Peroni Diego U.O. di Pediatria Università di Pisa - Infezioni respiratorie ricorrenti: Federazione Italiana Medici Pediatri
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
Infezioni respiratorie ricorrenti:
nuove evidenze e bandierine rosse per
la prevenzione nella pratica quotidiana
Peroni Diego IRR ..
U.O. di Pediatria Le bandierine rosse
Università di Pisa Immunomodulanti e IRR
IRR ma non solo ..
Le novità ..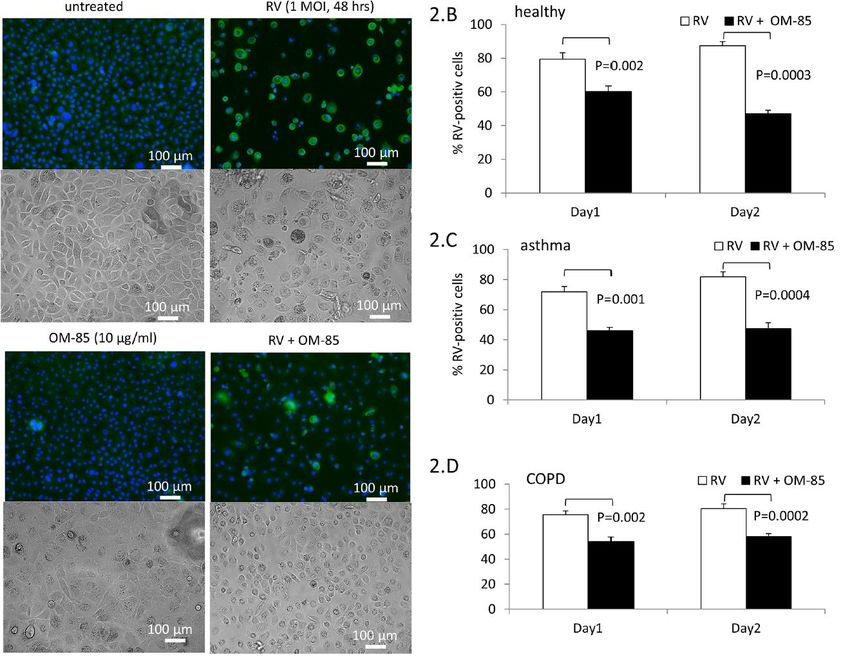
Immunomodulanti oggi…
Novità ?
IN LETTERATURA NON ESISTE
UNA DEFINIZIONE UNIVOCA DELLE IRR
- Alte e/o basse vie respiratorie?
- Forme febbrili e non?
- Il wheezing va considerato?
- Limiti di età?
- Forme virali e/o batteriche?
Clin Rev Allergy Immunol 2002. Ballow
Pediatr Infect Dis J 2004. Griffin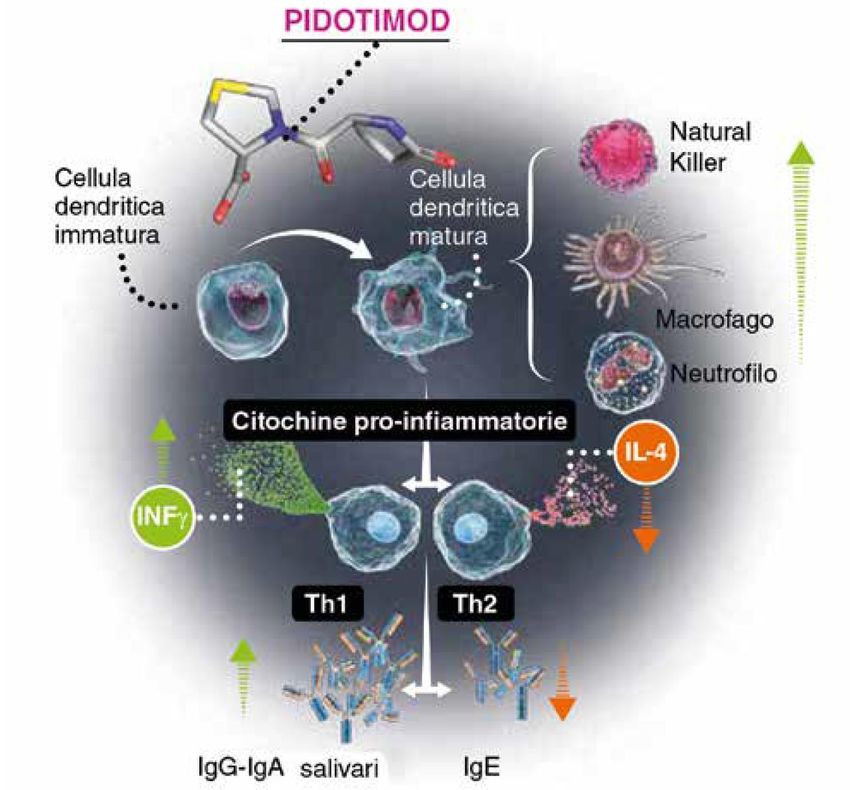
Le Infezioni Respiratorie Ricorrenti
IN LETTERATURA NON ESISTE
UNA DEFINIZIONE UNIVOCA DELLE IRR
Immunology Study Group of the Italian Pediatric Society
6 o più infezioni per anno
1 o più infezioni respiratorie al mese tra Settembre e Aprile
3 o più infezioni delle vie respiratorie inferiori per anno
Criterio Numerico diventa il parametro Ottimale
Pediatric Allergy Immunol 2007. De Martino
Chi è il bambino con infezioni respiratorie ricorrenti?
