of patients (%)
Age, (years)* Patients harboring a t(4;14), t(14;16), or del(17p) were classified as having high-risk disease
and all other cases as being at standard risk.
12Table 2. Incidence of serious adverse events
EloRd (N=300)
Grade 3/4 adverse events No of cases (%)
Hematological toxicities
Lymphocytopenia 38 (12.7)
Anemia 47 (15.7)
Thrombocytopenia 30 (10)
Neutropenia 57 (19)
Non-hematological toxicities
Infections 103 (34.3)
Pneumonia 50 (16.7)
Fatigue 62 (20.7)
Diarrhea 22 (7.3)
13Figures legend
Figure 1. Progression-free survival of the retrospective cohort of RRMM patients treated with
EloRd. Kaplan-Meier curve of progression-free survival of the entire cohort (A). Forest plot
of Cox univariate analysis for progression-free survival according to clinical laboratory
variables (B).
14ONLINE SUPPLEMENTARY CONTENTS
Elotuzumab, lenalidomide, and dexamethasone as salvage therapy for patients
with multiple myeloma: Italian, multicenter, retrospective clinical experience
with 300 cases outside of controlled clinical trials
Massimo Gentile1,2, Giorgina Specchia3, Daniele Derudas4, Monica Galli5, Cirino Botta1,2,
Stefano Rocco6, Concetta Conticello7, Catello Califano8, Nicola Giuliani9, Silvia
Mangiacavalli10, Enrico Attingenti11, Alessandra Lombardo12, Marino Brunori13, Elena Rossi14,
Elisabetta Antonioli15, Roberto Ria16, Renato Zambello17, Nicola Di Renzo18, Giuseppe Mele19,
Gianpaolo Marcacci20, Pellegrino Musto21, Silvana Capalbo22, Nicola Cascavilla23, Claudio
Cerchione24, Angelo Belotti25, Clelia Criscuolo26, Giuseppina Uccello27, Paola Curci3, Ernesto
Vigna1,2, Vincenzo Fraticelli1,2, Donatella Vincelli28, Angela Bonalumi29, Agostina Siniscalchi30,
Raffaella Stocchi31, Massimo Martino32, Stelvio Ballanti33, Dominella Gangemi34, Alfredo
Gagliardi35, Barbara Gamberi36, Alessandra Pompa37, Anna Grazia Recchia2, Giovanni
Tripepi38, Annalisa Pitino39, Ferdinando Frigeri11, Ugo Consoli27, Sara Bringhen40, Elena
Zamagni41, Francesca Patriarca31, Valerio De Stefano14, Francesco Di Raimondo7, Salvatore
Palmieri6, Maria Teresa Petrucci42, Massimo Offidani43, Mario Boccadoro40, Michele Cavo41,
Fortunato Morabito2,44.
1
Hematology Unit, Azienda Ospedaliera of Cosenza, Cosenza, Italy; 2Biotechnology Research
Unit, AO di Cosenza, Italy; 3Hematology Section, University of Bari, Italy; 4Department of
Hematology, Businco Hospital, Cagliari, Italy; 5Hematology and Bone Marrow Transplant
Unit, Azienda Socio-Sanitaria Territoriale-Papa Giovanni XXIII, Bergamo, Italy; 6Hematology
Unit, Ospedale Cardarelli, Napoli, Italy; 7Department of medical and surgical specialties,
Hematology Section, University of Catania, Catania, Italy; 8Onco-hematology Unit, Ospedale
Umberto I, Nocera Inferiore, Italy; 9Hematology Unit, Parma University Hospital, Italy;
10
Hematology Division, Department of Hematology-Oncology, IRCCS Fondazione Policlinico
San Matteo, Pavia, Italy; 11UOC Ematologia a Indirizzo Oncologico, AORN “Sant’Anna e San
12
Sebastiano”, Caserta, Italy; Onco-hematology Unit Azienda Ospedaliera Santa Maria of
13
Terni, Italy; Internal Medicine, Ospedale S. Croce, Azienda Ospedaliera Ospedali Riuniti
14
Marche Nord, Presidio of Fano, Italy; Istituto di Ematologia, Università Cattolica,
15
Fondazione Policlinico Gemelli IRCCS, Roma, Italy; Hematology Unit, Careggi Hospital,
Florence, Italy; 16Department of Biomedical Science, University of Bari "Aldo Moro" Medical
17
School, Internal Medicine "G. Baccelli", Policlinico, Bari, Italy; Department of Medicine,Hematology and Clinical Immunology Section, Padua University School of Medicine, Padua,
18 19 20
Italy; Hematology Unit, Lecce, Italy; Hematology Unit, Brindisi, Italy; Hematology and
Bone Marrow Transplant Unit, Istituto Nazionale Tumori, Fondazione 'G. Pascale', IRCCS,
Napoli, Italy; 21Unit of Hematology and Stem Cell Transplantation, IRCCS-CROB, Referral
22
Cancer Center of Basilicata, Rionero in Vulture (Pz), Italy; Department of Hematology,
23
Hospital University Riuniti, Foggia, Italy; Department of Hematology and Bone Marrow
Transplant, IRCCS Casa Sollievo della Sofferenza, San Giovanni Rotondo, Italy; 24Hematology
Unit, IRCCS - Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori, Meldola,
25 26
Italy; Hematology Unit, A.O. Spedali Civili, Brescia, Italy; Hematology Unit, AO S.G.
