UPDATE Malattie Infettive - AMITI 2017 - Amiti Med
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

UPDATE Malattie Infettive
AMITI 2017
PD Dr. med. Christian Garzoni
christian.garzoni@gmail.com
Servizio medicina interna e malattie infettive Clinica universitaria di malattie infettive
Clinica Luganese – Moncucco Inselspital - Ospedale universitario
Lugano Berna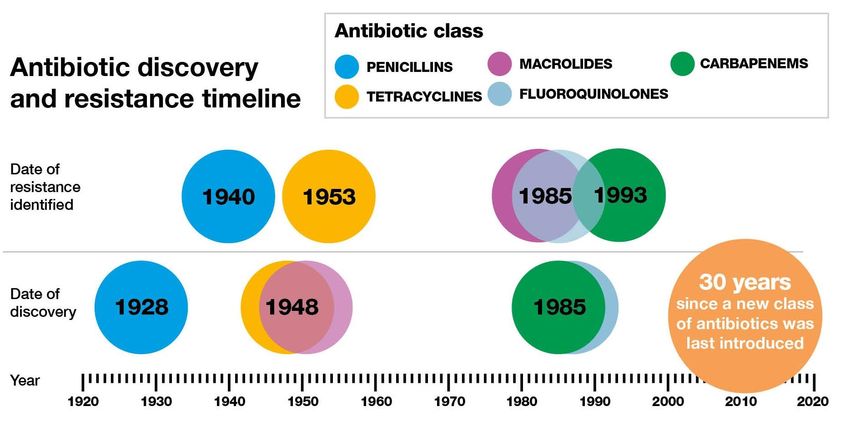
Malattie infettive – novità 2016-2017
Resistanza antibiotica:
– Dove siamo-update epidemiologia
– Programma Star – OFSM
– Terapie di germi multiresistenti: novità 2017
– Viaggi e germi multiresistenti
– Nuovi antibiotici? Update
Nuove linee guida terapia antibiotica per il TI 2018-2019
Polmonite - 2017
– Diagnostica
– Durata di terapia
Zika virus - update
HIV:
– Speranza di vita
– quando iniziare a trattare: subito!
– TERAPIA 2017 1x pillola
HCV:
– Novità casse malati: tutti i pazienti possono essere trattati
– la rivoluzione terapeutica va avanti
Nuovo patogeno: Candida Auris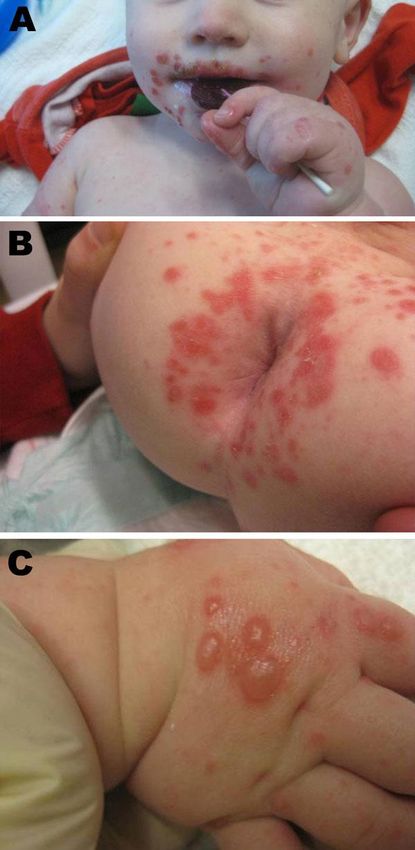
Malattie infettive – novità 2016-2017
Resistanza antibiotica:
– Dove siamo-update epidemiologia
– Programma Star – OFSM
– Terapie di germi multiresistenti: novità 2017
– Viaggi e germi multiresistenti
– Nuovi antibiotici? Update
Nuove linee guida terapia antibiotica per il TI 2018-2019
Polmonite - 2017
– Diagnostica
– Durata di terapia
Zika virus - update
HIV:
– Speranza di vita
– quando iniziare a trattare: subito!