my child is
always sick
Criteri per definire il bambino affetto da Infezioni Respiratorie Ricorrenti (IRR) in età
pediatrica :
1-3 anni: 6 o più infezioni delle vie respiratorie superiori (o una o più al mese da
ottobre a marzo) in un anno e/o 2 infezioni delle vie respiratorie inferiori (polmonite
confermata da criteri clinici e/o radiologici) in un anno
3-6 anni: 5 o più infezioni delle vie respiratorie superiori (o una o più al mese da
ottobre a marzo) in un anno e/o 2 infezioni delle vie respiratorie inferiori (polmonite
…
confermata da criteri clinici e/o radiologici) in un anno
6 anni fino a 10 anni***: 3 o più infezioni delle vie respiratorie superiori (o una o più
al mese da ottobre a marzo) in un anno e/o 2 infezioni delle vie respiratorie inferiori
(polmonite confermata da criteri clinici e/o radiologici) in un anno
*** Limite di età oltre il quale la WHO definisce l’adolescente
proposta dal Prof. Maurizio de Martino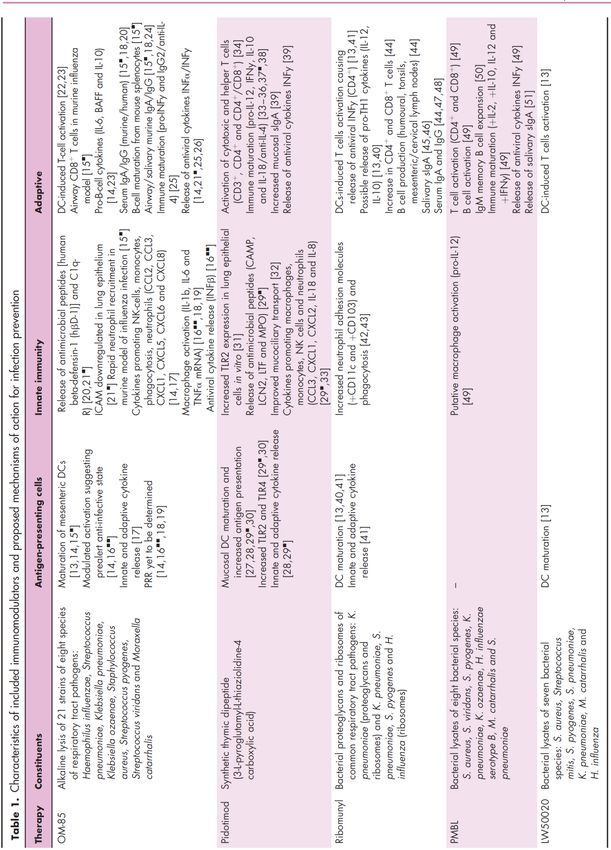
Costi sanitari
Se proviamo a considerare il punto di vista della famiglia che si
trova a dover affrontare un numero di 10-12 episodi infettivi
concentrati di solito nel periodo settembre/aprile alcune delle
nostre convinzioni sulla banalità del problema vacillano.
COSTI DIRETTI E INDIRETTI DELLE IRR
Durata media di ogni infezione respiratoria: 10,4 giorni
46,7 visite mediche/100 episodi
19,7 cicli di antibioticoterapia/100 episodi
2,2 ricoveri ogni 100 episodi
11,7 ore utilizzate per accudire il bambino/episodio
(Terracciano L. RIAP 2008;2:12)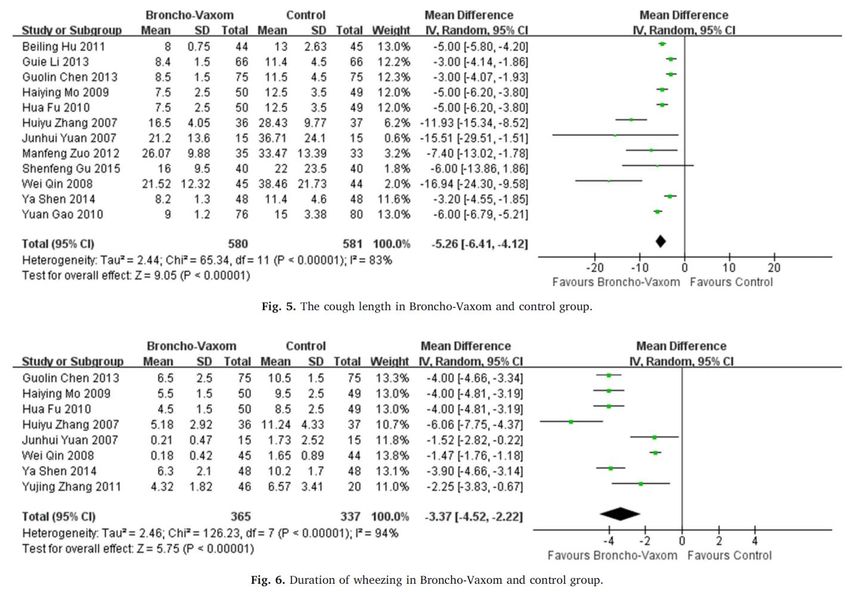
Fattori di rischio individuali
Fattori anatomici individuali
Immaturità immunologica
Immunodepressione postinfettiva
(convalescenza)
Atopia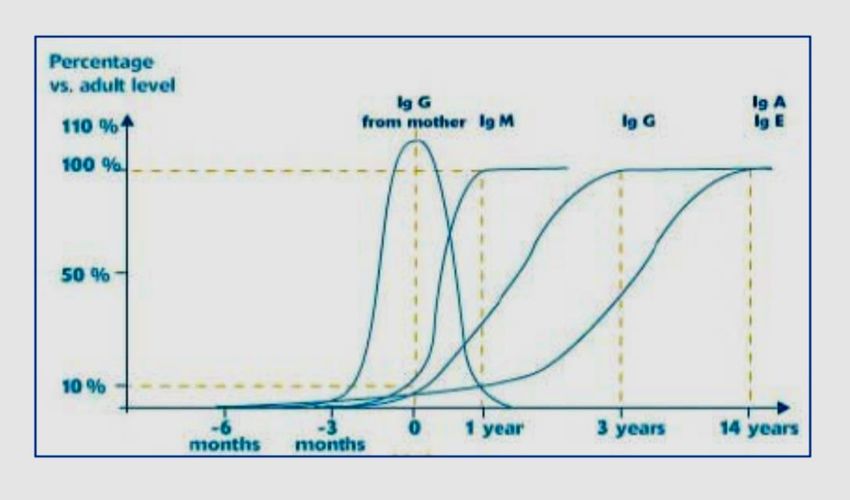
IRR : fattori di rischio individuali
Fisiologica immaturità
immunologica del
bambino !
