New Paradigm for the Management of Recurrences from Clostridium difficile infections (rCDI) - MSD Salute
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
New Paradigm for the Management of Recurrences
from Clostridium difficile infections (rCDI)
Torino 4 Dicembre 2018
Francesco G. De Rosa
SCDU Malattie Infettive 2
AOU Città della Salute & Scienza, Torino
&
Ospedale Cardinal Massaia, Asti
AINF-1280702-0000-ZIN-W-02-2020
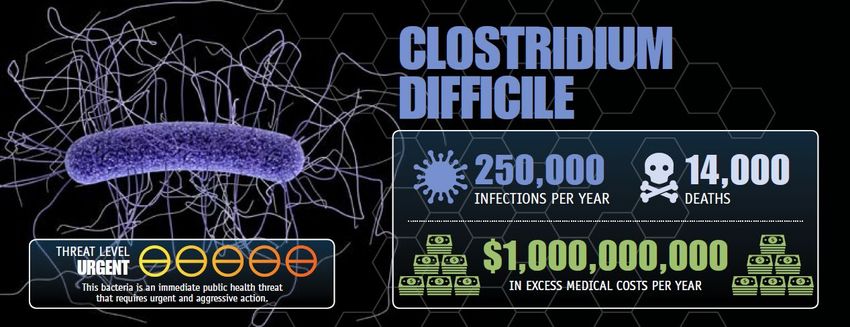
Clostridium difficile in USA ANTIBIOTIC RESISTANCE THREATS in the United States, 2013; US Dep. of Health and Human Services, CDC
C. difficile Infection:
Clinical Outcomes in Patients with Cancer
• In a retrospective cohort study of adult out- or
inpatients with CDI, patients with cancer had higher
30-day mortality than non-cancer patients
(OR 1.44; 95% CI 1.33-1.55) [1].
• CDI patients with hematologic malignancies had
higher mortality than solid tumor patients
(OR 1.85; 95% CI 1.56-2.19) [1].
• Determining C. difficile ribotypes in cancer patients with CDI is relevant: patients with ribotype
014-20 experienced similar rates of response to therapy but fewer complications [2].
1. #E0168 - Delgado A, et al. Cancer as a predictor of poor outcomes in Clostridium difficile infection among a national cohort of United States veterans
2. #E0166 - Yepez Guevara E, et al. Relevance of Clostridium difficile ribotype 014-20 in cancer patients with diarrhea
Recidiva di CDI: Terapia
Linee Guida ESCMID & IDSA
Le linee guida ESCMID & IDSA raccomandano :
– Vancomicina/Metronidazolo: CDI lieve moderata
– Vancomicina/Fidaxomicinaa: CDI grave
ESCMID1 IDSA2
First recurrence Vancomycin or metronidazole Vancomycin or fidaxomicin
Vancomycin or fidaxomicin
Second or multiple recurrence Vancomycin or fidaxomicin
No pharmacologic treatment No pharmacologic treatment
Prevention of recurrence
recommendation recommendation
CDI = C. difficile infection; ESCMID = European Society of Clinical Microbiology and Infectious Diseases; IDSA = Infectious Diseases Society of
America; rCDI = recurrent C. difficile infection. a. No data on efficacy in severe life-threatening disease and/or toxic megacolon. 1. Debast SB et al.