– TERAPIA 2017 1x pillola
HCV:
– Novità casse malati: tutti i pazienti possono essere trattati
– la rivoluzione terapeutica va avanti
Nuovo patogeno: Candida Auris
ESBL - E. coli in Europa – in meno di 15 anni…
2002 2011 2015
www.ecdc.europa.eu
Europe 2009-2013 Source eCDC
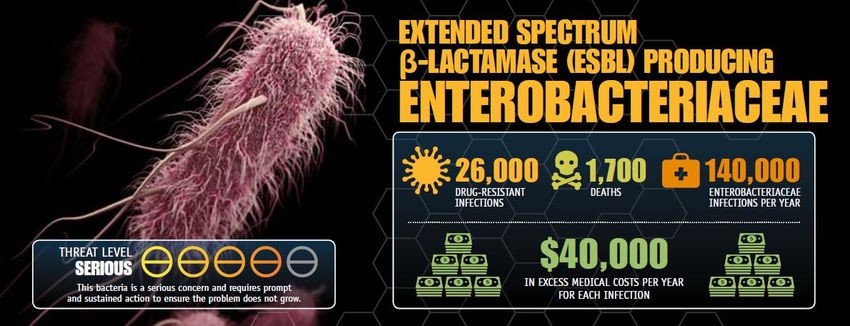
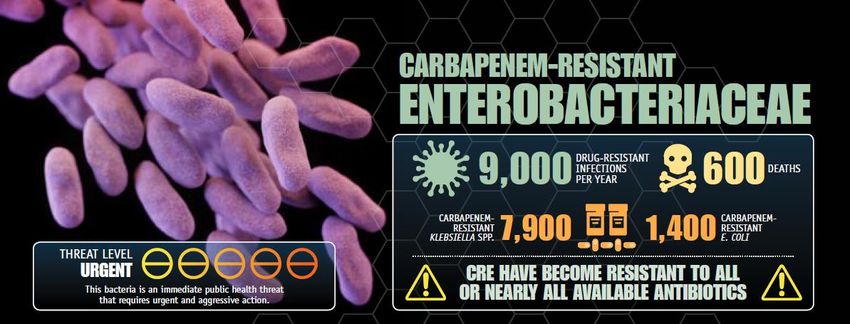
USA - 2013 CDC ANTIBIOTIC RESISTANCE THREATS in the United States, 2013
CDC ANTIBIOTIC RESISTANCE THREATS in the United States, 2013
2050…Studio UK
2050:
- Drug resistant infections will kill an extra 10 million people a year worldwide
- They are currently implicated in 700,000 death/y.
- Costs would spiral to $100’000’000’000 (=100 triliardi) = 100tn$!
Mr O’Neill told the BBC: “To put that in context, the annual GDP [gross domestic product]
of the UK is about $3tn, so this would be the equivalent of around 35 years without the
UK contribution to the global economy.”
Source Jim O’Neill
RESISTENZA ANTIBIOTICA PROBLEMA MAGGIORE CI CONCERNE TUTTI
Jährlich erkranken in Schweizer Spitälern rund 70 000 Patientinnen und Patienten an einer healthcare-assoziierten Infektion (HAI) und rund 2000 sterben daran.
http://www.anresis.ch/files/pdf/BAG_Swiss_Antibiotic_Resistance_Report_2016_WEB.pdf
Klebsiella pneumoniae
S.aureus e MRSACDT 10.11.2017
Settimana
Ufficio del Medico Cantonale
www.ti.ch/antibioticiBatteri multi-resistenti
Pz ambulanti- UPDATE
• ESBL
• Produttori carbapenemasi
• Misure di igieneSituazione in Svizzera – trends 2017
MRSA
ESBL
VRE
CRE
MRSA = Methicllin Resistant Stphylococcus Aureus
ESBL = Extended Spectrum Beta-Lactamase
VRE = Vancomycin Resistant Enterococci
CRE = Carbapenem Resistant Enterobacteriaceae www.anresis.chBatteri produttori di ESBL
Rilevanza clinica
• Producono enzima che distruggono tutti betalattamine
(Extended spectrum bela-lactamases)
• Epidemia SEMPRE PIÙ EXTRAOSPEDALIERA
– Agricoltura!
• Batteri NON sono più aggressivi
• Sono difficili da curare!
-> mortalità più alta perché attualmente tt empirico
non li copre sempre!
