Idoneita sportiva nel soggetto con sincope - Giorgio Galan* - SESSIONE PLENARIA 5 SIMPOSIO GIMSI
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
SESSIONE PLENARIA 5 SIMPOSIO GIMSI
- SIC SPORT
“Cause aritmiche di sincope e/o di morte
improvvisa nello sportivo”
Idoneità sportiva nel
soggetto con sincope
Giorgio Galan*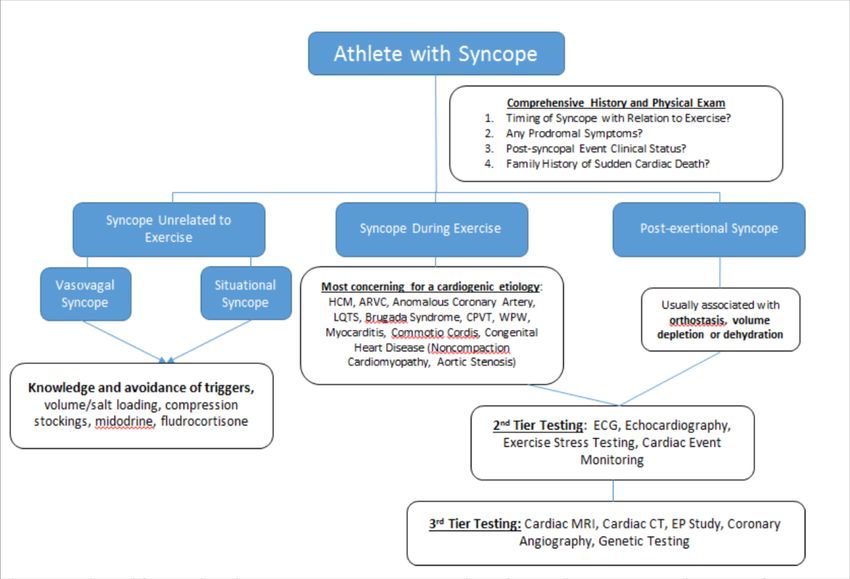
Tutela sanitaria
delle attività sportive
DM 18 2 1982
• Art. 1.
• Ai fini della tutela della salute, coloro che praticano
attività sportiva agonistica devono sottoporsi
previamente e periodicamente al controllo dell'idoneità
specifica allo sport che intendono svolgere o svolgono.
• La qualificazione agonistica a chi svolge attività
sportiva è demandata alle federazioni sportive nazionali
o agli enti sportivi riconosciuti.
• Devono sottoporsi altresì ai controlli di cui sopra i
partecipanti ai giochi della gioventù per accedere alle
fasi nazionali.
Attività sportiva a tutte le età
ØAthlete
any individual who engages in routine
vigorous physical exercise in the settings of
competition, recreation,or occupation.
ØElite athlete
requires regular competition against others
as a central componen requires vigorous and
intense training in a systematic
fashionplaces a high premium on excellence
and achievement
JACC December 2013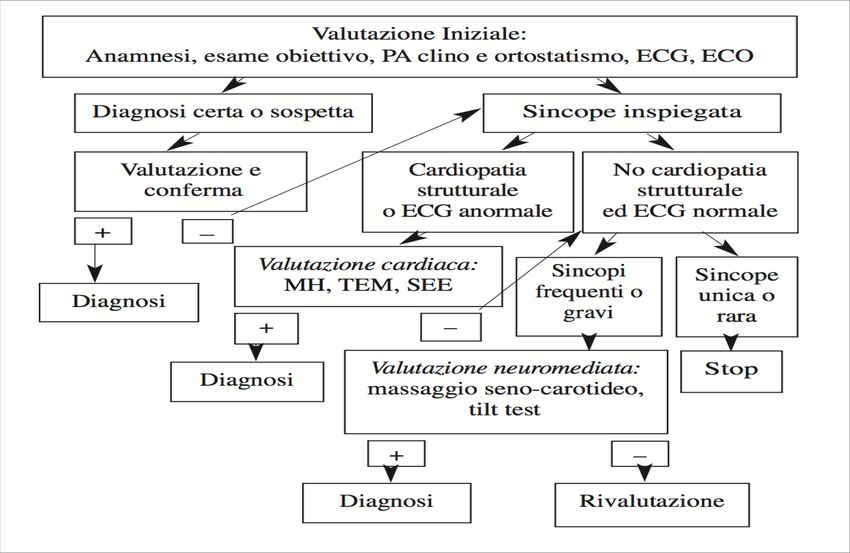
Quindi la certificazione medico sportiva
agonistica e non agonistica in Italia è per tutti
(atleti e non) e normata per legge
SYNCOPE
• Syncope is a transient loss of • La sincope è “un sintomo
consciousness caused by caratterizzato da un’improvvisa e
transient global cerebral transitoria perdita di coscienza e
hypoperfusion characterized by del tono posturale, con recupero
rapid onset, short duration, and spontaneo e completo in breve
spontaneous complete recovery. lasso di tempo”. Essa è dovuta ad
• Less frequently, syncope results una riduzione brusca e globale
from serious cardiovascular del flusso ematico cerebrale.