De Palma A, et al 2004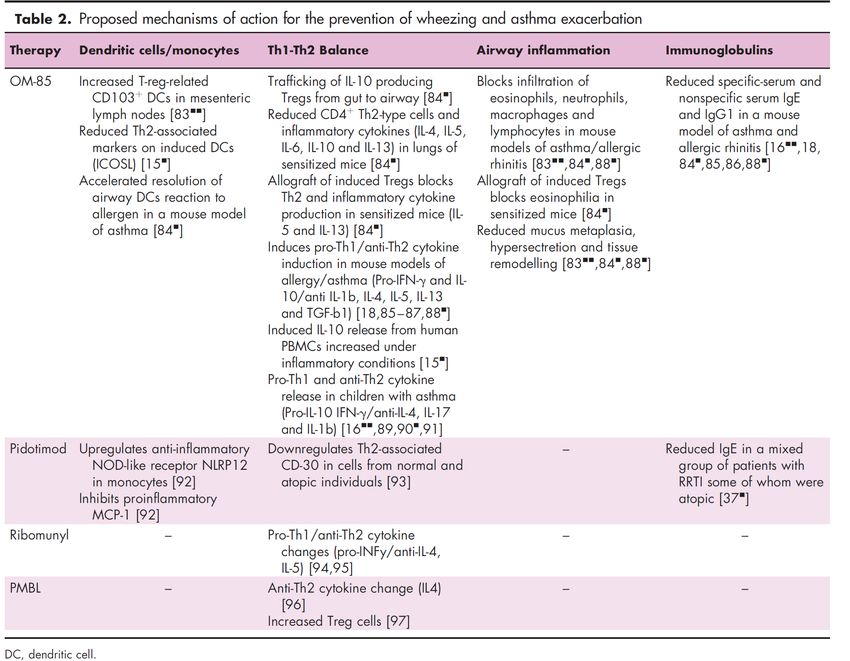
IRR : fattori di rischio individuali
L’immunodeficienza “fisiologica” si traduce in…
difficoltà nella produzione anticorpale, soprattutto verso
antigeni polisaccaridici nei primi 3 anni di vita
la scarsa efficienza delle risposte anticorpali è responsabile anche
di una difettiva memoria immunologica con rischio di recidività
della stessa infezione
alterazione della clearance con conseguente prolungamento della
permanenza dei patogeni nelle mucose nasali e faringee
De Palma A, et al 2004
IRR : fattori di rischio individuali
Azione immunodepressiva delle infezioni virali
riduzione del numero di linfociti CD4+ circolanti
alterata risposta citochinica (ridotta, switch Th1>Th2)
riduzione della fagocitosi macrofagica
riduzione della chemiotassi dei neutrofili
deficit parziale di IgA o delle sottoclassi di IgG
Inoltre il danno causato dai virus alle cellule epiteliali delle vie
aeree puo favorire l’adesione batterica e portare a superinfezione
Cardinale F Pediatr Allergy
Immunol 2001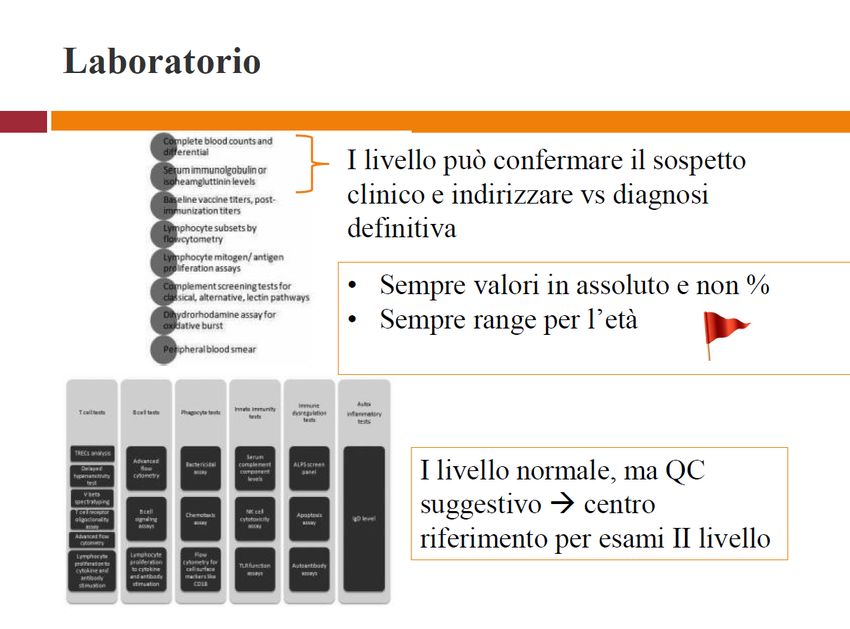
IRR : fattori di rischio individuali
Deficit di IgA
Studio svedese ha identificato 2508 individui con Deficit di IgA
Maggior numero di vari tipi di infezione (PR 2.4)
Significativa associazione con infezioni respiratorie (17.8% vs 6.3%)
ma anche gastrointestinali,urinarie,cutanee,sepsi
Ludvigsson JF et al J Clin
Immunol 2016IRR : fattori di rischio individuali
Presenza di Atopia
persistente flogosi delle vie aeree
rinosinusite ricorrente nel 25-70 % dei pazienti
batteri colonizzatori patogeni del microbioma
possibilità di inizio precoce di IRR
disfunzione immunologica nel 13.2% dei casi
Delle Piane RM Pediatr Med Chir 2009
Ciprandi G PAI 2006
Chicoulaa B Int J Gen Med 2017IRR : fattori di rischio individuali
Basso peso alla nascita
Maggiore frequenza di problemi respiratori all’età di 6-7 anni
Maggiore numero di episodi di wheezing
Maggior numero di diagnosi di asma
Ridotti parametri spirometrici rispetto ai soggetti di pari età
Kwinta P Ital J Pediatr
2013Fattori di rischio ambientali
Il fumo passivo, (ma tutti giurano di fumare
fuori al balcone)
La socializzazione precoce (... sa, la nonna
non ce lo tiene)
La presenza di fratelli (beati i primi...)