• Essere colonizzati NON significa dover trattare!Batteri produttori di ESBL
• Echerichia Coli • Salmonella
• Klebsiella pneumoniae • Morganella morganii
• Proteus mirabilis • Klebsiella oxytoca
• Enterobacter aerogenes • Citrobacter koseri
• Enterobacter cloacae • Pseudomonas aeruginosa
• Citrobacter freundii
• Serratia marcescens
Slide: dr. Carlo Balmelli EONOSOESBL - terapie SI*=SOLO SE LAB =S
Nome comm Cistite Pielonefrite Batteriemia Commento
TMT/SMX Bactrim® Si* SI*, 14d SI*, 14d
Ciprofloxacin Si* SI*, 7d SI*, 14d
Fosfomycin Monuril® Si* NO NO
Nitrofurantoin Furadantin® Si* NO NO
Amoxi/Cl Augmentin® NO NO NO NO per definizione
Cefuroxim Zinat® NO NO NO NO per definizione
Ceftriazon Rocefin® NO NO NO NO per definizione
Cefepime Cefepime NO NO NO NO per definizione
Cetazidin Fortam®
Pip/tazo Tazobac® NO NO NO NO per definizione
Aminoglycoside Ev. Ev. Ev. TOSSICITÀ
IMI/MERO Tienam, (SI) SI SI i.v. 3-4x/24h Test
Meronem
ERTA Invanz SI SI SI i.v. 1x/24h. Test!Produttori di carbapenemasi (CRE = Carbapenem Resistant Enterobacteriaceae) una catastrofe annunciata purtroppo
Cultura urinaria di un pz in studio…
Carbapenemasi
• Resistenti a tutti i seguenti:
– Penicilline
– Cefalosporine
– Carbapenemi: imipenem , meropenem, invanz
• Acquisizione di resistenze multiple->PANresistenti!
• Serbatoio: intestino
• Rapida diffusione nella “community”/nosocomiale
• Rapida diffusione «mondiale» (globalizzazione!)
• diffusione attraverso cibo e acqua (non solo in paesi con
problemi igienici!)
• Epidemie ospedaliere fino a endemicità!Carbapenemase, sono varie!
Batteri produttori carbapenemasi 2013 2015
Batteri produttori di carbapenemasi
TI e in CH ?
Obbligo di
dichiarazione
(nuovo dal 1.1.2017)
www.anresis.chPrevezione infezione in caso di germe multiresistente in studio medico? http://www4.ti.ch/dss/dsp/umc/cosa-facciamo/malattie-infettive/malattie-batteriche/germi-multiresistenti/
Batteri in viaggio
un problema?
- 170 viaggiatori nel SE asiatico
- striscio rettale prima e dopo alla ricerca di enterobatt. ESBL
- 69.4% tornano colonizzati
34 Courtesy C. Truniger, sett. 2017Batteri in viaggio
un problema?
- persistenza dei ESBL:
- in media 30 giorni
Pensarci! - 11.3% restano colonizzati
per 12 mesi
Se viaggio recente, aumento di
- 7.7% trasmissione a membro
rischio di colonizzazione a germi
dell’economia domestica
multiresistenti!
36 Modified from C. Truniger, sett. 2017E nuovi antibiotici?
E nuovi antibiotici?
…Malattie infettive – novità 2016-2017
Resistanza antibiotica:
– Dove siamo-update epidemiologia
– Programma Star – OFSM
– Terapie di germi multiresistenti: novità 2017
– Viaggi e germi multiresistenti
– Nuovi antibiotici? Update
Nuove linee guida terapia antibiotica per il TI 2018-2019
Polmonite - 2017
– Diagnostica
– Durata di terapia
Zika virus - update
HIV:
– Speranza di vita
– quando iniziare a trattare: subito!