conditions that result in transient • La sincope può essere dovuta ad
loss of cerebral blood flow una varietà di cause. Le forme
because of an obstruction or principali sono: le sincopi
arrhythmias associated with neuromediate (vasovagale,
underlying structural heart senocarotidea, situazionale), le
disease. Primary electrical sincopi ortostatiche, le sincopi di
disorders can result in syncope in origine cardiaca (aritmiche o
the absence of any structural meccaniche), le sincopi
heart disease . cerebrovascolari.
Cocis 2017
Le forme principali sono
Øle sincopi neuromediate • Nella maggioranza degli atleti la
sincope ha una origine
(vasovagale, neuromediata e quindi una
senocarotidea, prognosi benigna .Tuttavia, essa
può costituire l’epifenomeno di
situazionale) una patologia cardiaca
Øle sincopi ortostatiche misconosciuta anche a prognosi
fatale e rappresentare un
Øle sincopi di origine potenziale marker di rischio di
morte improvvisa. A prescindere
cardiaca (aritmiche o dalla causa, la sincope è
meccaniche) associata a un rischio di
traumatismi, soprattutto in atleti
Øle sincopi praticanti sport a rischio
cerebrovascolari. intrinseco.
Cocis 2017
European Heart Journal (2004) 25, 1749–1753

European Heart Journal (2004) 25, 1749–1753

Incidenza della sincope per classi di età
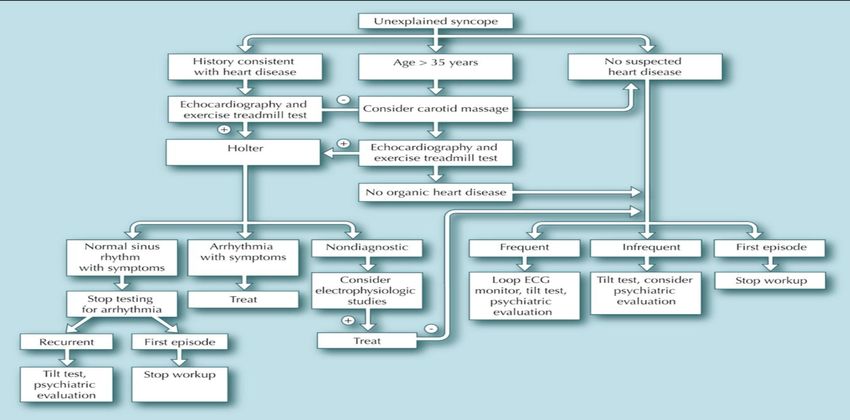
ITER DIAGNOSTICO
• Nella valutazione iniziale dell’atleta che ha
avuto una sincope vanno perseguiti tre
obiettivi prioritari:
• differenziare la sincope da altre condizioni
• valutare la presenza di cardiopatia;
• ricercare la presenza di elementi clinici in
grado di suggerire la diagnosi.
Cocis 2017• La valutazione iniziale deve comprendere l’anamnesi, l’esame
obiettivo con misurazione della pressione arteriosa in clino ed
in ortostatismo e l’ECG a 12 derivazioni. La storia clinica deve
includere un’anamnesi familiare, fisiologica e patologica
remota dettagliate, volte alla ricerca di patologie cardiache
genetiche o acquisite che possano essere causa di sincope.
L’anamnesi patologica pros- sima deve stabilire nel modo più
preciso possibile le modalità dell’evento sincopale o presunto
tale.
• Gli elementi anamnestici che suggeriscono un attacco non-
sincopale sono: confusione dopo l’attacco per più di 5 minuti,
movimenti tonico-clonici prolungati che iniziano prima
dell’attacco, automatismi, morsicatura della lingua, cianosi,
aura epilettica (epilessia); attacchi frequenti con disturbi
somatici in assenza di cardiopatia (malattia psichiatrica);
vertigine, disartria, diplopia (TIA).