Clin Microbiol Infect. 2014;20(suppl 2):S1‒S26 2. LC.McDonald et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and
Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clinical
Infectious Diseases® 2018;XX(00):1–48
Recurrent CDI: FADOI-PRACTICE
10,780 patients:
103 (0.96 %) had CDI
Recurrent CDI = 14.6 %
Overall Incidence
5.3/10,000 patient-days
In-hospital mortality
16.5 % CD group
6.7% No-CD group
(p < 0.001)
Median length of hospital stay
16 days (IQR = 13; CDI)
8 days (IQR = 8; No CDI)
Cioni et al. BMC Infectious Diseases (2016) 16:656
Fattori di Rischio per Recidiva di CDI
Includono:
Età avanzata (>65 anni),
Precedente episodio di CDI,
Stato di immunocompromissione,
CDI severa,
Prolungata ospedalizzazione,
Infezione sostenuta dal ribotipo 027,
Esposizione ad antibiotici (in particolareclindamicina, fluorochinoloni, amoxicillina,
cefalosporine) e chemioterapici
Utilizzo di antiacidi, inibitori di pompa,
Comorbidità (quali malattia renale cronica, diabete, neoplasie, diverticolosi intestinale,
malattia infiammatoria intestinale),
Chirurgia del tratto gastro-intestinale
Nutrizione enterale
Johnson S. J Infect. 2009 Jun;58(6):403-10. Garey KW, J Hosp Infect. 2008 Dec;70(4):298-304. Leffler DA, N Engl J Med. 2015 Apr
16;372(16):1539-48). Wilcox M,. Lancet 357(9251), 158–159 (2001); Debast SB et al. Clin Microbiol Infect. 2014;20(suppl
2):S1‒S26 Neemann K, Freifeld A. Clostridium difficile-associated diarrhea in the oncology patient. J Oncol Pract. 2017;13(1):25-30;
McFarland. Curr Opin Gastroenterol 2009;25:24–3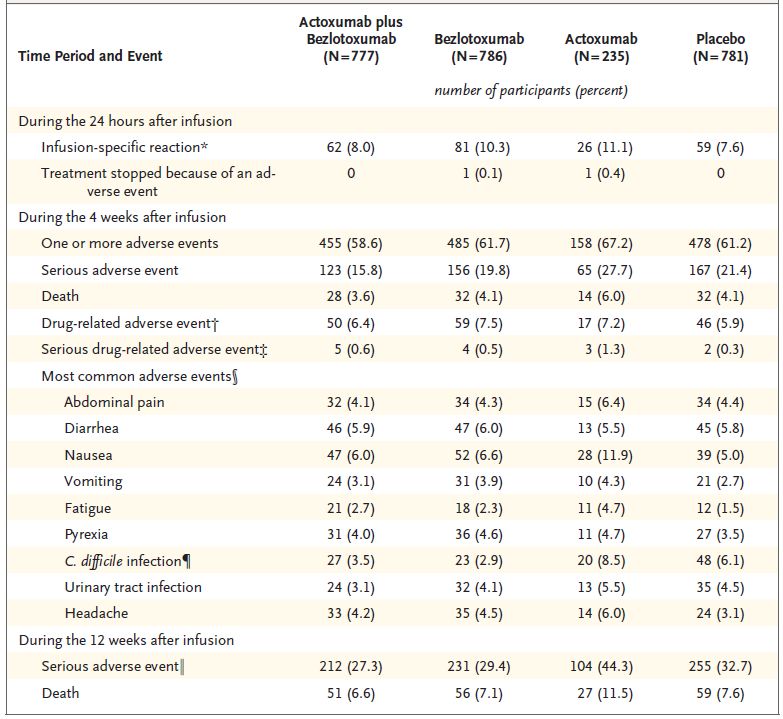
Fattori di Rischio per Recidiva di CDI
I fattori di rischio sono correlati ad una inadeguata risposta anticorpale
anti-tossina e ad una persistente alterazione della flora microbica del colon
Includono:
Età avanzata (>65 anni),
Precedente episodio di CDI,
Stato di immunocompromissione,
CDI severa,
Prolungata ospedalizzazione,
Infezione sostenuta dal ribotipo 027,
Esposizione ad antibiotici (in particolareclindamicina, fluorochinoloni, amoxicillina,
cefalosporine) e chemioterapici
Utilizzo di antiacidi, inibitori di pompa,
Comorbidità (quali malattia renale cronica, diabete, neoplasie, diverticolosi intestinale,
malattia infiammatoria intestinale),
Chirurgia del tratto gastro-intestinale
Nutrizione enterale
Johnson S. J Infect. 2009 Jun;58(6):403-10. Garey KW, J Hosp Infect. 2008 Dec;70(4):298-304. Leffler DA, N Engl J Med. 2015 Apr
16;372(16):1539-48). Wilcox M,. Lancet 357(9251), 158–159 (2001); Debast SB et al. Clin Microbiol Infect. 2014;20(suppl
2):S1‒S26 Neemann K, Freifeld A. Clostridium difficile-associated diarrhea in the oncology patient. J Oncol Pract. 2017;13(1):25-30;
McFarland. Curr Opin Gastroenterol 2009;25:24–3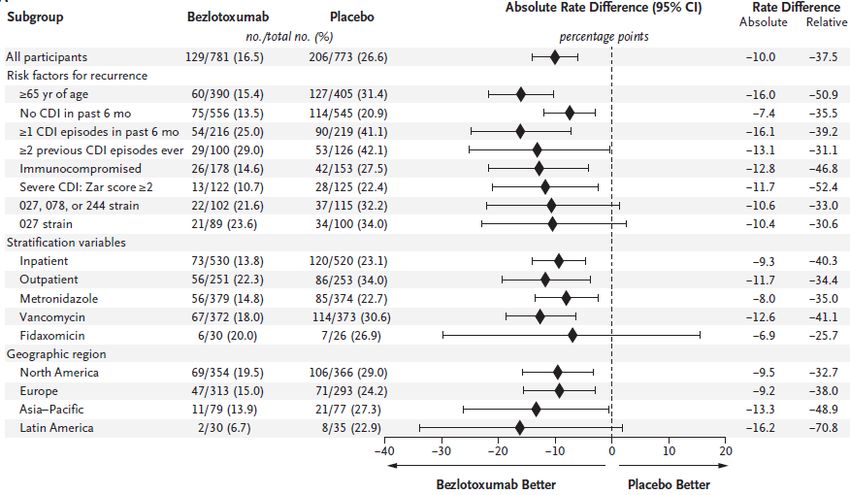
Risk Estimation for Recurrent CDI Based on Clinical Factors
D’Agostino Sr RB, et al. Clin InfectDis 2014;58:1386–93
• A simple/practical scoring rule (logistic regression model) for recurrent CDI
using data from the phase 3 clinical trials on fidaxomycin was developed
• 77 baseline CDI factors were classified:
