La terapia del dolore in onco-ematologia e le terapie di supporto - Elena Bandieri - Studio ER Congressi
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
La terapia del dolore in onco- ematologia e le terapie di supporto. Elena Bandieri USL Modena

Qual’è lo stato dell’arte sulla gestione del
dolore oncologico?
Is pain in patients with haematological
malignancies under-recognised? The results
from Italian ECAD-O survey
E. Bandieri, D. Sichetti, M. Luppi, C. Ripamonti, G. Tognoni
Leuk Res 2010
Pain intensity ST 59.4% moderate severe
HT 67.3% moderate-severe
Il setting condiziona l’appropriatezza prescrittiva
“…The patient’s level of
worst pain is subtracted
from the most potent level
of analgesic drug therapies
as prescribed by the
physician…”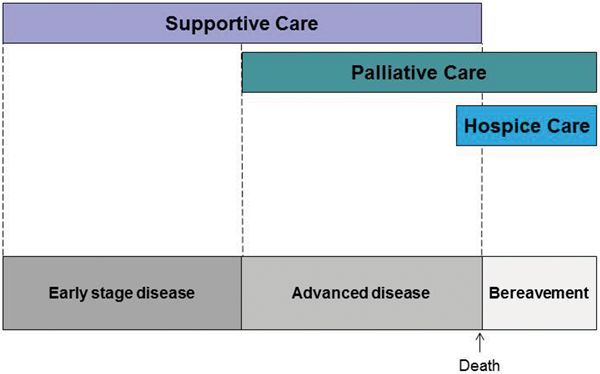
Gestione del dolore onco-ematologico
ancora insoddisfaciente
BISOGNI:
• 1) ottimizzazione della terapia analgesica
(cronica ad orari fissi e del BTcP);
• 2) un approccio farmacologico migliore non è
sufficiente per se: il miglioramento della
terapia del dolore deve avvenire nel contesto di
un nuovo modello di cure supportivo/palliative
precoci.
Gestione del dolore da cancro ancora
insoddisfaciente.
:
BISOGNI:
• 1) ottimizzazione della terapia cronica
ad orari fissi (ATC) (II vs III gradino
OMS);
• 2) un approccio farmacologico migliore
non è sufficiente per se: il
miglioramento della terapia del dolore
deve avvenire nel contesto di un nuovo
modello di cure palliative precoci.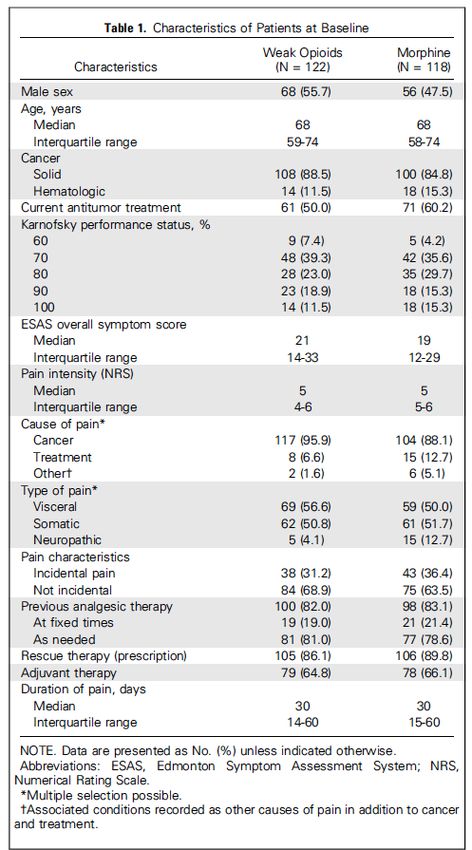
Strategia farmacologica:
i “tre gradini” OMS
I “tre gradini” consentono di
controllare il dolore oncologico
cronico in circa il 90% dei casi.
Tale approccio, sviluppato nel
1986 da un gruppo di esperti
dell’ Organizzazione Mondiale
della Sanità (OMS), fornisce
specifiche indicazioni per la
scelta della terapia
antidolorifica che non va
somministrata al bisogno ma
a orari fissi.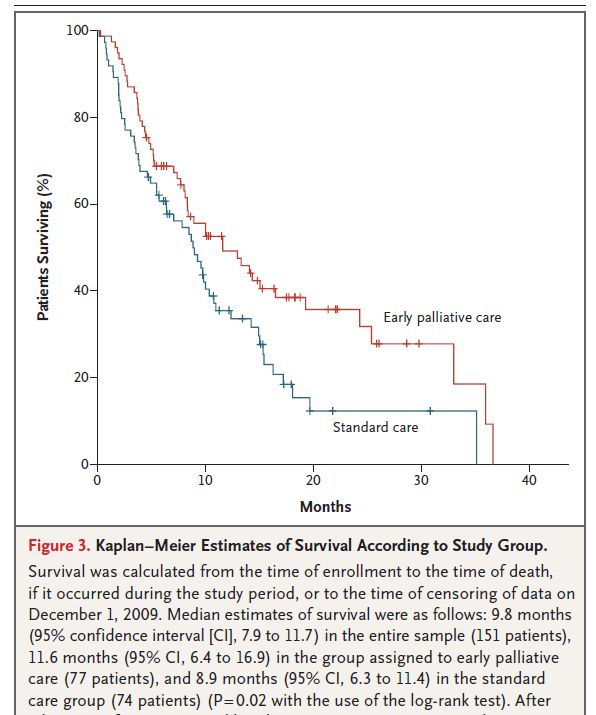
La strategia a 3 gradini è validata?
Perché si cambia gradino?
• Numerosi studi sono stati condotti per validare
tale approccio metodologico: sono stati
osservati oltre 8.000 pazienti in diversi paesi
del mondo ed in ambienti clinici differenziati
(ospedale e domicilio).
• Le varie casistiche riportano un efficace
controllo del dolore nel 71-100% dei pazienti
trattati.
• Tra gli studi eseguiti per validare l’approccio
OMS quello di Ventafridda et al, (Cancer 1997)
condotto su 1.229 pazienti seguiti per 2 anni, ha
evidenziato che il passaggio dal 1° al 2° gradino
è dovuto in circa la metà dei casi ad effetti
collaterali e nell’altra metà all’inefficacia
analgesica, mentre il passaggio dal 2° al 3°
gradino è soprattutto dovuto all’inefficacia
analgesica. Efficacia media dei farmaci del
secondo gradino è di 3 settimane.
Criticità sul secondo gradino
• Hanno tutti un “effetto tetto”: ciò significa che
aumentando la dose di un farmaco oltre una certa soglia
l’efficacia non aumenta (ma possono aumentare gli effetti
indesiderati).