• Gli elementi anamnestici che permettono una diagnosi
pressoché certa di sincope vaso-vagale sono la presenza di
eventi precipitanti quali paura, dolore, stress emozionale,
prolungato ortostatismo, associati ai tipici prodromi. Gli
elementi che suggeriscono con buona probabilità una sincope
vasovagale sono: il verificarsi della sincope dopo esercizio
fisico, dopo una visione, un suono o un odore improvviso
spiacevole e la presenza di nausea e vomito.
Cocis 2017• Syncope unrelated to exercise is the most common presenta4on, accoun4ng for
more than 85% of cases.This form of syncope (frequently referred to as
neurocardiogenic, or reflex or vasovagal syncope) is largely neurally mediated
with poorly understood pathophysiology.Vasovagal syncope, considered a benign
condi4on, typically occurs when going from a siEng to standing posi4on, or
experiencing fear or emo4onal distress with specific triggers such as sight of
blood or trauma. Frequently, these pa4ents describe a prodrome of
lightheadedness, pallor, a feeling of warmth, diaphoresis, and nausea or
epigastric pain. Situa4onal syncope, as the name implies, tends to be
reproducible with certain behaviors or ac4vi4es such as coughing, bearing down
to pass stool, or micturi4on. Dehydra4on and reduced intravascular volume can
induce a state of orthosta4c hypotension and induce a presyncopal event with
many of the same prodromal features of reflex syncope but importantly no loss of
consciousness.
• Post-exer4onal syncope frequently occurs when exercise is stopped suddenly and
reduc4on of lower extremity muscle pumping results in less cardiac venous
return and cardiac output. In such a circumstance, an acute increase in
myocardial contrac4lity can lead to ac4va4on of the cardiac depressor reflex
inducing concomitant paradoxical bradycardia. As a result, the athlete may
develop acute loss of postural tone, hypotension, and therefore transient global
cerebral hypoperfusion – this is termed the Bezold-Jarisch reflex.Contribu4ng
factors likely include dehydra4on and reduc4on in plasma volume. Syncope
immediately post-exercise which occurs when the subject is s4ll standing, is
usually less concerning than syncope during Shivanshu
exercise.Madan,Eugene H. Chung,2016 JACC• L’elemento anamnestico che permette una diagnosi certa di sincope situazionale è il verificarsi della sincope durante o immediatamente dopo minzione, defecazione, tosse o deglutizione. • L’elemento che permette una diagnosi certa di sincope ortostatica è rappresentato dalla documentazione di ipotensione ortostatica (decremento della pressione arteriosa sistolica ≥20 mmHg o a valori ≤90 mmHg) associata a sincope o presincope. • Gli elementi clinici che devono far sospettare una causa cardiaca sono: sincope che avviene in posizione supina; sincope durante esercizio fisico; sincope preceduta da palpitazioni; presenza di cardiopatia; presenza di alterazioni all’ECG di base; storia familiare di morte improvvisa. Cocis 2017
• Syncope or presyncope in an athlete mandates a thorough
evaluation by a qualified clinician. The purpose of the
evaluation is to determine the cause of syncope, with
particular emphasis on detecting structural or electrical
heart disease that may lead to sudden death.
• The evaluation should include a detailed history that
includes specific details of the event and observations of
witnesses when available. The distinction between syncope
during exercise and postexertional syncope is clinically
important. Most syncopal episodes that occur immediately
after exercise are benign. This pattern is believed to be a
result of transient postural hypotension caused by lower-
extremity pooling of blood once the athlete stops the
activity (from exercise-induced vasodilation) and the
resultant impairment of cardiac baroreflexes. It may be
potentiated by relative or absolute bradycardia attributable
to a parasympathetic surge at the cessation of exercise. By
contrast, syncope during exercise has a higher probability
of being caused by serious underlying cardiovascular
disease; however, neurally mediated syncope also can be
induced by prolonged intense exercise.
Shivanshu Madan,Eugene H. Chung,2016 JACC• The history should include asking about a family history of syncope, cardiovascular disease, and
sudden death. A careful physical examination with particular attention to the cardiovascular
examination should be performed in all athletes. Subsequent diagnostic testing in all patients should
include an ECG and an echocardiogram, with selective cardiovascular tests. These tests may include
a tilt table test, exercise stress test, ambulatory monitoring, and an implantable loop monitor.