– TERAPIA 2017 1x pillola
HCV:
– Novità casse malati: tutti i pazienti possono essere trattati
– la rivoluzione terapeutica va avanti
Nuovo patogeno: Candida AurisBase di discussione
TI-Guidelines gruppo malattie infettive
2018-2019
Disponibile online: www.ti.ch/antibiotici: Medico CantonaleMalattie infettive – novità 2016-2017
Resistanza antibiotica:
– Dove siamo-update epidemiologia
– Programma Star – OFSM
– Terapie di germi multiresistenti: novità 2017
– Viaggi e germi multiresistenti
– Nuovi antibiotici? Update
Nuove linee guida terapia antibiotica per il TI 2018-2019
Polmonite - 2017
– Diagnostica
– Durata di terapia
Zika virus - update
HIV:
– Speranza di vita
– quando iniziare a trattare: subito!
– TERAPIA 2017 1x pillola
HCV:
– Novità casse malati: tutti i pazienti possono essere trattati
– la rivoluzione terapeutica va avanti
Nuovo patogeno: Candida AurisGuidelines TI 2018-2019 Guidelines TI 2015-2016
Polmonite: durata? CAP 5g (-10g) (3 giorni senza febbre) Linee Direttive Cantonali 2015-16
JAMA Intern Med 2016 Jul 25.
• IMPORTANCE The optimal duration of antibiotic treatment for community-acquired pneumonia
(CAP) has not been well established.
• OBJECTIVE To validate Infectious Diseases Society of America/American Thoracic Society
guidelines for duration of antibiotic treatment in hospitalized patients with CAP.
• DESIGN, SETTING, AND PARTICIPANTS multicenter, noninferiority randomized clinical trial
• INTERVENTIONS Patients were randomized at day 5 to an intervention or control group.
• Those in the intervention group were treated with antibiotics for a minimum of 5 days, and the
antibiotic treatment was stopped at this point if their body temperature was 37.8°C or less for
48 hours and they had no more than 1 CAP-associated sign of clinical instability:
– as systolic blood pressure < 90mmHg,
– heart rate >100/min,
– respiratory rate >24 /min,
– arterial oxygen saturation < 90%, or PaO25d
Polmonite (non legionella): buon decorso = 5 giorni!
JAMA Intern Med 2016 Jul 25.CID 2016: 62 817
Background. The frequent lack of a microbiological diagnosis in community-acquired pneumonia
(CAP) impairs pathogendirected antimicrobial therapy. This study assessed the use of
comprehensive multibacterial, multiviral molecular testing in adults hospitalized with CAP.
Methods. Clinical and laboratory data were collected for 323 adults with radiologically-confirmed
CAP admitted to 2 UK tertiary care hospitals. Sputum (96%) or endotracheal aspirate (4%)
specimens were cultured as per routine practice and also tested with fast multiplex real-time
polymerase-chain reaction (PCR) assays for 26 respiratory bacteria and viruses. …
Results. Comprehensive molecular testing of single lower respiratory tract (LRT) specimens
achieved pathogen detection in 87%of CAP patients compared with 39% with culture-based
methods. Haemophilus influenzae and Streptococcus pneumoniae were themain agents
detected, along with a wide variety of typical and atypical pathogens. Viruses were present in
30% of cases; 82% of these were codetections with bacteria. ..Molecular testing had the
potential to enable de-escalation in number and/or spectrum of antimicrobials in 77% of
patients.
Conclusions. Comprehensive molecular testing significantly improves pathogen detection in CAP,
particularly in antimicrobialexposed patients, and requires only a single LRT specimen. It also has
the potential to enable early de-escalation from broadspectrum empirical antimicrobials to
pathogen-directed therapy.
CID 2016: 62 817CID 2016: 62 817
CID 2016: 62 817
CID 2016: 62 817
Striscio gola e PCR multiplex – anche
da voi!
• Problema: costo 400 frs!
• Indicazione chiara: casi selezionati
(immunosuppressi)Malattie infettive – novità 2016-2017
Resistanza antibiotica:
– Dove siamo-update epidemiologia
– Programma Star – OFSM
– Terapie di germi multiresistenti: novità 2017
– Viaggi e germi multiresistenti
– Nuovi antibiotici? Update
Nuove linee guida terapia antibiotica per il TI 2018-2019
Polmonite - 2017
– Diagnostica
– Durata di terapia
Zika virus - update
HIV:
– Speranza di vita
– quando iniziare a trattare: subito!