• Le specialità a base di codeina disponibili in Italia non
hanno dosaggi ottimali. Non permettono di raggiungere
la dose massima efficace di codeina (360 mg/die) senza
somministrare dosaggi tossici di paracetamolo (la scheda
tecnica indica 3-4 gr/die).
E le evidenze disponibili?:
• Non dimostrano una chiara differenza nell’efficacia dei
farmaci del 1° e del 2° gradino;
• Non permettono di concludere sui benefici dell’aggiunta
degli oppioidi minori - in particolare codeina - rispetto al
solo paracetamolo o al FANS. Overall, the limited evidence provided by these studies shows that oral morphine at low doses can be used in opioid-naive cancer patients and that in some patients pain relief might be better than that achieved with step II drugs…”
QUESITO E’ possibile abolire il secondo gradino, cioè anticipare il terzo gradino al posto del secondo gradino nella terapia analgesica del dolore moderato da cancro ?
STUDIO INDEPENDENTE NO SPONSOR
Lo studio ha mostrato un vantaggio altamente significativo nell’ utilizzo della morfina: tra i 118 pazienti che hanno ricevuto la morfina, piu’ dell’ 88% ha presentato una riduzione del 20% nell’ intensità del dolore, laddove tale riduzione si è potuta riscontrare nel solo 57% dei 122 pazienti che hanno ricevuto oppioidi deboli.
In questo studio multicentrico randomizzato, della durata di 28 giorni, la morfina a basse dosi confrontata con gli oppioidi deboli ha ridotto in modo statisticamente significativo l’intensità del dolore, già nei primi 7 giorni di terapia. L’efficacia minore e piu’ tardiva degli oppioidi deboli ha portato i clinici a sostituire piu’ frequentemente gli oppiodi deboli con quelli maggiori nel trattamento del dolore moderato da cancro nel periodo di studio.
Gli effetti collaterali piu’ frequentemente associati al trattamento con oppioidi risultavano paragonabili sia come intensità che frequenza tanto nei pazienti che ricevevano morfina a basse dosi quanto nei pazienti che ricevevano oppioidi minori.
La condizione generale dei pazienti basata sulla valutazione dei sintomi fisici ed emozionali nel punteggio globale di tutti i sintomi misurati dall‘ Edmonton Symptom Assessment System (ESAS), era migliore nel gruppo di pazienti trattati con morfina.
Sebbene gli oppioidi deboli siano efficaci quando usati per brevi periodi, la morfina a basse dosi può essere utilmente anticipata nella terapia del dolore moderato da cancro, per la sua maggiore efficacia e paragonabile profilo di tossicità.
Gestione del dolore da cancro ancora
insoddisfaciente, sebbene migliorata.
:
BISOGNI:
• 1) ottimizzazione della terapia analgesica
• 2) un approccio farmacologico migliore
non è sufficiente per se: il
miglioramento della terapia del dolore
deve avvenire nel contesto di un nuovo
modello di cure supportive/palliative
precoci.Studio multicentrico in 32 ospedali, 1450 pts.con dolore da cancro: 602 con accesso a standard care (SOC) e 848 con accesso a cure palliativa/ supporto precoci (ePSC). Un’analisi multivariata ha mostrato che il modello ePSC è un fattore indipendente in grado di ridurre il rischio di dolore severo del 31%
Cure supporto/Cure palliative:
contenuto
ESMO definisce Supportive care la cura che ha come obiettivo di
ottimizzare “comfort, function, and social support” a pazienti e
famigliari in tutti gli stadi di malattia, inclusa la malattia curabile.
ESMO definisce Palliative Care la stessa cura rivolta ad una
malattia incurabile.
I termini descrivono programmi clinici comuni
con l’obiettivo primario di controllare i sintomi
fisici (in primis il dolore) psicosociali e
spirituali di pazienti con patologia oncologica e
loro famigliari.E. BOOK ASCO 2013
L’intervento precoce di cure supporto/
palliative: quali evidenze?Early Versus Delayed Early Palliative Oncology Care
VOLUME 33 ! NUMBER 13 ! MAY 1 2015
JOURNAL OF CLINICAL ONCOLOGY
VOLUME 33 ! NUMBER 13 ! MAY 1 2015
O R I G I N A L R E P O R T
mographic and Clinical Characteristics of Table 1. Baseline Demographic and Clinical Characteristics of
Patient Participants Patient Participants (continued)
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
Delayed Delayed
Early Group Group Early Group Group
(n ! 104) (n ! 103)
Marie A. Bakitas, J. Nicholas Dionne- Early Versus Delayed Initiation(nof! Concurrent
104) (n ! Palliative
103)
No. %
Odom, and Andres Azuero, University
No. % P
!
of Alabama at Birmingham, Birming- OncologyCharacteristic
Care: Patient Outcomes No. in%the ENABLE No. % III P!
ham, AL; Marie A. Bakitas, Jennifer
Randomized
Marie A. Bakitas, J. Nicholas Dionne- Early Versus Delayed
Controlled Trial 4 Initiation of Concurrent Palliative
.68
Frost, and Konstantin H. Dragnev, 6 to 12 7.27 4 6.78
64.03 64.6
Odom, and Andres Azuero, University
Dartmouth-Hitchcock Medical Center;
of Alabama at Birmingham, Birming-
Marie A.#
Oncology Care: Patient
12 Tor D. Tosteson, Zhigang Li, Kathleen
Bakitas,
Outcomes
42D. Lyons,
76.36
in Versus
Early the ENABLE
48 Zhongze81.36
Jay G. Hull, Li,
III Palliative Oncology Care
Delayed Early
Zhongze Li, Norris Cotton Cancer
10.28 9.59
ham, AL;
Center, Lebanon; TorFrost,
Marie A. Bakitas, Jennifer
D. Tosteson,
No.A.of
and Konstantin H. Dragnev, Randomized
J. Nicholas Dionne-Odom,
packs per day Controlled
Jennifer Frost, TrialMark T. Hegel, Andres Azuero, .06
Konstantin H. Dragnev,
Kathleen D. Lyons, and and Tim
Mark T. Hegel, Medical Center;
Dartmouth-Hitchcock
Ahles
56 53.85 53 51.46
Geisel School of Medicine
Zhongze .78
at Li,
Dart- ! .5Marie A. Bakitas, Tor D. Tosteson, Zhigang
Norris Cotton Cancer 15 Li, Kathleen
27.27 24Jay G. Hull,
D. Lyons, 40.68Zhongze Li,
mouth; Zhigang Li and Jay G.
