Silvio Monfardini Programma Oncologia Geriatrica Istituto Palazzolo,Fondazione Don Gnocchi,Milano - Italia Longeva
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

IL PAZIENTE ONCOLOGICO E I “LONG SURVIVORS”: BISOGNI
INEVASI PER UNA CORRETTA PRESA IN CARICO
Silvio Monfardini
Programma Oncologia Geriatrica
Istituto Palazzolo,Fondazione Don
Gnocchi,Milano
LONG-TERM CARE THREE
Stati Generali dell’Assistenza a lungo termine
Roma, 11 e 12 luglio 2018 Ministero della Salute
Disclosure
Session Chairman at a Meeting sponsored by Cellgene
Giotto. Evil exorcism in Arezzo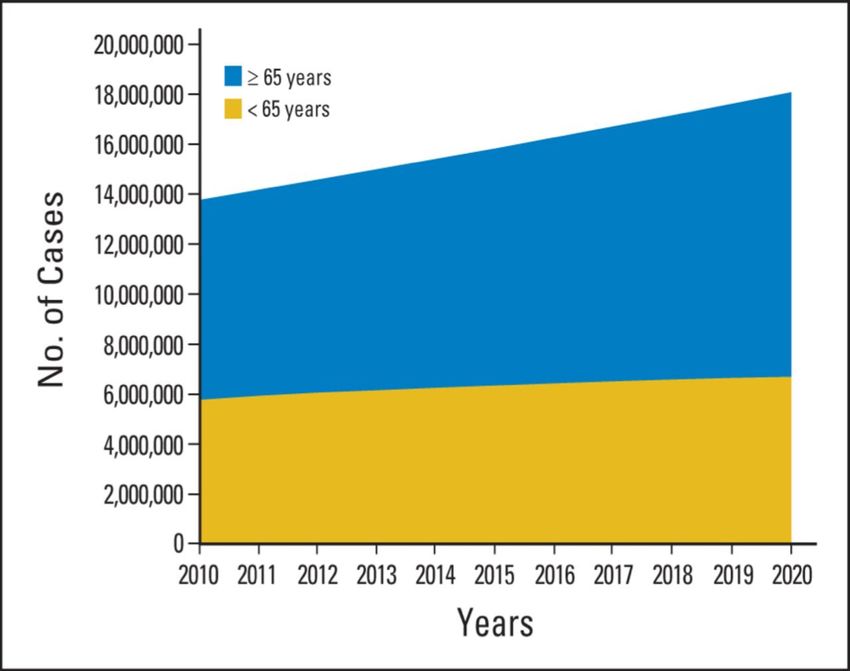
Quanti sono gli italiani che vivono
dopo una diagnosi di tumore?
*Nel 2017, oltre 3 milioni e
trecentomila (3.304.648) gli italiani
che vivono dopo
una diagnosi di tumore ( 5,4% della
popolazione italiana ,1/19 italiani)
*I NUMERI DEL CANCRO IN ITALIA 2017 AIOM-AIRTUM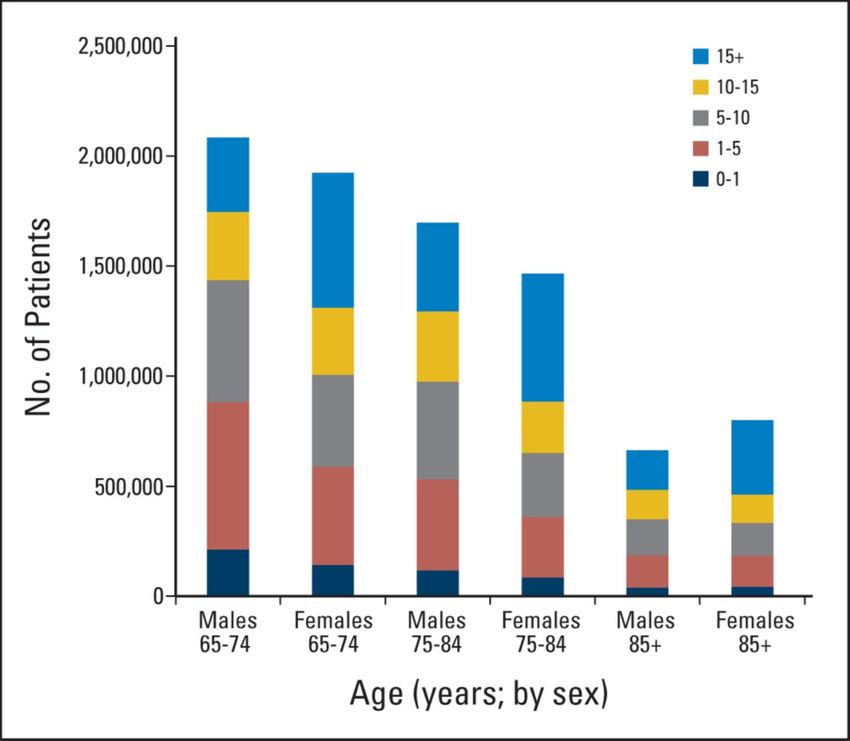
Survivorship by Age
• Survivorship includes not just patients in
remission but where cancer is a chronic disease
46% of cancer
survivors are 70
years and older
Survivorship includes not just patients in remission but where cancer is a chronic disease
Estimated number of persons with a history of cancer from 1971 to 2008, by age group, projected through to the year 2030. 2014 prevalence by age, sex, and duration among cancer survivors age ≥ 65 years Rowland J. H., and Bellizzi K. M. JCO 2014; 32:2662-2668 ©2014 by American Society of Clinical Oncology

How to improve survivors' physical
and psychological outcome?