The sensitivity and specificity of tilt table testing for the
diagnosis of syncope in the competitive athlete are lower
than for the general population, and some experts believe
there is not a role for tilt testing in the workup .
For those patients in whom the cause of syncope remains uncertain, especially if the syncope raises
concern for arrhythmic causes, contrast-enhanced magnetic resonance imaging, cardiac computed
tomography, coronary angiography, and invasive electrophysiological testing may be indicated.
Provocative testing with stress testing, epinephrine, procainamide, or isoproterenol should be
considered to identify otherwise concealed cases of long-QT syndrome, catecholaminergic
polymorphic VT, and Brugada syndrome. Genetic testing may be clinically useful in selected cases.
Shivanshu Madan,Eugene H. Chung,2016 JACCCirculation Vol84,No3 September1991
Conclusions. Endurance athletes have greater ventricular diastolic chamber compliance and
distensibility than nonathletes and thus operate on the steep portion of their Starling curve.
This may be a mechanical, nonautonomic cause of orthostatic intolerance.Physiological alterations accompanying acute exercise
and recovery and their possible sequelae in athlete
In athlete
Thompson Paul D
Exercise and Acute Cardiovascular EventsPhysiological alterations accompanying acute exercise
and recovery and their possible sequelae
Thompson Paul D
Exercise and Acute Cardiovascular EventsSyncope which occurs during exercise
• Syncope which occurs during exercise raises concern for
structural heart disease and can serve as the only symptom
that precedes sudden cardiac death.The differential diagnosis
for life-threatening causes of syncope in athletes includes
hypertrophic cardiomyopathy (HCM), anomalous coronary
artery, arrhythmogenic right ventricular dysplasia (ARVD), ion
channelopathies such as Long QT Syndrome (LQTS) or the
Brugada Syndrome, myocarditis, and even previously
undiagnosed congenital heart disease such as noncompaction
cardiomyopathy.Although not necessarily associated with
underlying native structural heart disease, commotio cordis is
an important cause of syncope and is characterized by sudden
cardiac death attributable to cardiac contusion from trauma to
the precordium.Heat stroke or hyponatremia must also be
considered in patients with exercise related syncope.
Shivanshu Madan,Eugene H. Chung,2016 JACCthe cause of syncope remains uncertain
• Echocardiography
• contrast-enhanced magnetic resonance imaging,
• cardiac computed tomography,
• coronary angiography,
• invasive electrophysiological testing may be indicated.
• Provocative testing with stress testing, epinephrine,
procainamide, or isoproterenol should be considered to
identify otherwise concealed cases of long-QT syndrome,
catecholaminergic polymorphic VT, and Brugada syndrome.
Genetic testing may be clinically useful in selected cases.
Shivanshu Madan,Eugene H. Chung,2016 JACC• Close monitoring of ECG changes during the exercise and recovery
periods would be crucial. Ambulatory cardiac event monitors should
also be used, and the choice of monitor depends on the frequency of
episodes. For very rare occurrences, an implantable loop recorder may
be required to capture the heart rhythm during a syncopal episode. With
respect of athletes, it is noteworthy that many event monitors require
adhesive, which can be troublesome to manage in a group of subjects
that are prone to active perspiration.
• A relatively new and potentially useful tool to evaluate patients is the
cell phone application that functions as a monitoring device. This
device allows “real-time” smartphone-based recording and transmission
of tracings in symptomatic athletes to consultants. This technology has
the potential to make quicker diagnoses and return athletes to back to
activity.
Shivanshu Madan,Eugene H. Chung,2016 JACCApproccio in un atleta con sincope Cocis 2017
Approach to the evaluation of an athlete with syncope
Athlete with Syncope
Syncope unrelated Syncope during Post exertional
to Exercise Exercise Syncope
Vasovagal Situational
Syncope Syncope
Shivanshu Madan,Eugene H. Chung,2016 JACCApproach to the patient with unexplained exercise-associated syncope.