See accompanying
Hull, Tor D. Tosteson,
editorial
J. Nicholas on pageJennifer
Dionne-Odom, 1420 Frost, Konstantin H. Dragnev, Mark T. Hegel, Andres Azuero,
Center,
Dartmouth College, Hanover,
.68
Lebanon;
NH;
Table 1. Baseline
1 and Tim A. Ahles
and and Mark T. Hegel,
Demographic and
23 Clinical Characteristics
41.82 16 of
27.12 Table 1. Baseline Demographic and Clinical Characterist
Kathleen D. Lyons,
7 6.73 5 4.85
Tim A. Ahles, Memorial Sloan-Kettering
Geisel School of Medicine at Dart- A Patient
B
1.5 See accompanying editorial on page111420 20 S Participants
T R A C T 5 8.47 Patient Participants (continued)
Cancer Center, Newmouth;
York, NY.
Zhigang Li and Jay G. Hull,
tner 69 66.35 66 64.08 Dartmouth College, Hanover,
Published online ahead of print at
NH; and 2
Purpose 2 3.64 6 Delayed 10.17 Dela
15 14.42 Within 30-60 days
21
www.jco.org on20.39
March 23, 2015.
Cancer Center, New York, NY.
Randomized controlled trials have supported
Tim A. Ahles, Memorial Sloan-Kettering
2.5
A B
0 integrated
Early S T oncology
Group
however, optimal timing has not been evaluated. We investigated the effect of early versus
(n !
0.0
104)
R A C and
3
(n !
T palliative care (PC);
Group
103)
5.08 3-month delay Early Group
(n ! 104) (n
Gro
!
13 12.5 11
Supported by 10.68
Grant No.
Published online ahead of print delayed
at
Purpose
3PC on quality of life (QOL), symptom impact, 3 mood,5.451-year4survival, 6.78 and resource use.
R01NR011871-01 from the National Insti- Randomized controlled trials have supported integrated oncology and palliative care (PC);
tute for Nursing Research; by a.05 Used and other tobacco 13No.evaluated. 12.5
% We13 12.62
%the 1.00
www.jco.org on March 23, 2015.
Cancer Patients Characteristic
however,
Methods optimal timing has not been No.
investigated P! of early versus
effect Characteristic No. % No.
and Leukemia Group Supported by Grant
Clini- No. Between October 2010
8 7.69 3 2.91 B Foundation
Alcoholic delayed
beverages PC onandin March
quality
typical 2013,
of life (QOL), 207symptom
patientsimpact,with advanced
mood, 1-year cancer at a and
survival, National
resource use.
cal Scholar Award; byR01NR011871-01 from the National Insti-
the Foundation for
CancerAge,Institute
Research; by a Cancer week
years cancer center, a Veterans Affairs 2.56 Medical 5.76Center, 1.22and community
2.84 .04 .68outreach 6 to 12 4 7.27 4
61 58.65 50 Medical48.54
Informed tute for Nursingby
Decision-Making;
clinics werePatients
randomly and Methods
assigned toandreceive an2013,in-person PC consultation, structured PCa National
Grants No. P30CA023108, and Leukemia
UL1 Group B Foundation
CAGE‡ Mean
Clini- Between October 2010 March 0.84 64.03 2071.01patients with64.6advanced
0.77 and 0.6 cancer
.82 at # 12 42 76.36 48
35 33.65 50
TR001086, and 48.54 cal Scholar an
R03NR014915; telehealth
Award; by the Foundation for nurse
Cancer coaching
Institutesessions (once per
cancer center, week forAffairs
a Veterans six sessions),
Medical 9.59 Center, monthly follow-up outreach
and community
either bySDearly after enrollment or 3 months later. 10.28
Outcomes were QOL, symptom impact, No. of packs per day
NIH/NINR Small Research Informed Medical Decision-Making;
Grant
.52 Caregiverclinics enrolled were randomly assigned 63
to receive 60.58
an 61
in-person PC 59.22
consultation,.89 mood, structured PC
Grants No.Li); P30CA023108, UL1
1R03NR014915-01 (Zhigang by Norris 1-yearMale survival,
sex and resource
telehealth nurse use (hospital/intensive
coaching sessions 56 (once care
53.85
per unit for
week days,
53 six emergency
51.46
sessions), room
and .78 visits, follow-up
monthly ! .5 15 27.27 24
102 98.08 98 Cancer Center 95.15 TR001086, and by
R03NR014915; an Lives in rural
chemotherapy in area
last 62 59.62 60 58.25 .78
early14after
days, and death location).
Cotton pilot funding;
NIH/NINR Small Research Grant Marital status either enrollment or 3 months later. Outcomes were QOL, symptom .68 impact, mood, 1 23 41.82 16
1R03NR014915-01 (Zhigang Li); Diagnosis .97
the Dartmouth-Hitchcock Section of Palli-
0 0.0 1 Medicine; by0.97 by Norris
Results 1-year survival, and resource use (hospital/intensive care unit days, emergency room visits,
Initial, standardized
ative a National Palliative
Cotton Cancer Center pilot funding; by
Overall
Never
Lung married
chemotherapy
patient-reported in last were
outcomes 14 days, and46 7
death location).
not statistically
6.73
44.23 after
significant
5
42 enrollment 4.85
40.78(QOL, P ! .34; 1.5 11 20 5
2 1.92 3 2.91
Care Research Center Junior Career
the Dartmouth-Hitchcock Section of Palli-
ative Medicine; by a Nationalsymptom
Development Award (M.A.B.); by Grant Married
GI impact,
tract or Pliving
Results ! .09; with partner
mood, P ! .33) or before 69 death
26 66.35
25 (QOL, P24 66 64.08 impact, P !
! .73; symptom
23.3 2 2 3.64 6
0 0.0 No.15R25CA047888 0.97
consultation by a PC
Palliative
from the University
Care Research Center Junior.30; Careermood,
Divorced POverall
! .82).
or Kaplan-Meier 1-year
patient-reported
separated outcomes survival
were
15 rates were 63%significant
not statistically
14.42 in the early
21 after
20.39group and 48%
enrollment (QOL,in P ! .34; 2.5 0 0.0 3
of Alabama at Birmingham Cancer
Breast symptom P10 9.62 13early to12.62
Prevention and Control Training.96
Development Award (M.A.B.);
Program
the delayed
by Grant group (difference,
impact, P 15%;! .09; Pmood,! .038). Relative
! .33) ratesdeath
or before of (QOL, Pdelayed decedents’
! .73; symptom impact, P !
Widowed 13 12.5 11 10.68 3 3 5.45 4
34 32.69 31
(J.N.D.-O.); and 30.1
No. 5R25CA047888 from theresource
by Mentored Research
of Alabama at Birmingham Cancer
Scholar Grant No. MRSG 12-113-01-
University
unit
Other
days
Education
usesolid
(0.68;
were
.30;
the
Genitourinary
95%
similar
tumor
mood,
delayedCI,
P !for
0.23
group to
tract last 14
hospital
.82).