1)Focus on screening for physical impairments (from
mild to severe) as they need to be identified and treated
2)refer cancer survivors who have problems amenable
to rehabilitation interventions to the appropriate health
care
From Giuseppe Colloca 2018,Treviso advanced
course of Geriatric Oncology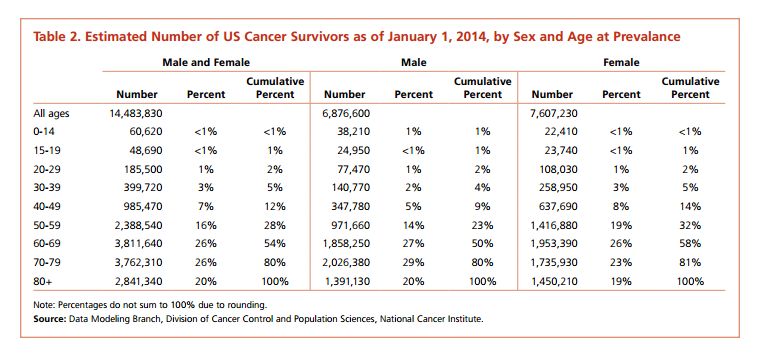
Common amenable Impairments General Physical Impairments •Difficulty returning to premorbid activities •Joint pain, diffuse (e.g., arthralgias) •Musculoskeletal pain (e.g., myalgias) •Neuropathic pain •Somatic pain •Visceral pain •Weakness •Fatigue •Deconditioning And Specific (organ or treatment related in each neoplasia)Physical Impairments
What is then Cancer Rehabilitation?
“medical care that should be integrated throughout the oncology care
continuum and delivered by trained rehabilitation professionals
to diagnose and treat patients’ physical, psychological and cognitive impairments
to maintain or restore function,in a multidisciplinary approach reduce symptom
burden, maximize independence and improve quality of life
From Giuseppe Colloca 2018,Treviso advanced course of Geriatric
OncologyArco temporale di attuazione della
riabilitazione in oncologia
“La riabilitazione deve occuparsi del paziente oncologico per
tutto
l’iter della malattia, dalla diagnosi all’intero percorso
terapeutico, fino alla fase
ultima della vita “
Progetto finanziato dal Ministero Salute -Riabilitazione in oncologia-: dalla
diagnosi alle cure palliative,2006. Istituto Nazionale TumoriMilano-FAVO
M.P. Schieroni, M.R. Strada, P. Varese in
Libro Bianco sulla
riabilitazione
oncologicaLa Riabilitazione Oncologica non è
purtroppo stata inclusa nei Lea
“la riabilitazione oncologica continuerà a essere inclusa in modo frammentato
all’interno di diverse tipologie riabilitative riferite ad altri gruppi di patologie
Si tratta di una soluzione inaccettabile che condanna il paziente a un percorso
riabilitativo discontinuo, frammentato, ma soprattutto parziale,
perché focalizzato esclusivamente sul recupero della funzione fisica lesa dalla
malattia e non
sul completo recupero cognitivo, psicologico, sessuale, nutrizionale e sociale
FAVO .Quotidiano Sanita’ 2016Ministero della salute Quaderno
n. 8 del 2011
“La centralità della Persona in riabilitazione: nuovi
modelli organizzativi e gestionali”
“un’efficace terapia antitumorale non può prescindere
da una precoce presa in carico riabilitativa globale che
prevede una completa integrazione con chi si occupa
del piano terapeutico strettamente oncologico e
chi si occupa della terapia di supporto e delle cure di
sostegno”Rehabilitation in older cancer
patients
The rehabilitative program should be tailored to
single-out elderly patients after an attentive
evaluation of their needs and the assessment of
clinical(impairments for each type of cancer and
comorbidities), psychological and social conditions
through a Comprehensive Geriatric Assessment
E Morello,G Giordano,C Falci,S Monfardini. Aging Health
2009Unmet needs of old cancer survivors
● In elderly cancer survivors an assessment of persistent
and coexisting health problems should be carried out
● In this field issues are still open concerning delivering
optimal post-treatment care
● Dialogue between oncology and geriatric specialists
other than cross-training of clinical researchers
should be encouraged
Rowland J. and Bellizzi K., J ClinOncol.20142014Follow-up of elderly patients with urogenital
cancers: Evaluation of geriatric care needs and
related actions (Supported by the Italian Ministry of Health (RF -2009-
1502045 )
(Comparison of a modeled geriatric management to usual care in elderly patients
firstly treated urogenital neoplasms )
S.Monfardini1, S.Morlino2, R.Valdagni2, M.Catanzaro3, A.Tafa4,