Livello socioeconomico basso (?)
non solo i maschi si ammalano di più rispetto alle
femmine (62% vs. 38%), ma i maschi sono più atopici
delle femmine (67% vs. 33%).Quali Fattori predisponenti
determinano una IRR?
Vivere in comunità
Esposizione a fumo passivo
Inquinamento ambientale/domestico
Fattori di Allattamento artificiale
Rischio Precoce socializzazione con frequenza in asili nido
ambientali Basso livello socio-economico e scarsa igiene
Malnutrizione
Stato vaccinale
Stato della vitamina DIRR : fattori di rischio ambientali
Vivere in comunità
Fattore di rischio preponderante
nei mesi invernali in ambienti chiusi e affollati
trasmissione attraverso le goccioline aerosolizzate
contatto diretto con secrezioni contaminate
invasione negli occhi
invasione nell’apparato respiratorio
De Hoog ML BMC Med 2014IRR : fattori di rischio ambientali
Esposizione a fumo passivo
irritazione della mucosa
aumentata permeabilità mucosale
ridotta migrazione di macrofagi e neutrofili
aumento delle IgE totali sieriche
aumentato rischio di sensibilizzazione ad allergeni
soppressione delle difese antibatteriche
Evitare il fumo passivo rappresenta un’efficace misura preventiva
Goldstein AO . Ann Fam Med 2015
Walker N. Nicotine Tob Res. 2015
Cardinale F PAI 2001IRR : fattori di rischio ambientali
Inquinamento ambientale
Non è facile definire i termini di esposizione individuale
iper-reattività bronchiale
consequenziale incremento di infezioni respiratorie
Darrow LA Am J Epidemiol 2014
Liu HA J Allergy Clin Immunol 2015
Inquinamento domestico Trandafir LM EHB 2017
Allergeni domestici, muffe
Eccessiva umidità
Ridotta aerazione
Scarsa pulizia degli impianti di ventilazione
Infezioni respiratorie e patologiche allergiche Smith KR et al. Thorax
2000IRR : fattori di rischio ambientali
Allattamento artificiale
Diversi studi hanno dimostrato l’importanza dell’allattamento al seno
nella riduzione delle IRR
Karmaus W J Asthma 2008; Sniders BEP J Pediatr 2007
Precoce socializzazione con frequenza in asilo nido
Studio register-based su 138.821 ricoveri ospedalieri per ARTI in una
coorte di bb Danesi 0-5 aa : 3.982.925 anni/persona di follow-up
Bb < 12 mesi, primi 6 mesi di day-care associati a +69% rischio di
ricovero
Riduzione rischio ricovero a 47%, 41% e 8%,in bb di età 1,2 e 3aa
Dopo 12 mesi di frequenza day-care e in bb > 3 aa rischio uguale
agli home-care
Rischio di ricovero >4 volte per bb età 0-2 aa senza fratelli
Kamper-Jorgensen,Pediatrics 2006IRR : fattori di rischio ambientali
Basso livello socio-economico e scarsa igiene
In uno studio è stato dimostrato che con il solo lavaggio delle mani:
• bambini< 5 anni:riduzione del 50% di polmoniti rispetto ai controlli
• bambini < 15 anni: riduzione percentuale di tosse, dispnea e rinite
Luby SP Lancet 2005
Malnutrizione
Costituisce un importante fattore di rischio anche se non è facile
stimare con esattezza l’associazione tra IRR e grado di malnutrizione
Black RE Lancet 2008
Schmidt WP J Health Popul Nutr 2011
Stato vaccinale
Le vaccinazioni anti-pneumococcica e anti-influenzale possono
rappresentare un possibile fattore di protezione contro le IRR
Estrada J Pediatr Infect Dis J 2016IRR : fattori di rischio ambientali
Stato della vitamina D
Diversi studi hanno dimostrato che la vitamina D può interferire sulla
funzione di un grosso numero di immunociti con
• accentuazione dei meccanismi innati di difesa immune
• inibizione degli effetti antinfiammatori
Deficit di Vitamina D= più elevato numero di IRR
Una meta-analisi pubblicata quest’anno conferma
la supplementazione di vitamina D come
prevenzione
di IRR nei bambini inoltre:
• il beneficio è maggiore se la supplementazione
è giornaliera o settimanale Martineau AR Health Technol
• il benefico è maggiore nei soggetti Assess 2019
Martineau AR, BMJ 2017
con bassi livelli di vitamina D Muehleisen A JACI 2013
Camargo CA Pediatrics 2011
Camargo CA Pediatrics 2012Infezioni respiratorie ricorrenti:
nuove evidenze e bandierine rosse per
la prevenzione nella pratica quotidiana
Peroni Diego IRR ..
