Systemic treatment approach: the new standard of care for advanced CSCC - Paolo Bossi - Carcinoma Squamoso Cutaneo
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

Systemic treatment approach: the new standard of care for advanced CSCC Paolo Bossi MAT-IT-2001175
Disclosure of interests Participation in advisory board or conference honoraria: Merck, Sanofi-Regeneron, Merck Sharp & Dohme, Sun Pharma, Angelini, AstraZeneca, Bristol-Myers Squibb, Helsinn, GSK
Cosa porta a definire «advanced» il cSCC? MALATTIA PAZIENTE TERAPIA Stadio T, N (M) Fragile, Anziano Radicalità chirurgia? RT fattibile? Tipologia Immunodepresso Ricostruzione? infiltrazione (trapianto, patologia reumatologica…) Linfangite – lesioni Comorbidità Disfigurement? multiple
Avanzato perchè….. AVANZATO PERCHÉ OLTRE I LIMITI DEL T → Diffusione linfonodale, cutanea, metastatica AVANZATO PERCHÉ NON HO SCELTE RADIOTERAPICHE → Patologie concomitanti → Pz già irradiato AVANZATO PER INTERVENTO «INVASIVO» → Amputazione → Exenteratio orbitae AVANZATO PERCHÉ LA CHIRURGIA NON MI RENDE CONFIDENTE IN UNA CURA DEFINITIVA: → Non margini negativi → Ennesima recidiva a chirurgia → Linfangite AVANZATO PERCHÉ IL PAZIENTE NON TOLLERA CHIRURGIA → Comorbidità → Età → Preferenze del paziente
Real life: come arrivano ad essere «advanced» ?
Caratteristiche e storia naturale dell’ «advanced cSCC» ➢60% Pz con comorbidità cardiovascolari; 22% cognitive ➢ Un terzo dei Pz in prima diagnosi è Advanced cSCC ➢ 62% dei report patologici è incompleto ➢ 37%-50% trattato in modo subottimale
Quali risposte sinora ottenute? EGFR INHIBITORS Erlotinib ORR: 10%1 CHEMOTHERAPY Platinum-based: 34% ORR6 Gefitinib ORR: 16%2 Cetuximab ORR: 21%3 Dacomitinib ORR: 28%4 Panitumumab ORR: 31%5 1. Gold KA, et al. Cancer. 2018 May 15; 124(10):2169-2173; 2. William WN Jr., et al. J Am Acad Dermatol. 2017 Dec;77(6):1110-1113.e2; 3. Dereure O, et al. Dermatology. 2016;232(6):721-730; 4. Cavalieri S, et al. Eur J Cancer 2018 Jul;97:7-15 5. Foote MC, et al. Ann Oncol. 2014 Oct;25(10):2047-52; 6. Fitzgerald K, et al. Semin Cutan Med Surg. 2019 Mar 1;38(1):E67-E74.
Ruolo dell’Immunoterapia nel cSCC SETTING UTILITA’ UTILITY RADIOSENSIBILIZZANTE, Possible, extrapolated by STUDI IN CORSO FASE POSTOPERATORIA head and neck cancer ADIUVANTE Uncertain STUDI IN CORSO PALLIATIVO Possible, ALTA RESPONSE to improveRATE QoL E and DORsurvival (?)
Possiamo ancora definire «terapia palliativa»? ➢ Palliazione intesa come miglioramento (o stabilizzazione) dei sintomi ➢ Miglioramento (o non peggioramento) della qualità di vita L’immunoterapia risponde a queste caratteristiche nel cSCC?