– TERAPIA 2017 1x pillola
HCV:
– Novità casse malati: tutti i pazienti possono essere trattati
– la rivoluzione terapeutica va avanti
Nuovo patogeno: Candida AurisDépartement fédéral de l'intérieur DFI
Office fédéral de la santé publique OFSP
Division Maladies transmissibles
Propagation Zika
Virus ZIKA
Virus Zika / Connaissances actuelles et mesures
Michael Bel
9.2.2016Localizzazione 11.2017
Dati: CDC 11.11.2017Microcefalia
95:100’000
Microcefalie is incidence is estimated to be between :
- 5.8 per 100 000 livebirths in the USA
- 18.7 per 100 000 livebirths, stillbirths, and medical abortions
in Europe.
Lancet 15 March 2016Guillan Barré e Zika
• Mediamente 6 giorno dopo la malattia virale
• Decorso più benigno che GBS abituale
Lancet 29 Feb 2016Trasmissione sessuale
Update 11.11.2017 Recommandations Une protection optimale contre les piqûres de moustiques est recommandée à tous les voyageurs. En attendant de disposer de données plus précises sur le risque de malformations fœtales, il est déconseillé aux femmes enceintes, à tout moment de la grossesse, de se rendre dans les régions avec une transmission active du Zika. En raison d'un risque de transmission sexuelle du Zika, l'emploi d'un préservatif est conseillé après un séjour dans une zone de transmission active du virus Zika (durant au moins 2 mois pour les femmes, 6 mois pour les hommes ou durant toute la grossesse si la partenaire est enceinte). Les femmes qui souhaitent avoir un enfant devraient attendre 2 mois après leur retour d'une région à transmission active avant de planifier une grossesse.
Malattie infettive – novità 2016-2017
Resistanza antibiotica:
– Dove siamo-update epidemiologia
– Programma Star – OFSM
– Terapie di germi multiresistenti: novità 2017
– Viaggi e germi multiresistenti
– Nuovi antibiotici? Update
Nuove linee guida terapia antibiotica per il TI 2018-2019
Polmonite - 2017
– Diagnostica
– Durata di terapia
Zika virus - update
HIV:
– Speranza di vita
– quando iniziare a trattare: subito!
– TERAPIA 2017 1x pillola
HCV:
– Novità casse malati: tutti i pazienti possono essere trattati
– la rivoluzione terapeutica va avanti
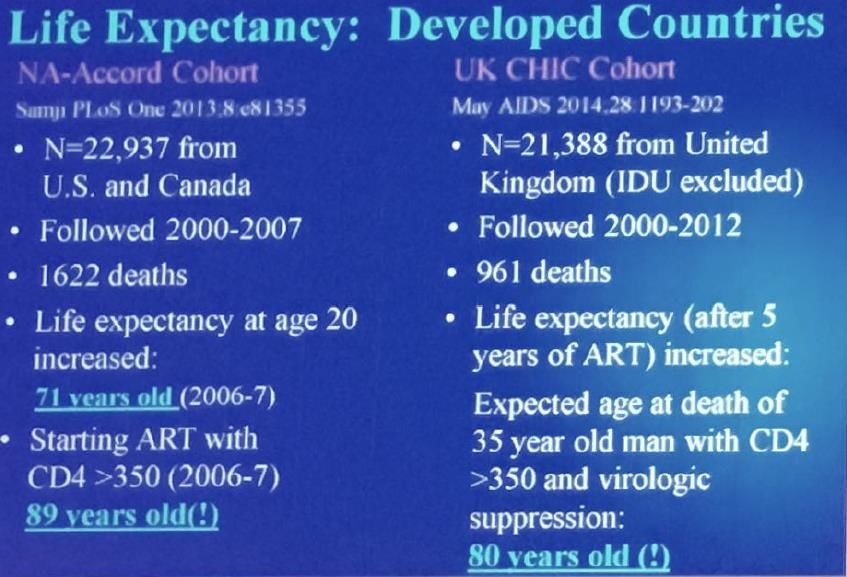
Nuovo patogeno: Candida AurisHIV: sopravvivenza
EACS 2017HIV-sopravvivenza
EACS 2017Quando iniziare?