U.O. di Pediatria Le bandierine rosse
Università di Pisa Immunomodulanti e IRR
IRR ma non solo ..
Le novità ..Infezioni respiratorie ricorrenti:
approfondimento diagnostico
Anamnesi – Esame obiettivo
Esame emocromocitometrico
Immunoglobuline siericheFattori costituzionali
Fattori costituzionali
140
120
100
IgM (mg/dl)
80
60
40
20
0
1-3 mesi 4-6 mesi 7-12 13-24 2-3 anni 4-5 anni 6-8 anni 9-11 12-16
mesi mesi anni anni
età
Adeguata risposta a stimoli
proteici
Deficitaria risposta a stimoli
polisaccaridici
IgA secretorie: produzione
dai 3 mesi e lento incrementoInfezioni respiratorie ricorrenti:
approfondimento diagnostico II livello
Anamnesi
Esame obiettivo
Accertamenti immunologici:
- Esame emocromocitometrico
- Immunoglobuline sieriche
- Sottopopolazioni linfocitarie
(CD3, CD4, CD8, CD19, DR, CD16)
- Ab anti-Tetano, Ab anti-epatite
- Ig E totaliI 10 warning signs della Jeffrey Modell Foundation
Le due componenti dell'immunità
INNATA ADATTATIVA
Risposta immediata e generalizzata. Risposta tardiva e specifica.
Macrofagi Linfociti
Granulociti Linfociti B
Neutrofili Immunità Umorale
Basofili Linfociti T
Eosinofili Immunità Cellula-Mediata
Natural Killers
Macrofagi e Neutrofili sono le classiche
“cellule infiammatorie.”Classificazione delle
Immunodeficienze primitive
• Immunodeficienze umorali (50%)
• Immunodeficienze combinate (30%)
• Immunodeficienze da difetto dei fagociti (10%)
• Immunodeficienze da deficit Complemento (2%)
• Immunodeficienze associate a Sindromi (8%)Ipotesi diagnostiche suggerite dai livelli
di immunoglobuline sieriche
IgG IgA IgM IgE Diagnosi suggerita Esami utili per la diagnosi
differenziale
↓↓ ↓↓ ↓↓ ↓↓ XLA, CVID, SCID, Linfociti T – B, SIgA, risposta
Ipogammaglobulinemia anticorpale, isoemoagglutinine
transitoria
↓↓ ↓↓ N/↑ ↓↓ HIGM Linfociti B con IgM-IgD di
membrana
CVID Linfociti B con Ig di membrana
di tutti gli isotipi
N ↓↓ N ↓N↑ Deficit IgA SIgA, sottoclassi IgG
Atassia-teleangectasia
N↓ N↓ N ↓ N Deficit sottoclassi IgG Deficit di 1 o più sottoclassi
N↓ N↓ N N Deficit anticorpale in Sottoclassi normali
normogammaglobulinemia
N N N ↑↑ Sindr. con iper-IgE
Sindr. Wiskott-Aldrich PiastrinopeniaValori normali delle Immunoglobuline
in rapporto all’età
Età IgG (mg/dl) IgA (mg/dl) IgM (mg/dl)
Cordone 1112 (862-1434) Non dosabili 9 (5-14)
ombelicale
1 - 3 mesi 468 (231-495) 24 (8-74) 74 (26-210)
4 - 6 mesi 434 (222-846) 20 (6-60) 62 (28-39)
7 - 12 mesi 569 (351-919) 29 (10-85) 89 (38-204)
13 - 24 mesi 801 (264-1509) 54 (17-178) 128 (48-337)
2 - 3 anni 889 (462-1710) 68 (27-173) 126 (62-257)
4 - 5 anni 1117 (528-1959) 98 (37-257) 119 (49-292)
6 - 8 anni 1164 (633-1016) 113 (41-315) 121 (56-261)
9 - 11 anni 1164 (707-1919) 127 (60-270) 129 (61-276)
12 - 16 anni 1105 (604-1909) 136 (61-301) 132 (59-297)DEFICIT DI IgA:
Definizione
Condizione caratterizzata da bassi livelli sierici di IgA
con livelli sierici di IgG e IgM normali e senza
alterazioni dell’immunità cellulo-mediata.
Frequenza: 1/200 – 1/1000
Deficit assoluto: la presenza di livelli di IgA < 5 mg/dl;
assenza di Ig secretorie;
Deficit parziale: la presenza di livelli di IgA > 5 mg/dl,
ma inferiori ai livelli normali per l’età, Ig secretorie
presenti.DEFICIT ASSOLUTO DI IgA:
Clinica
Molti soggetti sono asintomatici!
Associazioni cliniche: Infezioni
Allergopatie
Enteropatie
Malattie autoimmuni
Celiachia (5% dei celiaci)
TumoriDEFICIT ASSOLUTO DI IgA:
Prognosi
Per i bambini con infezioni respiratorie recidivanti e
severe:
- Antibioticoprofilassi
- Fisiokinesiterapia respiratoria
Per i bambini con patologie associate:
-la normale terapia specifica
La prognosi è nel complesso molto buona.