Current Sports Medicine Reports 2006, 5:300–306IDONEITÀ ALLO SPORT • La sincope neuromediata nell’atleta ha una prognosi favorevole. Quindi, una volta accertata la natura neuromediata della perdita di coscienza, l’atleta può essere riammesso allo sport competitivo. Tuttavia devono essere adottati criteri restrittivi negli atleti praticanti sport a rischio intrinseco, cioè negli sport in cui la perdita di coscienza può comportare la possibilità di gravi eventi avversi per l’atleta stesso e per il pubblico che assiste alla gara. • Nelle sincopi di origine cardiaca aritmica o meccanica, la concessione dell’idoneità dovrà essere basata sul tipo e sulle caratteristiche della aritmia riscontrata e/o sulla patologia cardiovascolare associata Cocis 2017
ØLa idoneità può essere concessa
-nelle sindromi neuromediate
-nelle sindromi ortostatiche
E’ tuttavia consigliabile prudenza negli sport a
rischio intrinseco
ØL’idoneità andrebbe negata
-nelle sincopi di natura cardiaca,aritmiche e non,in
base al tipo di cardiopatia
-nelle sincopi di natura indeterminata è
consigliabile sospendere provvisoriamente
l’idoneità
Cocis 2017Recommendations Ø Athletes with exercise-induced syncope should be restricted from all competitive athletics until evaluated by a qualified medical professional (Class I; Level of Evidence B). Ø Athletes with syncope should be evaluated with a history, physical examination, ECG, and selective use of other diagnostic tests when there is suspicion of structural heart disease or primary electrical abnormalities that may predispose to recurrent syncope or sudden death (Class I; Level of Evidence C). Ø Athletes with syncope caused by structural heart disease or primary electrical disorders should be restricted from athletic activities according to the recommendations for their specific underlying cardiovascular condition (Class I; Level of Evidence C). Ø Athletes with neurallymediated syncope can resume all athletic activities once measures are demonstrated to prevent recurrent syncope (Class I; Level of Evidence C). Ø Athletes with syncope of unknown cause, based on a ruling out of structural or molecular pathogenesis, should not participate in athletics in which transient loss of consciousness can be hazardous (Class III; Level of Evidence C).
Conclusions and Attentions
• Ultimately, the goals of an evaluation for the athlete with
syncope are to determine whether underlying heart disease
is present, and whether athletic activity can safely be
continued.
• Missing or improperly treating a potentially life-threatening
etiology of syncope can have devastating consequences,
and the cost of misdiagnosing a benign condition as a
dangerous or life-threatening one can lead to unnecessary
restriction of activity as well as negative monetary and
psychosocial ramifications.
• Although most causes of syncope in the athlete are benign,
high profile stories such as the example above underscore
the importance of performing a comprehensive evaluation
beginning with a detailed history.
Shivanshu Madan,Eugene H. Chung,2016 JACCContro i medici 300mila cause in
corso, 35mila ogni anno
• A due anni dall’approvazione della Legge Gelli sulla nresponsabilità medica va
precisato che nella stragrande maggioranza dei casi le denunce che coinvolgono
dei medici si rivelano infondate e la speranza è che la Legge Gelli possa ridurre il
numero di cause (spesso temerarie) proposte.
• “le stime nel 2016 la percentuale complessiva dei medici coinvolti in
procedimenti giudiziari, sia civili che penali, rispetto al numero totale di
assicurati, era in calo in termini percentuali, ma nel 2017, i sinistri aperti e che
possono coinvolgere più professionisti per uno stesso evento avverso, sono
aumentati dal 2016 del 60%”.
• La Suprema Corte di Cassazione con l’ordinanza 30998 ha, per certi versi,
ridimensionato il valore da attribuire alle linee-guida nei processi per responsabilità
professionale medica in quanto le medesime non rappresentano (secondo i
giudici) “un letto di Procuste insuperabile”,ma solo uno strumento per valutare la
condotta del medico in un modo che tuttavia non può prescindere dall'analisi del
caso concreto».La decisione e l’intervento sono l’essenza della azione
La riflessione e le ipotesi sono l’essenza del pensiero
L’essenza della Medicina è la combinazione di questi
insieme di pensiero e di azione al servizio degli
altri.
Noi suggeriamo questi spunti per stimolare sia
l’azione che il pensiero:questi suggerimenti
possono essere difficili da mettere in atto ma come
le stelle possono essere utili per la navigazione
durante la notte.
Oxford Handbook of Clinical MedicineSESSIONE PLENARIA 5 SIMPOSIO GIMSI
- SIC SPORT
“Cause aritmiche di sincope e/o di morte
improvvisa nello sportivo”
Idoneità sportiva nel
soggetto con sincope
Giorgio Galan*Puoi anche leggere