START: Immediate vs Deferred Therapy for
Asymptomatic, ART-Naive Patients
Study closed by DSMB
• International, randomized trial, 35 countries following interim analysis
Immediate ART
ART initiated immediately
following randomization
HIV-positive, ART-naive n = 2326
adults with CD4+ cell
count > 500 cells/mm3 Deferred ART
N = 4685 Deferred until CD4+ cell count ≤ 350 cells/mm3,
AIDS, or event requiring ART
n = 2359
• Composite primary endpoint: any serious AIDS-related (AIDS-related death or AIDS-defining
event) or non-AIDS–related event (non-AIDS–related death, CVD, end-stage renal disease,
decompensated liver disease, non-AIDS–defining cancer)
• Mean follow-up: 3 yrs; median baseline CD4+ cell count: 651 cells/mm3; median baseline
HIV-1 RNA: 12,759 copies/mL
• Median CD4+ cell count at initiation of ART for deferred group: 408 cells/mm3
INSIGHT START Study Group, Lundgren JD et al., N Engl J Med. 2015
Courtesy Prof. Battegay, BaselART, HIV RNA and CD4 Course
INSIGHT START Study Group, Lundgren JD et al., N Engl J Med. 2015START: 57% Reduced Risk of Serious
Events or Death with Immediate ART
4.1% vs 1.8% in deferred vs immediate arms experienced serious AIDS or
non-AIDS–related event or death (HR: 0.43; 95% CI: 0.30-0.62; P < .001)
10
Cumulative Percent With Event
8
Deferred ART
6
4
2 Immediate ART
0
0 6 12 18 24 30 36 42 48 54 60
Mo
INSIGHT START Study Group, Lundgren JD et al., N Engl J Med. 2015HAART Tri-Terapia / 1-2 pillola
1 tab
1 + 1 tab
1 tab
1 + 1 tab
1 tab
1 + 1 tab
1 + 2 tabHIV / Epidemiologia TI-CH
HIV / Epidemiologia TI-CH
HIV / Epidemiologia TI-CH
Malattie infettive – novità 2016-2017
Resistanza antibiotica:
– Dove siamo-update epidemiologia
– Programma Star – OFSM
– Terapie di germi multiresistenti: novità 2017
– Viaggi e germi multiresistenti
– Nuovi antibiotici? Update
Nuove linee guida terapia antibiotica per il TI 2018-2019
Polmonite - 2017
– Diagnostica
– Durata di terapia
Zika virus - update
HIV:
– Speranza di vita
– quando iniziare a trattare: subito!
– TERAPIA 2017 1x pillola
HCV:
– Novità casse malati: tutti i pazienti possono essere trattati
– la rivoluzione terapeutica va avanti
Nuovo patogeno: Candida AurisHCV - terapia
Swiss Guidelines (SASL 10.2017)
Courtesy Dr L. Magenta, EpatocentoIn CH >50% dei casi non sono ancora stati ancora
diagnosticati (e troppo pochi vengono trattatti)
Health Consumer Powerhouse AB, 2012. ISBN 978-91-980687-0-2
Courtesy Dr L. Magenta, EpatocentoMalattie infettive – novità 2016-2017
Resistanza antibiotica:
– Dove siamo-update epidemiologia
– Programma Star – OFSM
– Terapie di germi multiresistenti: novità 2017
– Viaggi e germi multiresistenti
– Nuovi antibiotici? Update
Nuove linee guida terapia antibiotica per il TI 2018-2019
Polmonite - 2017
– Diagnostica
– Durata di terapia
Zika virus - update
HIV:
– Speranza di vita
– quando iniziare a trattare: subito!
– TERAPIA 2017 1x pillola
HCV:
– Novità casse malati: tutti i pazienti possono essere trattati
– la rivoluzione terapeutica va avanti
Nuovo patogeno: Candida AurisCandida auris
Candida auris • Since 2016: emerging fungus. • Multidrug-resistant Candida species • Often resistant to agents from other antifungal classes, particularly azoles. • Recommanded initial therapy: echinocandin. • C. auris causes severe illness in hospitalized patients in several countries: candidemia with high mortality • Long colonization! • C. auris can persist on surfaces in healthcare environments.