2.02; P
days (0.73;
Kaplan-Meier
(difference,
! .49),
15%;
10 95%
1-year
emergency
P
7 days
!
CI,9.62
survival 0.41
room
.038).
rates to101.27;63%
were
visits
Relative
6.736.7; CI,
P ! 9.71
(0.73;
rates
in
95%
of clinician and six
.26),
theintensive
CI,
early
early group
0.45
to .05 to
delayed
care
1.19;
and 48% in
Used other tobacco
decedents’ 13 12.5 13
P9 !0.41 8.74
Prevention and Control Training Program
31 29.81 32 in Applied31.07 (J.N.D.-O.); and by MentoredPResearch! .21), chemotherapy
resource useinwere daysfor(1.57; 95% CI, 0.37
(0.73;to95% .27),toand home
P ! death (27
similar hospital
structured weekly
1.27; .26), intensive care
CPPB and Clinical Research
from the American Cancer Society "
[54%]Hematologic
High
v 28 [47%];
school
unit days
graduate
Pmalignancy
!
8
.60).95% CI, 0.23 to 2.02;5P ! .49), emergency
(0.68;
7.69
4.81 3
5room visits 2.91
4.85 (0.73; 95% CI, 0.45 to 1.19;
Alcoholic beverages in typical
1 0.96 0 0.0 Scholar Grant No. MRSG 12-113-01-
week 2.56 5.76 1.22
CPPB in Applied and Clinical ResearchHigh school graduate 61 (1.57; 58.65 50 to 6.7;48.54
(K.D.L.).
Disease P ! .21),
status atchemotherapy
enrollment in last 14 days 95% CI, 0.37 P ! .27),.24 and home death (27
23
13
22.12
12.5
21
Presented
15
20.39
at the 50thfrom the American
Annual
(K.D.L.).
14.56May
of the American Society of Clinical
Conclusion [54%] v 28 [47%]; P ! .60).
MeetingCancer Society
Early-entryCollege
New graduate patient-reported outcomes
participants’
diagnosis 35
48 and 33.65
resource
46.15 50 use were
46 48.54
44.66
telephone coaching
not statistically CAGE‡ 0.84 1.01 0.77
different; however,
Conclusion their survival 1-year after enrollment was improved compared with those who Caregiver enrolled 63 60.58 61
2 1.92
Oncology, Chicago, IL,
4
2014. 3.88
30-June 3,
Presented at the 50th Annual Meeting
of the American Society of began
Race†
Recurrence
Clinical 3 months
Chicago, IL, Mayremains
White
Early-entry participants’ the
later. Understanding
different; however,
3, an important research priority. their
complex
survival
29 mechanisms
patient-reported
102
1-year after
27.88 whereby
outcomes
98.08
enrollment
20 resource
and
98
was
PC 19.42
improved95.15
sessions by an
mayuse improve
compared
.52
weresurvival
not statistically
with those who
Lives in rural area 62 59.62 60
Authors’ disclosuresOncology,
of potential.33 30-June Progression 27 25.96 36 34.95
37 35.58
conflicts of interest are
40 online at38.83
article
2014.found in the
www.jco.org. Author
Authors’ disclosures J ClinDo
of potential
Black
Oncol
began 3 months later. Understanding 0
notremains
know an important
33:1438-1445. © 2015 research
the complex
0 Society 0.0
priority.
by American
0.0mechanisms 1 whereby
of Clinical1Oncology0.97
advanced practice
0.97PC may improve survival Diagnosis
Lung 46 44.23 42
Other 172 1.92 183 2.91 .71
nurse.
contributions are found at theofend of are found inBrain metastasis at enrollment 16.35 17.48
42 40.38 33 32.04 conflicts interest the
GI tract 26 25 24
this article. article online at www.jco.org. AuthorMissing J Clin Oncol 33:1438-1445. © 2015 by American
0 as a result, Society of
0.0PC is offered
1 Clinical Oncology
0.97
20 19.23 27 trial information:
26.21 contributions are found at the end Charlson
of score 6.3 1.62 6.21 late,1.86if at all..71
2
Similarly,
Clinical NCT01245621. INTRODUCTION
Religion performance status delaying PC consultation .96 Breast 10 9.62 13
5 4.81 3
this article.
2.91Marie A. Bakitas, Karnofsky 80.58 10.87 81.46PCuntil
as a result,
patients.54
is 9.74
offered late,
are hospice2
if at all. Similarly,
Corresponding author:
CatholicSociety of Clinical
The American
Clinical trial information: NCT01245621. Oncology provi- 34 eligible32.69
INTRODUCTION or admitted 31PC 30.1 until
to the hospital for a medical Other solid tumor 10 9.62 10
ealth 72 69.23 DNSc, CRNP, School of Nursing/Depart-
70 67.96 .88 Anticancer treatment at enrollment delaying consultation
crisis3 prevents patients from receiving all of the
patients are hospice
Corresponding
ment of Medicine, University of author: Marie sional clinical
Protestant
A. Bakitas, opinion recommends that “combined
The American Society of Clinical Oncology 31 provi-29.81 eligible32or admitted 31.07 to the .52hospital Genitourinary
for a medical tract 7 6.73 9
t month 63 87.5 59 at Birmingham,
Alabama 84.29 DNSc, .47
CRNP,
1720 2ndSchool standard
Ave of Nursing/Depart- Chemotherapy
oncology care and palliative care (PC) 76 potential 73.08
benefits380that early PC 77.67has to offer. 4-6
Jewish crisis prevents patients from receiving all ofHematologic
the malignancy 5 4.81 5
be considered early in the course of illness for 201 0.96 0 PC provides 0.0
South, Birmingham, ment of Medicine, University of
AL 35294-1210; sional clinical opinion recommends that “combined
at Birmingham, 1720 2nd Radiotherapy standard oncology care and palliative care (PC)19.23 20 benefits19.42
that early1.00
Alabama1.00
shouldAve In contrast, early anticipatory
potential PC has to offer.4-6
e-mail: mbakitas@uab.edu.