Deficit parziali 50% di risoluzione entro i 14 anni.
Predisposizione a sviluppare
Immunodeficienza Comune Variabile.ELEMENTI CLINICI CARATTERISTICI Elementi clinici caratteristici Forma Infezioni batteriche politopiche dopo i 6 mesi Deficit anticorpali di vita Infezioni severe batteriche, virali, fungine, e da Immunodeficienze combinate opportunisti sin dai primi mesi di vita, diarrea cronica, arresto di crescita, rash cutaneo, alopecia Infezioni cutanee, polmonari e linfonodali da Deficit dei fagociti batteri o funghi (nel deficit proteine di adesione: ascessi cutanei freddi) Meningiti batteriche (deficit fattori tardivi) Deficit del complemento Malattie autoimmuni (deficit fattori precoci) Piastrinopenia, eczema, infezioni ricorrenti, Sindrome di Wiskott-Aldrich autoimmunità Infezioni stafilococciche, lineamenti grossolani, Sindrome da iper-IgE ritardo caduta denti decidui
Infezioni respiratorie ricorrenti:
nuove evidenze e bandierine rosse per
la prevenzione nella pratica quotidiana
Peroni Diego IRR ..
U.O. di Pediatria Le bandierine rosse
Università di Pisa Immunomodulanti e IRR
I meccanismi
IRR ma non solo ..
Le novità ..Come gestire le IRR ?
Gli Immunomodulanti
Immunostimulators are substances that interact
with the immune system and modulate its
function by stimulating a more rapid and effective
immune response
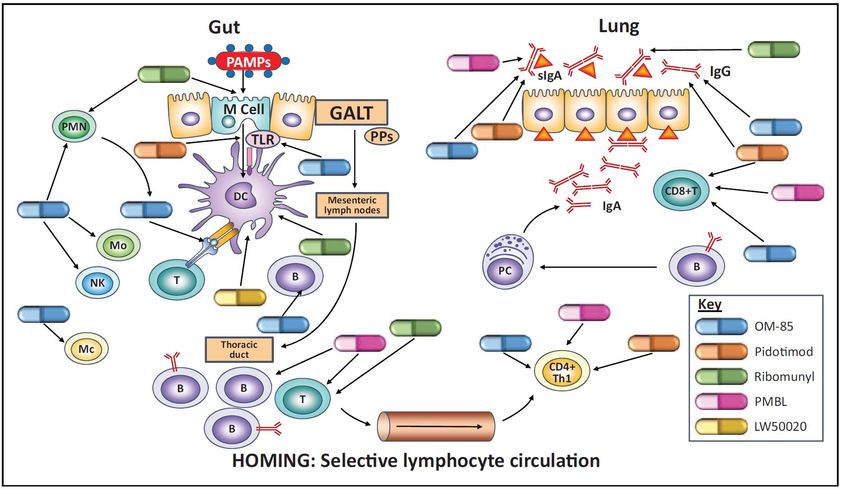
Allergy Asthma Proc 30:S21–S31, 2009S Esposito, COACI, 2018 The gut–lung immune axis illustrating points of immunomodulator activity in RTI prophylaxis
S Esposito, COACI, 2018 Antigen sampling by M cells and dendritic cells resident in the Peyer’s patches of the gut-associated lymphoid tissue leads to maturation of dendritic cells into an antigen-presenting cell phenotype. The subsequent dendritic cell-initiated immune cascade involves homing of cells from both innate and adaptive branches of the immune system to the mucosal-associated lymphoid tissue of the lungs and subsequent antibody production. They can also act to aid maturation of the immune system in children, correcting T helper cell (Th) Th1/Th2 imbalance through activation of T regulatory (Treg) cells. The correction of this Th2-oriented imbalance and other anti- inflammatory activities may reduce atopic responses related to wheezing and asthma.
OM-85 is the product of alkaline lysis of 21 strains of common bacterial respiratory tract pathogens . The active ingredients of OM-85 are resistant to gastric transit and cause maturation of mucosal dendritic cells in gastrointestinal Peyer’s patches, a key step in orally induced respiratory immunity. OM-85-induced dendritic cell activation occurs in a modulated manner, resulting in a putative prealert antiinfective state in the mucosal immune system
Induced dendritic cells release chemokines that act on monocytes and natural killer (NK) cells, as well as prophagocytic chemokines which induce polymorphonuclear neutrophil migration. The downstream effects on OM-85 on the innate immune system include the release of antimicrobial peptides and the activation of macrophages resulting in expression of proinflammatory and antiviral cytokines. OM-85 reduced rhinovirus infection of lung epithelial cells and cell death in vitro. Data also suggest that OM-85 causes more rapid neutrophil recruitment in response to viral infection, reducing viral load.
OM-85 modulates rhinovirus docking proteins on human airway epithelial cells via Erk1/2 mitogen activated protein kinase and cAMP. Roth M, PLoS ONE 2017; 12(11): e0188010. Representative IF images for RV infection (green) in primary BEC; nuclei were stained for cell counting by EVOS live cell staining kit. Light microscopic images are depicted for the effect of OM- 85 and RV infection on BEC phenotype. (B-D) Quantitation of RV infection of BEC by IF. BEC were pretreated for 24 or 48 hrs with OM-85 (10 μg/ml).
OM-85 modulates rhinovirus docking proteins on human airway epithelial cells via Erk1/2 mitogen activated protein kinase and cAMP. Roth M, PLoS ONE 2017; 12(11): e0188010. RV induced expression of ICAM-1 on BEC is prevented by OM-85 through cAMP and Erk1/2 MAPK. Increased expression of ICAM-1 by RV and its inhibition by OM-85 pre- incubation (24 hrs).