Malattie infettive – novità 2016-2017
Resistanza antibiotica:
– Dove siamo-update epidemiologia
– Programma Star – OFSM
– Terapie di germi multiresistenti: novità 2017
– Viaggi e germi multiresistenti
– Nuovi antibiotici? Update
Nuove linee guida terapia antibiotica per il TI 2018-2019
Polmonite - 2017
– Diagnostica
– Durata di terapia
Zika virus - update
HIV:
– Speranza di vita
– quando iniziare a trattare: subito!
– TERAPIA 2017 1x pillola
HCV:
– Novità casse malati: tutti i pazienti possono essere trattati
– la rivoluzione terapeutica va avanti
Nuovo patogeno: Candida AurisGrazie per l’attenzione
• Population-Based Estimates of Appropriate and Inappropriate Antibiotic Prescribing
• Thomas L. Schwenk, MD reviewing Fleming-Dutra KE et al. JAMA 2016 May 3. Tamma PD and Cosgrove SE. JAMA
2016 May 3.
• Thomas L. Schwenk, MD
• The U.S. annual antibiotic prescribing rate in 2010 was about 500 prescriptions per 1000 people; one third of
prescriptions were judged to be inappropriate.
• Thomas L. Schwenk, MD
• Research about inappropriate antibiotic prescribing usually focuses on specific conditions and age groups.
However, these researchers used several national ambulatory care databases to provide overall population-based
estimates that could guide government and professional mandates designed to reduce inappropriate antibiotic
prescribing.
• Researchers assessed appropriateness of antibiotic use in about 184,000 ambulatory visits (not including urgent
care centers, “minute” clinics, federal facilities, or long-term care facilities) in 2010 and 2011 using accepted
clinical practice guidelines. If guidelines were not available (e.g., for sinusitis), the lowest regional level of
antibiotic use was used as a surrogate for appropriateness (almost certainly still an overestimate). For some
conditions (e.g., pneumonia), all antibiotic use was deemed to be appropriate.
• The overall annual rate of antibiotic use was 506 prescriptions per 1000 people, of which roughly two thirds of
prescriptions (353 prescriptions/1000 people) were deemed to be appropriate. The overall rate ranged from 423
to 553 prescriptions per 1000 people in the West and South, respectively. Most inappropriate antibiotic use was
for acute respiratory conditions (111 prescriptions/1000 people annually).
• Comment
• A 50% reduction in inappropriate antibiotic prescribing could be achieved mostly through eliminating
prescriptions for acute respiratory conditions. This drop would translate to an overall annual rate of about 400
prescriptions per 1000 people, still much higher (as the authors note) than the prescribing rate in Sweden (328
prescriptions/1000 people), a country with a very low rate of antibiotic resistance.• Treatment of Asymptomatic Bacteriuria Promotes Antibiotic Resistance
• Neil M. Ampel, MD reviewing Cai T et al. Clin Infect Dis 2015 Dec 1. Wagenlehner FME and Naber KG. Clin Infect Dis
2015 Dec 1.
• Neil M. Ampel, MD
• In an extension of a study of treatment for asymptomatic bacteriuria, recurrent bacteriuria and antibiotic
resistance were more common in women who received antibiotics.
• Neil M. Ampel, MD
• Antibiotic therapy for asymptomatic bacteriuria (AB; bacteria in urine without signs or symptoms of urinary tract
infection) is recommended only for pregnant women and men undergoing urologic procedures; nonetheless,
treatment of AB is common. A previous study demonstrated that women treated for AB had significantly higher
rates of recurrent bacteriuria after 12 months compared with those not receiving antibiotics (NEJM JW Gen Med
Nov 1 2012 and Clin Infect Dis 2012; 55:771). Now, in an extension of this study (mean follow-up, 39 months), the
same Italian investigators analyzed the results from 550 participants (257 untreated; 293 treated with antibiotics).
• Risk for recurrent bacteriuria was 4.4-fold higher in women who received antibiotics than in those who did not
(P=0.003). Moreover, risk for developing recurrent bacteriuria with Escherichia coli resistant to
amoxicillin/clavulanate (P=0.03), trimethoprim-sulfamethoxazole (P=0.01), and ciprofloxacin (P=0.03) was
significantly higher in those who received antibiotics.