None with metastatic cancer and/or high 23 guidance
anyInpatient 22.12 21 management
about symptom 20.39 and thought- Disease status at enrollment
25 24.04 24 23.3
South, Birmingham, AL 35294-1210;
a clinical trialbeat
should enrollment
considered early in the course19 of illness for18.27 In8contrast, 7.77 early PC.04 provides anticipatory
© 2015 by American Society of Clinical
e-mail: mbakitas@uab.edu. symptom burden.”1p880 A gap exists between this
Other any patient with metastatic cancer 13
and/or
ful discussions
high 12.5 on
guidanceadvanced
15 about care
14.56
symptom planning
managementand goals New diagnosis
and thought-
48 46.15 46
49 47.12
Oncology
50 48.54 Advance directive
recommendation and currentin medical
practice,
1p880 and there is of care that engage individuals to consider their val- and goals
© 2015 by American Society
0732-183X/15/3313w-1438w/$20.00
of Clinical
Missing symptom burden.” A gap exists 2
between this 1.92 ful 4
discussions on 3.88
advanced care planning Recurrence 29 27.88 20The finding of a 15% improvement in 1-year survival in patients
with advanced cancer of mixed diagnoses receiving early (v 3-
month delayed) PC is consistent with the improved survival noted
in Temel’s study in patients with non–small-cell lung cancer only
(11.6 v 8.9 months).
Early Versus Delayed Early Palliative Oncology Care
specifically tailored for patients
1.0 ting.4,7 Unlike our prior RCT com
Overall Survival (proportion) Early
Delayed
care, comparison group patient
0.8 3-month delay.15,16 This design
with usual care at 3 months. W
0.6 63% patient-reported outcomes; how
tage was noted in the early-entry
48%
0.4 Our finding of a 15% impro
with advanced cancer of mixed d
0.2
delayed) PC is consistent with th
et al6 in their early PC study in
cancer only (11.6 v 8.9 months;
0 3 6 9 12 suggest that concurrent PC prov
Time (months) survival benefit by a mechanism
No. at risk findings, together with improved
Early 104 98 83 62 48
Delayed 103 89 73 55 39
for the recommendation of early
metastatic disease and/or high sy
Fig 2. Kaplan-Meier estimates of 1-year survival by treatment group. Unlike that by Temel et al6
study did not demonstrate stat
QOL or mood related to early PCL’intervento precoce di supporto/cure
palliative: quali OBIETTIVI?
Miglioramento:
1. Controllo dei sintomi (dolore), della QoL
2. Dati suggestivi, seppur iniziali, della sopravvivenza
3. Depressione nei care givers
4. Ridefinizione degli obiettivi di cura (Comunicazione)
Riduzione:
5. Cure inappropriateL’intervento precoce di supporto/cure
palliative: quali OBIETTIVI?
Miglioramento:
1. Controllo dei sintomi, della QoL
2. Dati suggestivi, seppur iniziali, della sopravvivenza
3. Depressione nei care givers
4. Ridefinizione degli obiettivi di cura (Comunicazione)
Riduzione:
5. Cure inappropriateVOLUME 33 ! NUMBER 13 ! MAY 1 2015
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
Benefits of Early Versus Delayed Palliative Care to Informal
Family Caregivers of Patients With Advanced Cancer:
Outcomes From the ENABLE III Randomized
Controlled Trial
J. Nicholas Dionne-Odom, Andres Azuero, Kathleen D. Lyons, Jay G. Hull, Tor Tosteson, Zhigang Li,
Zhongze Li, Jennifer Frost, Konstantin H. Dragnev, Imatullah Akyar, Mark T. Hegel, and Marie A. Bakitas
See accompanying editorial on page 1420
Early-group: Care Givers had lower depression (6%
J. Nicholas Dionne-Odom, Andres
Azuero, Imatullah Akyar, and Marie A. A B S T R A C T
Bakitas, University of Alabama at
Birmingham, Birmingham, AL; Kathleen Purpose
decrease) and stress burden in the terminal
D. Lyons, Jay G. Hull, Zhigang Li, and
Mark T. Hegel, Dartmouth College; Tor
Tosteson and Zhongze Li, Norris Cotton
To determine the effect of early versus delayed initiation of a palliative care intervention for family
caregivers (CGs) of patients with advanced cancer.
analysis. Patients and Methods
Cancer Center, Hanover; and Jennifer
Frost and Konstantin H. Dragnev, Between October 2010 and March 2013, CGs of patients with advanced cancer were randomly
Dartmouth-Hitchcock Medical Center,
assigned to receive three structured weekly telephone coaching sessions, monthly follow-up, and
Lebanon, NH.
a bereavement call either early after enrollment or 3 months later. CGs of patients with advanced
Published online ahead of print at cancer were recruited from a National Cancer Institute cancer center, a Veterans Administration
www.jco.org on March 23, 2015.
Medical Center, and two community outreach clinics. Outcomes were quality of life (QOL),
Palliative care for Care Givers should be initiated as
Supported by Grant No.
R01NR011871-01 from the National
Institute for Nursing Research; by a
depression, and burden (objective, stress, and demand).
Results
early as possible to maximize benefits.
postdoctoral fellowship supported by
A total of 122 CGs (early, n ! 61; delayed, n ! 61) of 207 patients participated; average age was
University of Alabama at Birmingham
Cancer Prevention and Control Training
60 years, and most were female (78.7%) and white (92.6%). Between-group differences in
Program Grant No. 5R25CA047888 depression scores from enrollment to 3 months (before delayed group started intervention)
(J.N.D.-O.); an NIH/NINR Small favored the early group (mean difference, "3.4; SE, 1.5; d ! ".32; P ! .02). There were no
Research Grant 1R03NR014915-01 differences in QOL (mean difference, "2; SE, 2.3; d ! ".13; P ! .39) or burden (objective: mean
(Zhigang Li) and by Mentored Research difference, 0.3; SE, .7; d ! .09; P ! .64; stress: mean difference, ".5; SE, .5; d ! ".2; P ! .29;
Scholar Grant No. MRSG 12-113-01–
demand: mean difference, 0; SE, .7; d ! ".01; P ! .97). In decedents’ CGs, a terminal decline
CPPB in Applied and Clinical Research
from the American Cancer Society
analysis indicated between-group differences favoring the early group for depression (mean
(K.D.L.). difference, "3.8; SE, 1.5; d ! ".39; P ! .02) and stress burden (mean difference, "1.1; SE, .4;
d ! ".44; P ! .01) but not for QOL (mean difference, "4.9; SE, 2.6; d ! ".3; P ! .07), objective
Presented at the 50th Annual Meeting
of the American Society of Clinical
burden (mean difference, ".6; SE, .6; d ! ".18; P ! .27), or demand burden (mean difference,L’intervento precoce di supporto/cure
palliative: quali OBIETTIVI?
Miglioramento:
1. Controllo dei sintomi, della QoL
2. Dati suggestivi, seppur iniziali, della sopravvivenza
3. Depressione nei care givers
4. Ridefinizione degli obiettivi di cura (Comunicazione)
Riduzione:
5. Cure inappropriate69% of pa)ents with lung cancer and 81% of those with colorectal cancer did not report understanding that chemotherapy was not at all likely to cure their cancer.