I dati degli studi Migden MR et al. New Engl J Med 2018
EMPOWER-CSCC-1: il disegno dello studio Key inclusion criteria • ECOG performance status of 0 or 1 • Groups 1 & 3: At least one lesion measurable by RECIST 1.1 • Group 2: oAt least one lesion measurable lesion by RECIST 1.1 criteria (for scans) or modified WHO criteria (for photos) oCSCC lesion that is not amenable to surgery or radiotherapy per investigator assessment Key exclusion criteria • Ongoing or recent (within 5 years) autoimmune disease requiring systemic immunosuppression • Prior anti–PD-1 or anti–PD-L1 therapy • History of solid organ transplant, concurrent malignancies (unless indolent or not considered life threatening; for example, basal cell carcinoma), or haematologic malignancies
EMPOWER-CSCC-1: il disegno dello studio Group 1 – Adult patients with Cemiplimab 3 mg/kg metastatic (nodal and/or distant) CSCC Q2W IV, for up to Tumour imaging 96 weeks Q8W for the (retreatment optional assessment of for patients with efficacy Group 2 – Adult patients with disease progression locally advanced CSCC during follow-up) Tumour imaging Cemiplimab 350 mg Group 3 – Adult patients with Q9W for the Q3W IV, for up to 54 metastatic (nodal and/or distant) CSCC assessment of weeks efficacy Tumour response assessment by ICR (RECIST 1.1 for scans; modified WHO criteria for photos)
EMPOWER-CSCC-1: caratteristiche basali Metastatic CSCC Locally advanced Overall (n=59) CSCC (n=78) (N=137) Median age, years (range) 71 (38–93) 74 (45–96) 72 (38–96) ≥ 65 years, n (%) 43 (72.9) 59 (75.6) 102 (74.5) Male, n (%) 54 (91.5) 59 (75.6) 113 (82.5) ECOG performance status, n (%) 0 23 (39.0) 38 (48.7) 61 (44.5) 1 36 (61.0) 40 (51.3) 76 (55.5) Primary CSCC site, n (%) Head/neck 38 (64.4) 62 (79.5) 100 (73.0) Extremity 12 (20.3) 14 (17.9) 26 (19.0) Trunk 9 (15.3) 2 (2.6) 11 (8.0) Prior cancer-related systemic therapy, n (%) Any 33 (55.9) 12 (15.4) 45 (32.8) 1 22 (37.3) 10 (12.8) 32 (23.4) ≥2 11 (18.6) 2 (2.6) 13 (9.5) Prior cancer-related radiotherapy, n 50 (84.7) 43 (55.1) 93 (67.9) (%) Prior cancer-related surgery, n (%) 58 (98.3) 66 (84.6) 124 (90.5)
Risposta di malattia
Longer follow up : risposte complete aumentano Time to Response 13% >6 months 9% 46% 4-6 months 0-2 months 32% 2-4 months 16 Median time to complete response: 11.2 mesi! Rischin et al 2020 ASCO 2020 Poster 367
Caratteristiche della risposta: malattia locoregionale
Caratteristiche della risposta: malattia metastatica
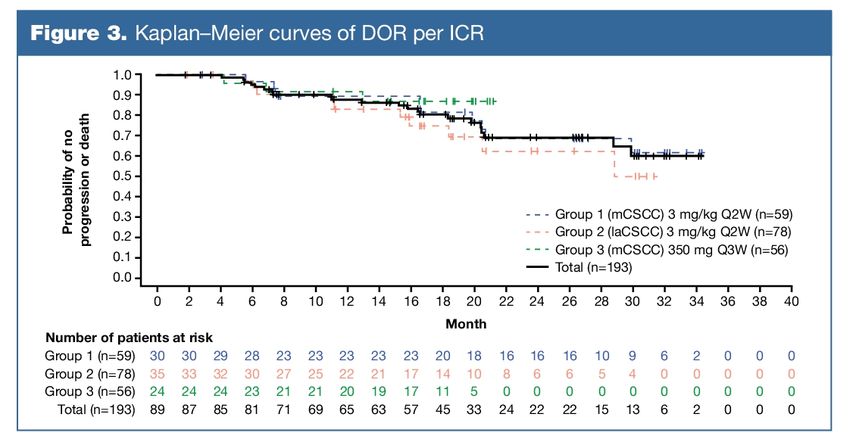
Durata media delle risposte Median Duration of Response = not reached!