Infezioni respiratorie ricorrenti:
nuove evidenze e bandierine rosse per
la prevenzione nella pratica quotidiana
Peroni Diego IRR ..
U.O. di Pediatria Le bandierine rosse
Università di Pisa Immunomodulanti e IRR
L’efficacia
IRR ma non solo ..
Le novità ..EFFICACY OF IMMUNOMODULATORS IN CHILDREN WITH
RESPIRATORY TRACT INFECTION
OM-85 reduced the duration of infections in children with a history of
RRTI compared with placebo and versus probiotic therapy.
In a study of children with recurrent tonsillitis, OM-85 prophylaxis
improved outcomes in the majority of patients and, importantly,
removed the need for surgery in a significant proportion of those
treated [Bitar MA, 2013].
In children with subacute sinusitis, OM-85 prophylaxis sped recovery
and reduced infections [Gomez Barreto D, 1998],
whereas children with chronic rhinosinusitis had a reduced symptom
burden and a lower incidence of attacks [Chen J, 2017].
Reductions in antibiotic and drug treatment following prophylactic
therapy with OM-85 have also been demonstrated in children with a
history of RRTI, subacute.
OM-85 therapy reduced school absenteeism in childrenEFFICACY OF IMMUNOMODULATORS IN CHILDREN WITH
RESPIRATORY TRACT INFECTION
OM-85 reduced the duration of infections in children with a history of
RRTI compared with placebo and versus probiotic therapy.
In a study of children with recurrent tonsillitis, OM-85 prophylaxis
improved outcomes in the majority of patients and, importantly,
removed the need for surgery in a significant proportion of those
treated [Bitar MA, 2013].
Gli effetti indesiderati con l’uso di
In children with subacute sinusitis, OM-85 prophylaxis sped recovery
OM-85 sono lievi e transitori.
and reduced infections [Gomez Barreto D, 1998],
Questo profilo di sicurezza è
whereas children with chronic rhinosinusitis had a reduced symptom
stabile
burden and a lower ancheof se
incidence utilizzato
attacks [Chen J,a2017].
lungo
Reductions in antibiotic and drug treatment following prophylactic
therapy with OM-85 have also been demonstrated in children with a
history of RRTI, subacute.
OM-85 therapy reduced school absenteeism in childrenOM-85 in pediatric recurrent respiratory tract infections: A systematic review and meta-analysis. YIN J, Intern Immunopham 2018; 54,198 53 RCTs involving 4851 pediatric patients were included in this meta-analysis. Frequency of RTIs in OM-85 and control group
OM-85 in pediatric recurrent respiratory tract infections: A systematic review and meta-analysis. YIN J, Intern Immunopham 2018; 54,198 53 RCTs involving 4851 pediatric patients were included in this meta-analysis. Cough length and frequency of wheezing in OM- 85 and control group
Impact of OM-85 Given during Two Consecutive Years to Children with a History of Recurrent Respiratory Tract Infections: A Retrospective Study. Esposito, Int. J. Environ. Res. Public Health 2019, 16, 1065; 200 children aged three to six years history of recurrent RTIs, defined as at least six documented episodes of acute RTI in a single year, received OM-85 for two consecutive years (3.5 mg once a day for 10 days for 3 months of each year) were selected and matched based on age, sex, and period of evaluation with children with recurrent RTIs who did not receive OM-85.
EFFICACY OF IMMUNOMODULATORS IN CHILDREN WITH RESPIRATORY TRACT INFECTION Pidotimod prophylaxis also results in less antibiotic use [Namazova LS, 2014], Less hospitalization and paediatric visits and school absenteeism [Caramia G, 2008] Where reported, adverse events were infrequent, mild and transient. Studies on pidotimod in particular lacked reporting of safety, control groups or information on the definition of RRTI, particularly in foreign language abstract-only publications.
Metabolomic profile of children with recurrent respiratory infections.
Bozzetto S Pharmacol Res 2017;115:162
L’analisi metabolomica ha riscontrato
138 metaboliti urinari diversi tra i
bambini con IRR e i controlli sani.
Dopo trattamento con Pidotimod la
differenza si è ridotta a 34
L’analisi metabolomica ha evidenziato metaboliti.
differenze sostanziali tra il profilo
metabolico dei bambini con infezioni
respiratorie ricorrenti (IRR) e i controlli2011 Issue 6 CD004974 TUTTI gli immunostimolanti studiati (estratti batterici, pidotimod) riducono di circa il 40% il numero delle infezioni respiratorie, rispetto al placebo.
2011 Issue 6 CD004974 TUTTI gli immunostimolanti studiati (estratti batterici, pidotimod) riducono di circa il 40% il numero delle infezioni respiratorie, rispetto al placebo.
Infezioni respiratorie ricorrenti:
nuove evidenze e bandierine rosse per
la prevenzione nella pratica quotidiana
Peroni Diego IRR ..
U.O. di Pediatria Le bandierine rosse
Università di Pisa Immunomodulanti e IRR
IRR ma non solo ..
Le novità ..EFFICACY OF IMMUNOMODULATORS IN
WHEEZING AND ASTHMA
OM-85 prophylaxis reduced the duration and incidence of
wheezing/asthma exacerbations in children with a history
or recurrent wheezing or asthma [Lu Y, 2015, Razi C,
2010], as well as hospitalizations related to asthma [Chen
ZG; 2009].
The reductions in exacerbations appear to be related to
reduced incidence of RTIs.
Safety data and its addition to corticosteroid therapy
caused no apparent issues.EFFICACY OF IMMUNOMODULATORS IN
WHEEZING AND ASTHMA
The two studies investigating pidotimod in asthma
and the related condition obstructive syndrome did
not report data on asthma exacerbations; however,
there were reductions in the incidence of RTI in both
studies [Lokshina EE, 2011].