JOURNAL OF PALLIATIVE MEDICINE
Volume 16, Number 8, 2013
ª Mary Ann Liebert, Inc.
DOI: 10.1089/jpm.2012.0547
The Cultivation of Prognostic Awareness Through the
Provision of Early Palliative Care in the Ambulatory Setting:
A Communication Guide
Vicki A. Jackson, MD, MPH,1 Juliet Jacobsen, MD,1,2 Joseph A. Greer, PhD,3 William F. Pirl, MD,3
Jennifer S. Temel, MD,3 and Anthony L. Back, MD 4
SPIKES AND NURSE COMMUNICATION ABILITIES
Abstract
Early, integrated palliative care delivered in the ambulatory setting has been associated with improved quality
of life, lower rates of depression, and even prolonged survival. We outline an expert practice that provides a
step-wiseVapproach
O L U M E 3 2to! cultivating
N U M B E R 3 prognostic
1 ! NOVEMB awareness
E R 1 2 0 1 4in patients cared for by a palliative care clinician early in
the course of the patient’s disease. This approach can be used by both novice and more experienced palliative
JOURNAL OF CLINICAL ONCOLOGY
care clinicians. COMMENTS AND CONTROVERSIES
Introduction Over the course of receiving care from a skilled palliative
care clinician, we have found that many of these patients seem
E arly, integrated palliative care delivered in the to develop an increased capacity to tolerate discussions about
ambulatory setting includes consultation and manage- prognosis and accept what this information means to them
Current State of the Art and Science of Patient-
ment throughout the entirety of the illness for patients with personally. Many of these patients develop the ability to hear,
advanced cancer. This approach has been associated with process, and draw on prognostic information to make medical
Clinician Communication in Progressive Disease:
improved quality of life, lower rates of depression, and, even, decisions that match their own values—and are grateful to the
prolonged survival.1,2 Many patients with cancer hold an in- clinician who worked with them to reach that point. In sum-
Patients’ Need to Know and Need to Feel Known
accurate view of the goals of treatment and their prognosis.3,4 mary, we observe patients gradually develop prognostic
These patients have a low ‘‘prognostic awareness.’’ We define awareness through an incremental cognitive and emotional
prognostic awareness as a patient’s capacity to understand his process that can be cultivated over time through interaction
or herLiesbeth M. and
prognosis van the
Vliet, King’s
likely College
illness London,
trajectory. Cicely Saunders
Improving a withInstitute,
a skilledLondon, United Kingdom
clinician.
Andrew S. Epstein, Memorial Sloan-Kettering
patient’s prognostic awareness is an important component of Cancer Center, New York, NY
We outline here an expert practice that provides a step-
early palliative care because a more accurate understanding of wise approach to cultivating prognostic awareness in pa-
prognosisEffective
is associated with earlier
communication rests atenrollment in hospice
the core of medicine, tients ficulty
especially cared21—forofby a palliative
linking care clinician
and responding to patients’early in the
cognitive and emo-
and lower
when rates
patientsof resuscitation
are confronted for
with patients with
progressive incurable
disease and course
death. of
tionalthe patient’s
needs disease.
simultaneously. We illustrate our approach
5,6
cancer. Palliative can
Communication caremitigate
clinicians can facilitate
the distress enhanced
of receiving bad news andwith a caseTothat unfolds
achieve this, over months.
we propose thatThis approach can
communication beshould
skills
prognostic awareness in patients with cancer through the use used by both novice and more experienced palliative care
influence patients’ psychological functioning and adaptation to a new be taught within a framework that entails approaches for both
of advanced communication
1-3 techniques.1 clinicians. It requires the clinician to assess the patient’s levelPotenza, Galli, Bandieri, Luppi et al. Journal of Pain and Symptom Management 2015
L’intervento precoce di supporto/cure
palliative: quali OBIETTIVI?
Miglioramento:
1. Controllo dei sintomi, della QoL
2. Dati suggestivi, seppur iniziali, della sopravvivenza
3. Depressione nei care givers
4. Ridefinizione degli obiettivi di cura (Comunicazione)
5. Cure inappropriate nel fine vitaOLUME Early introduction of supportive/palliative care also
33 ! NUMBER 13 ! MAY 1 2015
JOURNAL OF Cled to less aggressive end-of-life
LINICAL ONCOLOGY
care, reduced
O R I G I N A L R E P O R T
chemotherapy in the last 14 days (17.5%).
VOLUME 33 ! NUMBER 13 ! MAY 1 2015
JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T
Bakitas, J. Nicholas Dionne- Early Versus Delayed Initiation of Concurrent Palliative
d Andres Azuero, University
a at Birmingham, Birming- Oncology Care: Patient
Early Outcomes
Versus Delayed inofthe
Initiation
Marie A. Bakitas, J. Nicholas Dionne-
ENABLE
Concurrent III
Palliative
Oncology Care: Patient Outcomes in the ENABLE III
Odom, and Andres Azuero, University
Marie A. Bakitas, Jennifer
Konstantin H. Dragnev, Randomized Controlled Trial Trial
of Alabama at Birmingham, Birming-
Randomized Controlled
ham, AL; Marie A. Bakitas, Jennifer
Frost, and Konstantin H. Dragnev,
h-Hitchcock Medical Center; Dartmouth-Hitchcock Medical Center;
Marie A. Bakitas, Tor D. Tosteson, Zhigang Li, Kathleen D. Lyons, Jay G. Hull, Zhongze Li,
i, Norris Cotton Cancer
Marie A. Bakitas, Tor D. Tosteson,
Zhongze Li, Norris Cotton Cancer
Zhigang Li,
J. Nicholas Dionne-Odom,
Center, Lebanon; Tor D. Tosteson,
Kathleen
Jennifer D. Lyons,
Frost, Konstantin Jay G.
H. Dragnev, Hull,
Mark Zhongze
T. Hegel, Li,
Andres Azuero,
banon; Tor D. Tosteson, J. Nicholas Dionne-Odom, Jennifer Frost, Konstantin H. Dragnev, Mark T. Hegel, Andres Azuero,
and Tim A. Ahles
Kathleen D. Lyons, and Mark T. Hegel,
Geisel School of Medicine at Dart-
See accompanying editorial on page 1420
D. Lyons, and Mark T. Hegel, and Tim A. Ahles
mouth; Zhigang Li and Jay G. Hull,
Dartmouth College, Hanover, NH; and
hool of Medicine at Dart- Tim A. Ahles, Memorial Sloan-Kettering A B S T R A C T
igang Li and Jay G. Hull, Chemotherapy use in the last 14 days averaged 7%
See accompanying editorial
Purpose
on page 1420
Cancer Center, New York, NY.