• Demographics, comorbidity, medications, vital signs, lab tests, severity, symptoms
• The final model was derived from 922 participants
• In the first trial, fidaxo Vs. vanco recurrences were, respectively:
• 15.4% Vs. 25.3% Difference = 9.9%, P = .005
• In the second trial, fidaxo Vs. vanco recurrences were, respectively:
• 12.7% VS. 26.9% Difference = 14.2, P < .001
• The final model included 4 independent risk factors
• Age (
Clostridium difficile Toxins
• Most C. difficile strains two toxins: TcdA and TcdB
• A: permeability and fluid secretion
• B: cytotoxicity colonic inflammation
• Some C. difficile strains produce a binary toxin:
• C. difficile transferase (CDT)
• Closely related to the C. perfringens binary toxin
• 50-60% higher fatality rates than CDT-deficient strains
• CDT enhanced C. difficile virulence
• By suppressing protective colonic eosinophilia
Eckert C et al New microbes and new infections 2015;3: 12-17.
Chowdhury PR et al. BMC microbiology 2016; 16:41.
Cowardin CA et al. Nature Microbiology 2016;1: 16108.
Bacci S. Emerging Infectious Diseases 2011; 17: 976-982.Analisi Integrata degli Studi di Fase 3
MODIFY I e MODIFY II
Wilcox MH et al NEJM 2017; 376: 305-17MODIFY I e MODIFY II: Disegno dei Trials Clinici di fase III
Wilcox MH et al NEJM 2017; 376: 305-17
I trials clinici di fase 3
MODIFY I e MODIFY II sono
studi randomizzati, placebo-
controllati in doppio cieco.
Coinvolti 322 Centri in 30
Stati
Primary endpoint:
Percentuale di pazienti con
recidiva di CDI (definita
come nuovo episodio di
infezione da C. diff. dopo la
cura clinica iniziale
dell’episodio basale)
durante 12 settimane di
follow-up.
Secondary endpoint:
Global Cure: initial clinical
cure dell’episodio basale e
nessuna recidiva durante le
12 sett. di follow-up
12MODIFY1 e MODIFY2
Wilcox MH et al NEJM 2017; 376: 305-17
13MODIFY1 e MODIFY2
Wilcox MH et al NEJM 2017; 376: 305-17
77% dei pazienti: >1 fattore di rischio per recidiva di CDI
14ZAR Score
Wilcox MH et al 2017; 376: 305-317
Scala di punteggio: (1-8)
1. Età >60 anni 1 punto
2. Temperatura corporea >38,3 C° 1 punto
3. Livello di albumina 15.000 / mm3 1 punto
5. Evidenza endoscopica di colite pseudomembranosa 2 punti
6. Trattamento in reparto di terapia intensiva 2 punti
Infezione grave è stata definita come uno Zar score ≥2Endpoint primario: Recidiva di CDI
Endpoint primario; mITT, MODIFY l and MODIFY ll; percentuale di pazienti con recidiva di CDI
durante 12 sett. di follow-up
* pRecidiva di CDI per Sottogruppi
Durante 12 sett. di follow-up; MODIFY I + II; mITT
*
Wilcox M.H. et al. N Engl J Med 2017;376:305-17 and supplementary appendixClinical AEs Comparabili al Placebo
Wilcox NEJM 2017
* The adverse events reported on the day of or day after infusion that might have been a sign of an acute hypersensitivity reaction were
nausea, vomiting, chills, fatigue, feeling hot,
infusion-site conditions, pyrexia, arthralgia, myalgia, dizziness, headache, dyspnea, nasal congestion, pruritus, rash, urticaria, flushing, hot
flush, hypertension, and hypotension.