RTI duration was also reduced in children with allergic
rhinitis and asthma [Vargas Correa, 2002].The immunostimulant OM-85 BV prevents wheezing attacks in preschool children. Razi JACI, 2010;126:763 75 children with recurrent wheezing who were 1 to 6 years old. Participants were randomly assigned to groups given either OM-85 or a placebo (1 cps per day for 10 days each month for 3 consecutive months) at the start of the trial. Participants were followed for 12 months
The immunostimulant OM-85 BV prevents wheezing attacks in preschool children. Razi JACI, 2010;126:763 75 children with recurrent wheezing who were 1 to 6 years old. Participants were randomly assigned to groups given either OM-85 or a placebo (1 cps per day for 10 days each month for 3 consecutive months) at the start of the trial. Participants were followed for 12 months
Can we prevent exacerbations of asthma caused by common cold
viruses? Weinberger M JACI, 2010 Oct;126(4):770
‘‘We can put a man on the moon, so why can’t we cure the
common cold?’’ This colloquial question is certainly not trivial
to those of us that care for asthma, especially asthma in the
preschool-age child.
The common cold, caused by rhinovirus and other viral
respiratory infections, a nuisance illness to most,
is the major cause of serious asthma exacerbations. Viral
respiratory infections are the major cause of asthma
exacerbations at all ages 1-3 and appear to be the major risk
factor
Becausefor the
the large increase
current in clinical
controlled hospitaltrial
admissions for
was registered
asthma that occurs in
in ClinicalTrials.gov every autumn.
2008 as a phase IV study, is there
any realistic expectation that these questions are likely to
addressed? If they are not, is there any realistic likelihood
that US Food and Drug Administration approval for
marketing in the United States is likely to occur within the
foreseeable future? These are, of course, rhetorical
questions.Infezioni respiratorie ricorrenti:
nuove evidenze e bandierine rosse per
la prevenzione nella pratica quotidiana
Peroni Diego IRR ..
U.O. di Pediatria Le bandierine rosse
Università di Pisa Immunomodulanti e IRR
IRR ma non solo ..
Le novità ..Early Origins of Asthma: Role of Microbial Dysbiosis and Metabolic Dysfunction
F. Martinez, AJRCCM 2017Holt PG. Prevention – what is the most promising approach?
Pediatr Allergy Immunol 2014;25:12-4.
And wheezing.. The next future
The ORal Bacterial EXtracts for the prevention of wheezing lower
respiratory tract illness (ORBEX) trial represents a step change in
immunomodulatory research.
This large, multicentre, NIH-funded RCT (NCT02148796) will enrol
upwards of 1000 infants at high asthma risk due to having atopic
eczema and/or parents or siblings with asthma.
https://clinicaltrials.gov/ct2/show/NCT02148796.Early Origins of Asthma: Role of Microbial Dysbiosis and Metabolic Dysfunction
F. Martinez, AJRCCM 2017
And wheezing.. The next future
Participants will receive long-term OM-85 prophylaxis (3.5 mg/day
for 10 days/month for 2 years).
The primary outcome will be time to first wheezing episode in the
third observational year when children are not receiving prophylaxis.
Preliminary results of the ORBEX trial are expected by December
2022.
https://clinicaltrials.gov/ct2/show/NCT02148796.The ORBEX trial This is a 36 month parallel arm, double-blind, placebo-controlled trial for the prevention of WLRI into the third to fifth year of life (30 to 54 mo. inclusive) in young children (6-18 months old) at increased risk for asthma. The trial will be divided into 2 periods. During the initial treatment period (first and second years in the study) participants will receive OM-85 (3.5 mg) or placebo for ten days each month for two consecutive years. This period will allow the observation of key secondary outcomes while participants are receiving therapy. https://clinicaltrials.gov/ct2/show/NCT02148796.
The ORBEX trial This is a 36 month parallel arm, double-blind, placebo-controlled trial for the prevention of WLRI into the third to fifth year of life (30 to 54 mo. inclusive) in young children (6-18 months old) at increased risk for asthma. The trial will be divided into 2 periods. The second period (third year in the study) will be a one year observation of the time to occurrence of the first WLRI episode (primary outcome) while off study drug along with the secondary outcomes noted above. https://clinicaltrials.gov/ct2/show/NCT02148796.
The Orbex trial Primary Outcome Measures : The time to the occurrence of the first WLRI episode in the third observation year while not receiving study drug Secondary Outcome Measures : The time to first WLRI during the two treatment years while receiving study drug The annualized rate of WLRI episodes during the two years while receiving study drug The annualized rate of WLRI episodes during the third observation year while not receiving study drug The annualized rate of severe wheezing respiratory tract illness (SWLRI) episodes during the two treatment years while receiving study drug. The annualized rate of severe wheezing respiratory tract illness (SWLRI) episodes during the third observation year while not receiving study drug. Number of participants with adverse events Safety and tolerability of OM-85 while receiving study drug during the two year treatment period Number of participants with adverse events
Treatment of pregnant mice with a
defined, clinically approved immune
modulator was shown to markedly reduce
susceptibility of their offspring to
development of the hallmark clinical
features of allergic airway inflammatory
disease
We provide evidence that the principal target for maternal
treatment effects was the fetal dendritic cell progenitor
compartment, equipping the offspring for accelerated functional
maturation of the airway mucosal dendritic cell network following
birth.
These data provide proof of concept supporting the rationale for
developing transplacental immune reprogramming approaches for
primary disease prevention.Puoi anche leggere