Published online ahead of print at
Randomized controlled trials have supported integrated oncology and palliative care (PC);
h College, Hanover, NH; and www.jco.org on March 23, 2015.
however, optimal timing has not been evaluated. We investigated the effect of early versus
es, Memorial Sloan-Kettering
Supported by Grant No.
R01NR011871-01 from the National Insti-
A
delayed PC on quality Bof lifeS(QOL),T symptom
R Aimpact,
C mood,
T 1-year survival, and resource use.
nter, New York, NY. tute for Nursing Research; by a Cancer Patients and Methods
and Leukemia Group B Foundation Clini- Between October 2010 and March 2013, 207 patients with advanced cancer at a National
online ahead of print at
Purpose
cal Scholar Award; by the Foundation for
Cancer Institute cancer center, a Veterans Affairs Medical Center, and community outreach
Randomized controlled trials have supported integrated oncology and palliative care (PC);
Informed Medical Decision-Making; by
Grants No. P30CA023108, UL1
clinics were randomly assigned to receive an in-person PC consultation, structured PC
org on March 23, 2015. telehealth nurse coaching sessions (once per week for six sessions), and monthly follow-up
however, optimal timing has not been evaluated. We investigated the effect of early versus
TR001086, and R03NR014915; an
NIH/NINR Small Research Grant either early after enrollment or 3 months later. Outcomes were QOL, symptom impact, mood,
by Grant No. 1R03NR014915-01 (Zhigang Li); by Norris 1-year survival, and resource use (hospital/intensive care unit days, emergency room visits,FORMAZIONE: ruolo centrale
The University of Michigan reduced
chemotherapy use from 50% to about 20% in
the pa)ent’s last 2 weeks of life by simply
ini)a)ng of educa)on in pallia)ve care
Trends in chemotherapy administered in the last
2 weeks of life for all studied pa>ents.
Blayney et al., J Clin Oncol 2009of print at
JOURNAL OF
The
C guideline update reflects
LINICAL ONCOLOGY
changesSinPevidence
A S C O
since
E C I A L
the previous guideline. Nine RC
A R T I C L E
er 31, 2016.
quasiexperimental trial, and five secondary analyses from RCTs in the 2012 PCO on p
ne Committee palliative care
JOURNAL services
OF CLINICAL Oto patients with
NCOLOGY A S Ccancer
O S P Eand/or
C I A L their caregivers,
A R T I C L E including fam
016.
givers, were found to inform the update.
rican Society of
al practice Recommendations
Integration of Palliative Care Into Standard Oncology Care:
Inpatients
American and outpatients
Society of with Clinical advanced
Oncology cancer should receive dedicated palliative care s
mmendations,
Integration of Palliative Care IntoClinical Standard Practice Oncology Care:
view and analyses early in the disease
Guideline Updatecourse, concurrent
American Society of Clinical with activeOncology treatment.
Clinical Referral
Practice of patients to interdis
eR.for each City of Hope Medical palliative careJennifer
teams is optimal, Temin, andErin R.services
Alesi, Tracy A.may complement existing
I. Firn, programs. Provid
er,
Ferrell,
ional information,
Duarte, CA; Jennifer S. Temel and
Betty R. Ferrell, Guideline
S. Temel, SarahUpdate Balboni, Ethan M. Basch, Janice
Judith A. Paice, Jeffrey M. Peppercorn, Tanyanika Phillips, Ellen L. Stovall,† Camilla Zimmermann, and
ey M. Peppercorn, Massachusetts refer family and friend Betty R.caregivers of Sarah
Ferrell, Jennifer S. Temel,
Betty R. Ferrell, City of Hope Medical patients
Temin, Erinwith early
R. Alesi, Tracy or advanced
A. Balboni, cancer
Ethan M. Basch, Janice I. Firn, to palliative care s
Thomas J. Smith
ment with
ral Hospital; Tracy A. Balboni, Center, Duarte, CA; Jennifer S. Temel and Judith A. Paice, Jeffrey M. Peppercorn, Tanyanika Phillips, Ellen L. Stovall,† Camilla Zimmermann, and
Farber Cancer Institute, Boston, MA; Jeffrey M. Peppercorn, Massachusetts Thomas J. Smith
es, a Methodology General Hospital; Tracy A. Balboni,
JSarahClin Oncol 34. © 2016 by American Society of Clinical Oncology
Temin, American Society of Clinical
Dana-Farber Cancer Institute, Boston, MA; A B S T R A C T
clinical tools and
logy, Alexandria; Erin R. Alesi,
Temin, American Society of Clinical
ia Commonwealth University Health Oncology, Alexandria; Erin R. Alesi,
A B S T R A C T
atient information
m, Richmond, VA; Ethan M. Basch, Purpose
Virginia Commonwealth University Health
ersity of North Carolina at Chapel Hill, System,To provide
Richmond, VA; Ethanevidence-based
M. Basch, Purpose recommendations to oncology clinicians, patients, family and friend
available at www. To provide evidence-based recommendations
the 2012toAmerican
oncology clinicians, patients, family and friend 3
caregivers,
el Hill, NC; Janice I. Firn, University of University of North Carolina atandChapel palliative
Hill, care specialists to update from
Society the National
of Clinical Consensus
Oncology Project (pro
guideline and Ann Arbor, MI;
gan Health System, Chapel
(ASCO) provisionalINTRODUCTION
Hill, NC; Janice I. Firn, University of caregivers, and palliative care specialists to update the 2012 American Society
clinical opinion (PCO) on the integration of palliative care into standard oncology of Clinical Oncology
h A. Paice, Northwestern University, Michigan Health
care
System, Ann
for all patients
Arbor, MI;
diagnosed with cancer. Bottom Line Box). Patients with advance
(ASCO) provisional clinical opinion (PCO) on the integration of palliative care into standard oncology
eswiki.
Key Recommendation
Judith A. Paice, Northwestern University,
ston, IL; Tanyanika Phillips, care for all patients diagnosed with cancer.