† Causality was assessed by the investigator, who was unaware of the study-group assignments.
‡ A list of serious drug-related events is provided in Table S12 in the Supplementary Appendix.
§ This category includes events with an incidence of at least 4% in at least one study group reported during the first 4 weeks after infusion.
¶ C. difficile infection (the primary efficacy end point) was to be reported as an adverse event only if it was serious.Bezlotoxumab
Somministrazione
durante
Unico e nuovo Meccanismo di Azione il ciclo di terapia antibatterica per CD
Singola infusione endovenosa di 10 mg/kg
Anticorpo monoclonale
(IgG1/kappa) di derivazione
completamente umana
Tecnologia di DNA ricombinante che Administration of Bezlotoxumab
neutralizza la tossina B at any time
Immunità passiva anti-B during the treatment
No attività antimicrobica diretta
Somministrato insieme alla terapia
Prevenzione delle recidive Initiation End
CDI CDI
antibiotic antibiotic
therapy therapy
FDA Briefing Document Bezlotoxumab Injection Meeting of the
Antimicrobial Drugs Advisory Committee (AMDAC) June 9, 2016). Leav
BA, et al. Vaccine 28 (2010) 965–969; RCP Zinplava, RCP ZinplavaVimalanand S. Prabhu et al. Clinical Infectious Diseases 2017
20Bezlotoxumab & Hospital Readmission for CDI Riduzione dei ricoveri ospedalieri in un'analisi post hoc su 1.050 pazienti ricoverati Riduzione del -53% il rischio di ri-ospedalizzazione a 30 giorni (5,1% vs 11,2%) Vimalanand S. Prabhu et al. Clinical Infectious Diseases 2017
Bezlotoxumab & Hospital Readmission for CDI Vimalanand S. Prabhu et al. Clinical Infectious Diseases 2017
• Indicazioni terapeutiche: ZINPLAVA è indicato per la prevenzione della recidiva
dell’infezione da Clostridium difficile (CDI) negli adulti ad alto rischio di recidiva di CDI.
• La rimborsabilità è limitata ai pazienti con diagnosi microbiologica di recidiva di CDI/CDAD
(NAAT o GDH positivo e tossina A/B positiva) già in trattamento con terapia antibiotica
specifica, in presenza di almeno 1 tra le seguenti condizioni:
• Soggetti di età >65 anni
• Forma severa di CDI (Zar-score ≥2)
• Soggetti immunocompromessi
• La prescrivibilità è riservata allo specialista infettivologo o, in sua assenza, ad altro
specialista con competenza infettivologica ad hoc identificato dal Comitato Infezioni
Ospedaliere (CIO) istituito per legge presso tutti i presidi ospedalieri (Circolare Ministero
della Sanità n. 52/1985).Posters…
25Golan Y. et al Poster 2017 ID_WEEK
Bezlotoxumab in Haematologic Malignancies
Post-hoc analysis of the Phase 3 MODIFY I/II trials to determine if bezlotoxumab
affected the rCDI rate in MODIFY I/II participants with a haematologic malignancy
107 participants included:
– 53 in the bezlo (BEZ) group
– 54 in the placebo (PBO) group.
Majority = inpatients at
randomization
Almost all ≥1 prespecified risk
factor for rCDI
A higher proportion of
participants in the PBO group
experienced ≥1 CDI episodes in
the previous 6 months
#P0358 - Cornely OA, et al. Impact of bezlotoxumab in recurrent Clostridium difficile infection in MODIFY I/II participants with haematologic malignancyPatients with haematologic malignancies with ICC, rCDI and SCC
The proportion of participants treated with bezlotoxumab (BEZ) achieving
initial clinical cure (ICC) was higher than in the placebo (PBO) group.
• The incidence of rCDI was
lower in BEZ participants
compared with PBO
• A greater proportion of
participants achieved
sustained clinical cure (SCC)
in the BEZ group than in the
PBO group
• Among participants who
experienced rCDI, no BEZ-
treated participants had
severe CDI (Zar score ≥2)
compared with 33.3% of
those treated with PBO
#P0358 - Cornely OA, et al. Impact of bezlotoxumab in recurrent Clostridium difficile infection in MODIFY I/II participants with haematologic malignancy.Hospitalization and Mortality in Patients with
Haematologic Malignancies
• A lower proportion of
BEZ-treated participants had a
CDI-associated re-hospitalization
compared with PBO (4.3% vs 11.6%)
• During the 12-week follow-up
period, the mortality rate was
9.3% in participants receiving
BEZ and 14.5% in participants
receiving PBO
Bezlotoxumab reduced the rate of rCDI compared with placebo in
participants with haematologic malignancy.