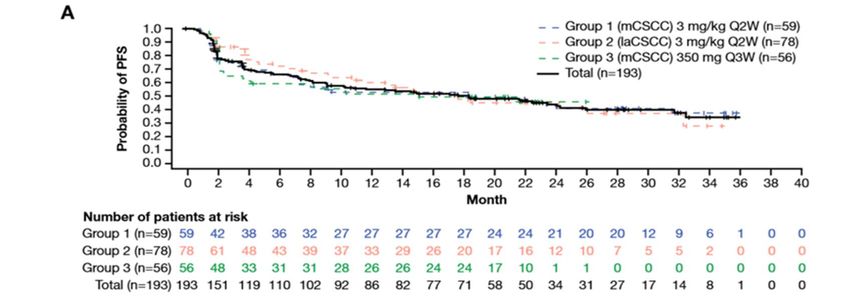
PFS
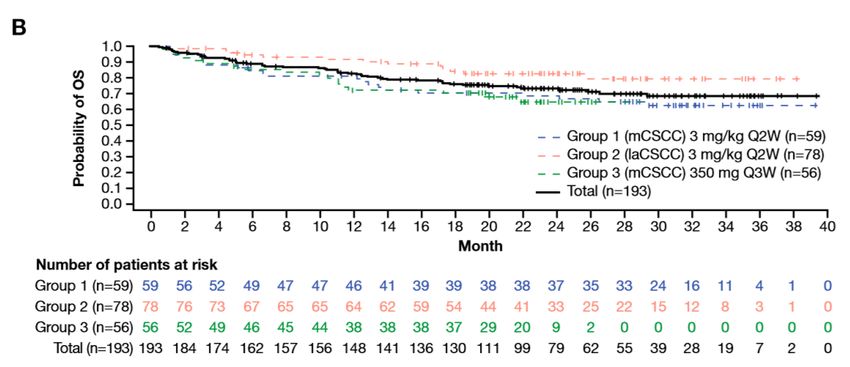
OS
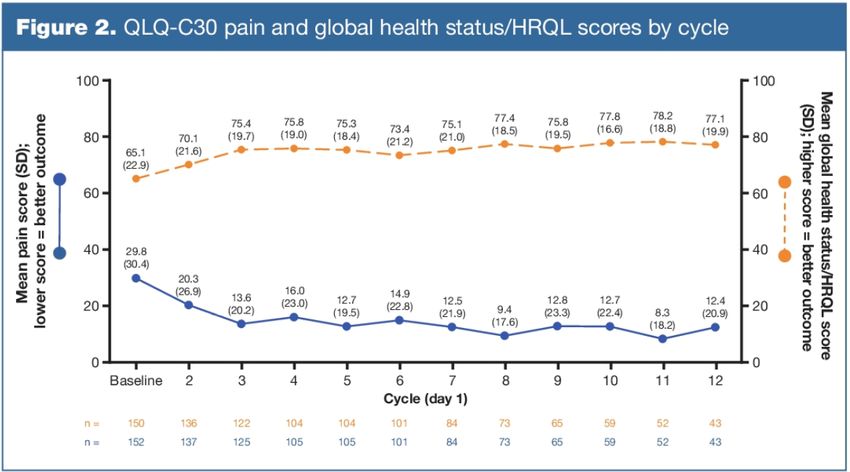
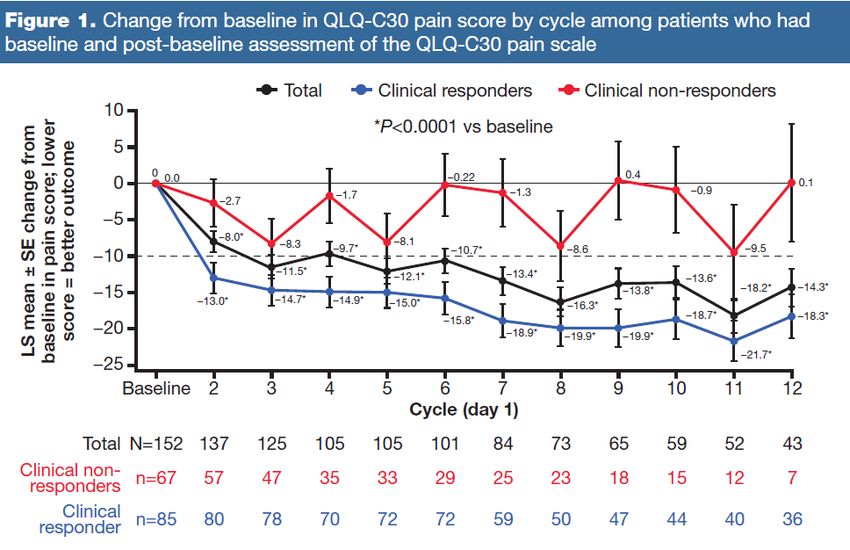
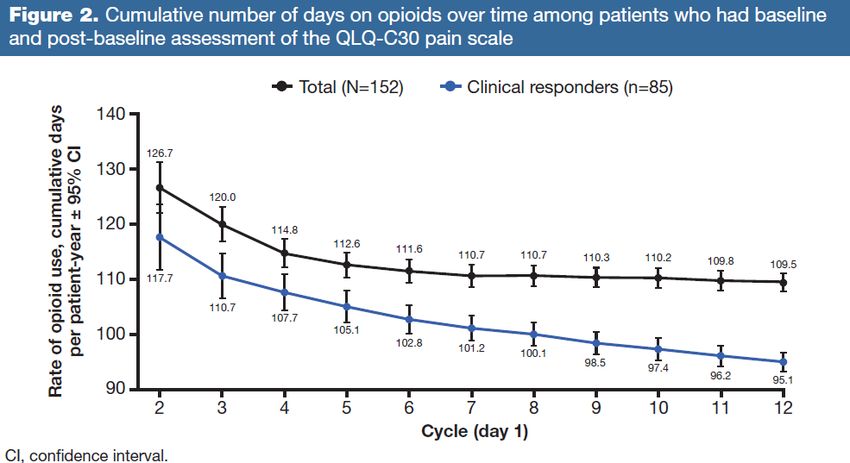
Impatto su Qualità di Vita Migden MR, ASCO 2020
Focus sul dolore… Parallel analysis: survival time according to Time to meaningful pain response Time to clinical response Migden et al Poster 1087 ESMO 2020
Focus sul dolore…
Possiamo ancora definire «terapia palliativa»? ➢ Miglioramento di sintomi ➢ Miglioramento della qualità di vita ➢ Lunghe risposte di malattia che si traducono in sopravvivenze lunghe … stiamo alzando l’asticella, almeno in un sottogruppo di pazienti, in cui questa terapia rappresenta una cura della malattia ➢ Il termine «palliazione» diventa improprio!