Evanston, IL; Tanyanika Phillips,
STUS St Frances Cabrini Hospital, Methods
CHRISTUS St Frances Cabrini Hospital, Methods are defined as those with distant metastases,
potential conflicts
ndria, LA; Ellen L. Stovall, National ASCO convened an Expert Panel ofanmembers
ASCO convened
Alexandria, LA; Ellen L. Stovall, National ofofthe
Expert Panel ASCO
members ofAd
the Hoc
ASCOPalliative Care Expert
Ad Hoc Palliative Panel
Care Expert toto
Panel
at KimmelThe purpose of this version of2012the was based on a review ofdisease,
PCO American cancertrialthat is life limiting, and
ion for Cancer Survivorship, Silver
he articleJ. online develop an update. The 2012
Coalition for Cancer Survivorship, Silver
develop PCO was
an update. The based on a review of a randomized controlled trial
a randomized controlled (RCT) by
(RCT) by
g; Thomas Smith, Sidney Spring; Thomas J. Smith, Sidney Kimmel
prehensive Cancer Center, Johns the National Cancer Institute Physicians
the National DataPhysicians
Cancer Institute Query and Dataadditional trials. The
Query and additional panel
trials. conducted
The panel conducted anan
ins University, Baltimore, MD; and Society University,of Clinical Oncologyseeking(ASCO) guideline prognosis of 6andtoandmeta-
24 months. This update
Comprehensive Cancer Center, Johns
ontributions are Hopkinsupdated systematic review
updated systematic randomized
review seeking clinical trials,
randomized systematic
clinical trials, reviews,
systematic reviews, meta-
Patients with advanced cancer,
clinical should nine RCTs,receive
Baltimore, MD; and
slaarticle.
Zimmermann, Princess Margaret Camilla analyses, analyses, as analyses
as well as secondary
Zimmermann, Princess Margaret well as secondary analyses
of RCTs in theof 2012
RCTs inPCO,
the 2012 PCO, published
published from from
MarchMarch
20102010
toto
er Centre, Toronto, Ontario, Canada. is toJanuary
update the 2012 ASCO
Cancer Centre, Toronto, Ontario, Canada.
2016. provisional
January 2016. as well as one quasiexperimen
Mill Rd, Suite 800,
dedicated supportive/palliative
1
care services, early in
†Deceased.
eased.
opinion
Results (PCO) on the integration of palliative
Published online ahead of print at
Results
and five secondary publications from pr
The guideline update reflects changes in evidence since the previous guideline. Nine RCTs, one
-mail:
shed guidelines@
online ahead of print at The guideline update reflects changes in evidence since the previous guideline. Nine RCTs, one
www.jco.org on October 31, 2016.
carequasiexperimental
into standardtrial, oncology care and from RCTs inreviewed
transition RCTs. It reviews and analyzes
quasiexperimental trial, and five secondary analyses from RCTs in the 2012 PCO on providing
.jco.org on October 31, 2016.
al Practice Guideline Committee the disease course,
Clinical Practice Guideline Committee
palliative care services
approved: August 15, 2016.
concurrent
and five secondary
to patients
analyses
with
with cancer and/or
the content into a guideline. The 2012 PCO was
active
their caregivers, treatment.
the 2012 PCO
including
on providing
palliative care services to patients with cancer and/or their caregivers, including family care-
family care-
updated evidence on early palliative care, i
givers, were found to inform the update.
ved: August 15, 2016.
American Society givers, were found to
Editor’s note: This American Society of inform the update.
Recommendations
r’s note: This American Society of
18
al Mill Rd,
Oncology clinical practice
based on a review of the 2010 study by Temel
Clinical Oncology clinical practice
Recommendations
guideline provides recommendations, evidence on patients in both inpatient a
Inpatients and outpatients with advanced cancer should receive dedicated palliative care services,
Inpatients and early inwith
outpatients the disease course,cancer
advanced concurrent with active
should treatment.
receive Referral
dedicated of patientscare
palliative to interdisciplinary
services,
For
et al newly diagnosed patients with advanced cancer,
2
with comprehensive review and analyses
line provides recommendations,
VA 22314; review and analyses
comprehensive
conducted by the National
of the relevant literature for each
early in the disease
recommendation. Additional information,
Cancer Institute
palliative
course, care teams is
concurrent optimal,
with activepatient settings,
andtreatment.
services mayReferral
complement
of components of and trig
existing programs.
patients to Providers may
interdisciplinary
palliative care refer family and friend caregivers of patients with early or advanced cancer to palliative care services.
with teams is optimal, and services may complement existing programs. Providers may
o.org.
e relevant literature for each
Physicians Data Query and additional randomized
including a Data Supplement
offering patients palliative care, palliat
mmendation. Additional information,
ding a Data Supplement with
ociety of Clinical
the Expert
refer
additional evidence
Panel
family
suggests
and friendJcaregivers
tables, a Methodology
controlled trials (RCTs) chosen by ASCO, showing
Supplement, slide sets, clinical tools and
onal evidence tables, a Methodology resources, and links to patient information
Clin Oncol 34. early
of patients
© 2016 bywith palliative
earlySociety
American or advanced
services
cancer
of Clinical
for family care
to palliative care services.
Oncology
caregivers, and how o
ement, slide sets, clinical tools and
rces, and links to patient information
ww.cancer.net, is available at www.
involvement
the benefits of early within 8INTRODUCTION
palliative
asco.org/palliative-care-guideline and
www.asco.org/guidelineswiki.
weeks
care when of diagnosis.
J Clin Oncol 34. © 2016 by American Society of Clinical Oncology
at www.cancer.net, is available at www.
addedfrom the National Consensus Project (provided in
professionals and other clinicians can
Bottom Line Box). Patients with advanced cancer
3
3
from the National Consensus
as those withProject (provided in
20.00
org/palliative-care-guideline and to usual oncology care.
INTRODUCTION As
Authors’ disclosures of potential conflicts in the 2012 PCO, this
Bottom Line
The purpose of this version of the American
of interest are found in the article online at
are definedpalliative
Box).cancer
disease, Patients
distantcare,
that with
metastases,
advanced
is life limiting,
inwith addition to palliat
late-stage
cancer
and/or
.asco.org/guidelineswiki.
6.70.1474 document uses theSociety definition
www.jco.org. Author contributions are
ors’ disclosures of potential conflicts found at the end of this article. of palliative
of Clinical Oncology (ASCO) are
guidelinecare
defined
is to update the 2012 ASCO provisional clinical
prognosis
as specialists.
of 6 to
those with 24 months.
distant Inupdate
This
metastases, this guideline, a family c
includes
late-stage
nine RCTs, as well as one quasiexperimental study
erest are found in the article online at The purpose of this version of the American disease, cancer that is life limiting, and/or with“Chiunque soffre cerca di
comunicare la sua
sofferenza; e solo così
facendo, la diminuisce
veramente.
Coloro che soffrono non
hanno, in fondo, bisogno
d'altro, che di uomini capaci di
prestar loro attenzione.
Ma la capacità di dare
attenzione a chi soffre è cosa
rarissima; quasi un miracolo.”
L'ombra e la grazia- 1943
Simone Weil
:Puoi anche leggere