• Comment
• This study demonstrates the pernicious effect of antibiotic overuse. Not only did antibiotics fail to prevent
recurrent bacteriuria, but they promoted resistance — even when their use occurred months or years before. As
editorialists point out, this and other studies indicate that once antibiotic resistance develops, it has a low
probability of reversal.• asymptomatic
• bacteriuria (AB), but the consequences of this procedure on antibiotic resistance are not fully known. The
• aim of this study was to evaluate the impact of AB treatment on antibiotic resistance among women with rUTIs.
• Methods. The study population consisted of 2 groups of women who had previously been enrolled in a
randomized
• clinical trial: group Awas not treated, and group B was treated. All women were scheduled for follow-up visits
every
• 6 months, or more frequently if symptoms arose. Microbiological evaluation was performed only in symptomatic
• women. All women were followed up for a mean of 38.8 months to analyze data from urine cultures and
antibiograms.
• Results. The previous study population consisted of 673 women, but 123 did not attend the entire follow-up
period.
• For the final analysis, 257 of the remaining 550 patients were assigned to group A, and 293 to group B. At the end
• of follow-up, the difference in recurrence rates was statistically significant (P < .001): 97 (37.7%) in group A versus
204
• (69.6%) in group B. Isolated Escherichia coli from group B showed higher resistance to amoxicillin–clavulanic acid
• (P = .03), trimethoprim-sulfamethoxazole (P = .01), and ciprofloxacin (P = .03) than that from group A.
• Conclusions. This study shows that AB treatment is associated with a higher occurrence of antibiotic-resistant
bacteria,
• indicating that AB treatment in women with rUTIs is potentially dangerous.• Third Generation Cephalosporin-Resistant Enterobacteriaceae Carriage in Germany
• Thomas Glück, MD reviewing Hamprecht A et al. J Antimicrob Chemother 2016 Jun 17.
• Thomas Glück, MD
• The prevalence of extended-spectrum beta-lactamase–producing pathogen colonization at hospital admission was almost 10%, with previous
colonization, antibiotic use, travel, long-term care facility residence, and acid-suppressive therapy as risk factors.
• Thomas Glück, MD
• Third-generation cephalosporin–resistant Enterobacteriaceae (3GCREB) have recently emerged in many countries. The gut is the reservoir for
infections with these organisms. Investigations into the prevalence of these multiresistant pathogens in Europe have been lacking in the past several
years. German researchers have now published results from a multicenter study performed at six German tertiary care hospitals in 2014 that shed
some light on this issue. The study involved 4376 patients admitted to general wards with various diagnoses who received stool or rectal swab
screening for 3GCREB within the first 3 days of their hospital stay.
• Of the 4376 patients, 416 were 3GCREB positive, an admission prevalence of 9.5%. Escherichia coli was the most common 3GCREB species,
accounting for 79.1%, followed by Klebsiella pneumoniae (8.5%), Enterobacter spp. (5.7%), and Citrobacter spp. (4.8%). Many (41%) of the 3GCREB
isolates were also resistant to fluoroquinolones, whereas carbapenem resistance was found in only 1.4% (overall admission prevalence, 0.1%).
Extended-spectrum ß-lactamase (ESBL) production was the predominant resistance mechanism, detected in 90.2% of the isolates (CTX-M-1, 67.3%;
CTX-M-9, 16.8%; SHV, 5.4%; and AmpC, 9.5%). In multivariate regression analysis, risk factors significantly associated with 3GCREB colonization
included prior infection with a multiresistant organism (odds ratio, 2.12), prior antimicrobial treatment (OR, 2.09), travel outside Europe (OR, 2.24),
previous colonization with an multidrug-resistant organism (OR, 2.12), stay in a long-term care facility (OR, 1.33), and medical treatment of
gastroesophageal reflux disease within the previous 6 months (OR, 1.22).
• Comment
• The prevalence of 3GCREB (mostly ESBL producers) among admitted patients is higher in this study than reported previously. The risk factors apply to
a large proportion of admitted patients, so high-risk patients cannot be easily identified. Therefore, vertical prevention strategies are unlikely to
reduce 3GCREB transmission (which likely occurs outside the hospital in most cases). Reinforcing horizontal prevention strategies, primarily hand
hygiene and antimicrobial stewardship programs, could be a more promising approach.Puoi anche leggere