B.Bortolato5, G.Petralia6, E.Bonetto7, E.Villa8, S.Picozzi9, M.C. Locatelli10,
G.Galetti1, E.Bianchi
S.Monfardini
11,A.Millul
1, S.Morlino 11, Y.Albanese
2, R.Valdagni 11, C.Panzarino
2, M.Catanzaro 3, A.Tafa41,,B.Bortolato
F.Gerardi1 5,
and E.Beghi
G.Petralia
11
6, E.Bonetto 7, E.Villa8, S.Picozzi9, M.C. Locatelli10, G.Galetti1,
E.Bianchi11,A.Millul11, Y.Albanese11, C.Panzarino1, F.Gerardi1 and E.Beghi11
Journal of Geriatric Oncology,2017Results CGA was performed in 459 pts, >70 years Prostate cancer : 291 pts (median age 75 y) Bladder cancer :126 (median age 77 y) Kidney cancer :37 (median age 77 y).
Clinical care patterns • Home & follow-up • Integrated home assistance • Home & caregiver for rehabilitation • Home & general • Geriatric rehabilitation practitioner • General & focused • Integrated home assistance rehabilitation • Specialist consultation • Nursing home
Distribution of Fit,Frail,Vulnerable Pts •prostate ca:40% Fit, 47% Vulner, 13% Frail. • bladder ca: 21% Fit, 42% Vulner, 37% Frail. •renal ca: 22% Fit, 43% Vulner, 35% Frail.
Conclusions of this Study •Vulnerable and Frail were over 75% of both renal and bladder cancer pts, and 60% of prostate cancer pts. •During the follow up only a minority of pts was seen by a specialist in case of severe comorbidities. Only few pts with functional deficits received rehabilitation. •A Geriatric consultation was almost unexistent.
An integrated approach also during
the follow up has to be considered
The U13 conference series of Cancer and Aging Research Group
NCI,NIA and the Alliance Clinical Trials in Oncology (2010-2014):
Areas of highest research priorities in Geriatric Oncology
The 3rdrd U13 Conference in 2016
focused on improving the quality of life
and survivorship of older and frail
adults with cancer(S.G. Mohile et al,
Cancer 2016)We need this Orchestra also for older cancer
survivors
Epidemiology.
Clinical Oncol. Clinical and
(Surgical, Laboratory Geriatrics,
Medical Research Gerontology
Oncology, RT)
GERIATRIC
Rehabilitation, ONCOLOGY
pharmacy, Palliative care
nutrition, Supportive therapy
social services
Primary care
Clinical Oncologists, Geriatricians and other partnersHow difficult is it to
transfer such specific
approach in the real
world throughout the
entire Patient’s Disease
Trajectory?
Bosch, Hieronymus the Ship of FoolsWe need to develope dedicated Geriatric Oncology
Programmes (GOP)
• A comprehensive care through a multidisciplinary approach (age-associated
conditions and cancer management) should be provided
• These programmes should take care of the initial diagnostic and therapeutic
approach
• But also provide Survivorship assistance through the management of
General and Specific Physical Impairments related to cancer and its treatment
as well as of the geriatric-related conditions,
during all the disease trajectory
• S Monfardini et al: Report of a SIOG task force.Crit Rev Oncol/Hematol,2006CONCLUSIONI • I pazienti oncologici anziani sono la maggior parte dei 3 milioni di italiani che vivono dopo una diagnosi di tumore ed il loro numero è in aumento • Le menomazioni legate al cancro ed alla terapia oncologica,come anche quelle connesse alla eta’dovrebbero essere oggetto della Riabilitazione Oncologica e di quella Geriatrica durante tutto l’arco della malattia( dalla fase iniziale a quella della malattia avanzata) • E’ necessario pensare per il futuro ad una Valutazione Geriatrica Multidimensionale ed un approccio integrato (Oncologo,Geriatra,Fisiatra,Psicologo,Medico di Medicina Generale,ecc) • Ad oggi molte di queste necessita’ sono inevase ,la prima sfida e’ di ordine culturale:occorre pensare anche per gli Oncologi che il processo di geriatrizzazione della Medicina richiede nuovi tipi di organizzazione :Programmi di Oncologia Geriatrica
Puoi anche leggere