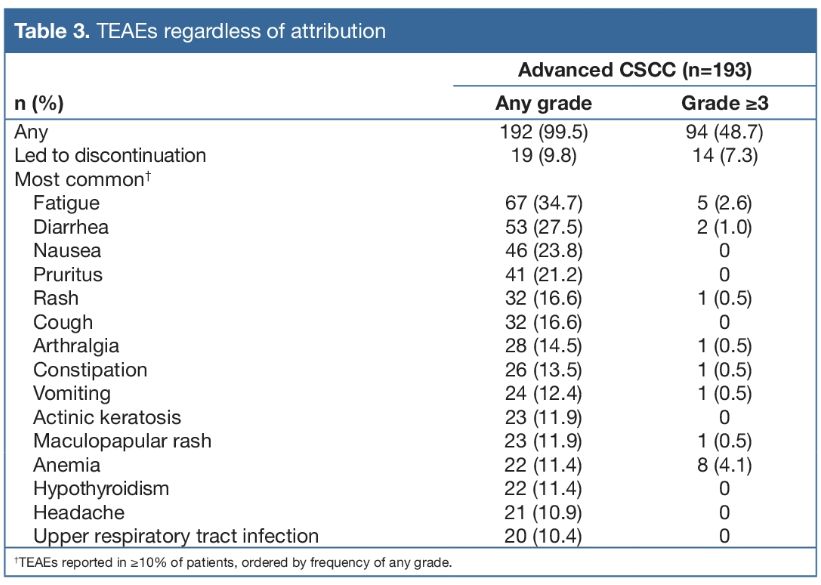
Suggerimenti utili • Possibile flare infiammatorio dopo prime somministrazioni • Dose flat feasible (PK data: peso non impatta su concentrazione) • Circa 15% dei Pz ha una progressione come best response • Numero di chirurgie precedenti impatta su risposta
Precedenti terapie e risposte
Marcatori predittivi di risposta? • PDL1 potenziale predittività di risposta? • Altri marcatori? TMB?
Marcatori predittivi di risposta?
Studi in corso NEOADJUVANT ADJUVANT PHASE III TRIALS COMBINATION APPROACHES • Cemiplimab1 • Cemiplimab • Pembrolizumab + Radiation • Pembrolizumab (KEYNOTE-630) • Avelumab + Radiation • Pembrolizumab + Cetuximab • Avelumab ± Cetuximab in advanced disease • Cemiplimab + RP1 oncolytic virus INTRALESIONAL THERAPY ONGOING SINGLE AGENT, TX NAIVE • TVEC • Cemiplimab • Nivolumab (EMPOWER-CSCC-1)
ZONE GRIGIE DELL’IMMUNOTERAPIA nel cSCC ➢ Trattamento dei pazienti immunosoppressi, trapiantati, con patologie ematologiche concomitanti ➢ Strategie alla risposta completa ➢ Cosa fare alla resistenza (primaria o acquisita)
In conclusione ➢ Definizione ampia di «advanced cSCCC» ➢ Immunoterapia con Cemiplimab: ORR 50%; TTR 2 mesi; DOR non raggiunta ➢ Miglioramento qualità di vita e dolore ➢ Terapia potenzialmente curativa in sottogruppo di pz ➢ Ricerca di predittori ➢ Nuove strategie: (neo)adiuvante – combinazioni per revertire resistenza primaria/acquisita paolo.bossi@unibs.it
Puoi anche leggere