#P0358 - Cornely OA, et al. Impact of bezlotoxumab in recurrent Clostridium difficile infection in MODIFY I/II participants with haematologic malignancyBezlotoxumab in Patients with Solid Tumours
Post-hoc analysis of the Phase 3 MODIFY I/II trials to determine if
bezlotoxumab affected the rCDI rate in MODIFY I/II participants with a
solid tumour as a comorbid condition.
290 participants were included in
the solid tumour subgroup:
– 143 in the bezlo (BEZ) group
(48.3% female; median age 69
years)
– 147 in the placebo (PBO) group
(53.7% female; median age 68 y)
A higher proportion of BEZ-treated
participants had ≥1 prespecified
risk factor for rCDI compared with
PBO (86.0% vs 77.6%), including a
higher incidence of participants
who had ≥1 CDI episode in the past
6 months (32.2% vs 21.8%)
#P0359 - Mullane K, et al. Reduction of recurrent Clostridium difficile infection in solid tumour participants treated with bezlotoxumabPatients with Solid Tumours with ICC, rCDI and SCC
• Initial clinical cure (ICC) rates
were similar between both
treatment groups.
• Although a lower proportion of
BEZ-treated participants
experienced an rCDI than PBO-
treated participants, the
difference was not significant.
• Among participants who
experienced rCDI,
a lower proportion of severe
rCDI (Zar score ≥2) was reported
in the BEZ group compared with
the PBO group (4.5% vs 12.9%).
• A similar proportion of
participants achieved sustained
clinical cure (SCC) in BEZ
and PBO groups.
#P0359 - Mullane K, et al. Reduction of recurrent Clostridium difficile infection in solid tumour participants treated with bezlotoxumabHospitalization & Mortality in Patients with Solid Tumours
• The rate of 30-day CDI-associated
re-hospitalization was lower in the
BEZ group than in the PBO group
(5.5% vs 10.2%).
• Mortality rates during 12-week
follow-up were lower in the
BEZ group (10.5% vs 15.6% in
the BEZ and PBO groups,
respectively).
Bezlotoxumab led to a proportionally lower rCDI rate in solid
tumour participants compared with placebo.
#P0359 - Mullane K, et al. Reduction of recurrent Clostridium difficile infection in solid tumour participants treated with bezlotoxumab. Prima molecola anti-tossina B approvata nella
prevenzione delle recidive di CDI in pazienti ad alto
rischio, in add-on agli antibiotici utilizzati per il
trattamento del CDI
Riduzione del 40% delle recidive di CDI (16.5% vs
26.6%) e della riammissione ospedaliera
Efficacia dimostrata in sottogruppi di pazienti a rischio
(insufficienza renale, fattori di rischio combinati,
paziente ematologico, neoplasia solida)
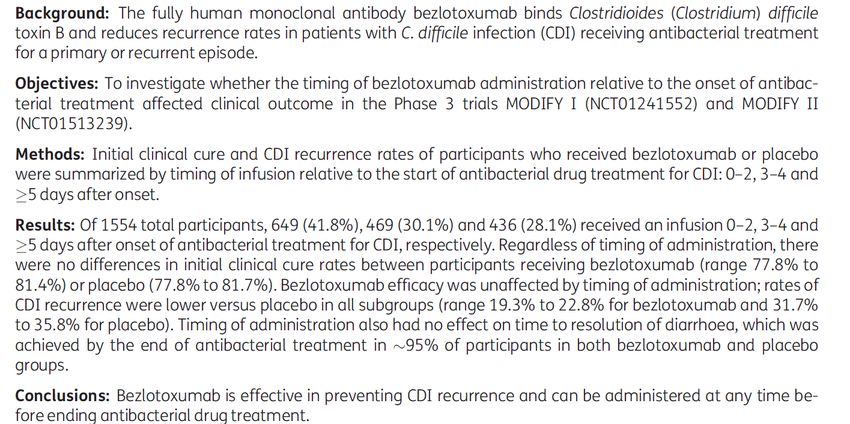
Il timing di infusione non influenza l’efficacia
AINF-1280702-0000-ZIN-W-02-2020Puoi anche leggere