Moscati, Aversa (CE), Italy; 27Hematology Department, G. Garibaldi Hospital, Catania, Italy;
28
Hematology Unit, Department of Hemato-Oncology and Radiotherapy, Great Metropolitan
29
Hospital "Bianchi-Melacrino-Morelli", Reggio Calabria, Italy; Section of Hematology,
30
Department of Medicine, University of Verona, Verona, Italy; Hematology Unit and
31
Pathology Department, S. Eugenio Hospital Rome, Rome, Italy; Hematology, DISM,
University of Udine, Italy; 32Stem Cell Transplantation Unit, Department of Hemato-Oncology
and Radiotherapy, Great Metropolitan Hospital "Bianchi-Melacrino-Morelli", Reggio
33
Calabria, Italy; Institute of Haematology and Stem Cell transplantation, Ospedale Santa
Maria della Misericordia, University of Perugia, Perugia, Italy; 34Hematology Unit, Fabrizio
35
Spaziani Hospital, Frosinone, Italy; Complex Operative Unit of Hematology, S. Maria di
Loreto Nuovo Hospital, Napoli, Italy; 36Hematology Unit, AUSL-IRCCS, Reggio Emilia, Italy;
37
Hematology Unit, Fondazione IRCCS Ca' Granda, Ospedale Maggiore Policlinico, Milano,
38
Italy; Nephrology Center of National Research Institute of Biomedicine and Molecular
39 40
Immunology, Reggio Calabria, Italy; CNR-IFC, Roma, Italy; Division of Hematology,
41
University of Torino, AOU Città della Salute e della Scienza di Torino, Italy; Seràgnoli
Institute of Hematology and Medical Oncology, University of Bologna, Bologna, Italy;
42
Department of Cellular Biotechnologies and Hematology, Sapienza University of Rome, Italy;
43
Hematology Unit, AOU Ospedali Riuniti di Ancona, Italy; 44Hemato-Oncology department,
Augusta Victoria Hospital of Jerusalem, Israel.
Correspondence: Massimo Gentile, MD, Hematology Unit, AO of Cosenza, Italy; 87100
Cosenza, Italy; e-mail: massim.gentile@tiscali.it; ph: +39-0984-681329; fax: +39-0984-681329.
Text word count: 1500; Table: 2; Figure: 1; Online Supplementary Table: 1; Online Supplementary
Figures: 5; Supplementary References 2.
References: 15.Article Type: Letter to the Editor Running title: An Italian real-life experience on EloRd for RRMM Keywords: Elotuzumab, lenalidomide, dexamethasone, multiple myeloma, salvage therapy. Supplementary Methods Supplementary References Supplementary Tables Supplementary Figures
Methods Databases from 40 Italian centers including all patients with RRMM treated with EloRd were established for research purposes. The databases contained clinical information such as age, sex, date of diagnosis, laboratory parameters, treatment history, and date of last follow-up or death abstracted from clinical records at the time of inclusion and updated on an ongoing basis. The 40 databases included 300 consecutive cases of RRMM who received at least one cycle of EloRd as salvage treatment between April 2017 and April 2019. All patients were treated with EloRd according to marketing approval as follows: Elo 10 mg/kg i.v. on days 1, 8, 15, and 22 during the first two cycles and then on days 1 and 15 of each following cycle, R 25 mg on days 1 to 21 of each cycle and d at a dose of 40 mg during the week without Elo, and 36 mg on the day of Elo administration. Patients received premedication with diphenhydramine (25 to 50 mg) or its equivalent, ranitidine (50 mg) or its equivalent, and acetaminophen (650 to 1000 mg) or its equivalent 30 to 90 minutes before the Elo infusion. Lenalidomide starting dose was adjusted according renal function. Elderly patients (>75 years) received d at a weekly dose of 20 mg. Response to treatment and disease progression were evaluated according the IMWG criteria(1, 2). Responsive patients had to reach at least a partial remission (PR). In all patients on EloRd antibacterial, antiviral, and antithrombotic prophylaxis was prescribed. The study was approved by institutional ethics committees according to the principles of the Declaration of Helsinki. For categorical variables, statistical comparisons were performed using two-way tables for the Fisher’s exact test and multi-way tables for the Pearson’s Chi-square test. To account for multiple testing, a Bonferroni correction was applied. Multivariate ordinal regression analysis was used to examine the effects of potential confounders on the association between the best response and several variables that were statistically significant on univariate analysis by Pearson chi-square or Fisher's exact test. In light of the etiological nature of our study, in this analysis, we introduced all variables
which significantly differed (P
References 1. Durie BG, Harousseau JL, Miguel JS, et al. International uniform response criteria for multiple myeloma. Leukemia. 2006;20(9):1467-1473. 2. Rajkumar SV, Harousseau JL, Durie B, et al. Consensus recommendations for the uniform reporting of clinical trials: report of the International Myeloma Workshop Consensus Panel 1. Blood. 2011;117(18):4691-4695.
Supplementary Table 1. Association between best response and main clinical-hematological
characteristics of multiple myeloma patients treated with EloRd
Variable CR + VGPR PR + MR SD + PD
N (%) N (%) N (%) P
Sex
Female 48 (33.6) 70 (49) 25 (17.4) 0.14
Male 63 (40.1) 58 (36.9) 36 (22.8)
Age
£75 61 (34.5) 78 (44.1) 38 (21.5) 0.55
>75 50 (40.7) 50 (40.7) 23 (18.7)
CrCl mL/min
³60 75 (35) 95 (44.4) 44 (20.6) 0.53Supplementary Figures legend Supplementary Figure 1. Time to achieve best response. Supplementary Figure 2. Progression-free survival by cytogenetic risk. Supplementary Figure 3. Progression-free survival by tumor response to EloRd. Supplementary Figure 4. Kaplan-Meier curve of time to next treatment of the entire cohort. Supplementary Figure 5. Kaplan-Meier curve of overall survival of the entire cohort.
Puoi anche leggere