Lichtenstein, Rives, Stoppa cosa ci resta? - GABRIELE MUNEGATO gabriele.munegato@gmail-com
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

Lichtenstein, Rives, Stoppa… cosa ci resta? GABRIELE MUNEGATO gabriele.munegato@gmail-com

June 25, 2000 … Dr. Lichtenstein, however, said that both the prolonged bed rest and the general anesthesia were unnecessary -- and that the anesthesia was even counterproductive. To prove this point, he insisted that many of his patients walk away from the table after surgery

… and he got one when he stood in front of a thousand doctors attending an American Medical Association meeting in San Francisco in 1964 and told them they were handling hernia patients all wrong.
1970 1986
Hernia repair without disability;: A surgical
atlas illustrating the anatomy, technique, and
physiologic rationale of the "one-day" hernia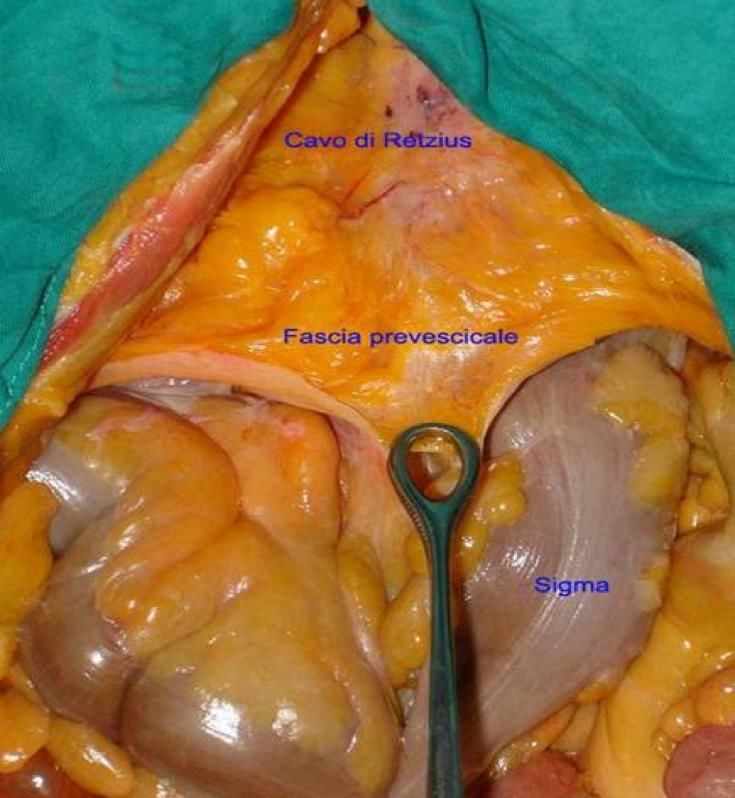
Anestesia locale e outpatient treatment • Giugno 1984: concetto di ernioplastica "tension free", priva di tensione, perché basata esclusivamente sul posizionamento di una rete protesica di rinforzo. • Shulman A.G., Amid P.L., Lichtenstein I.L.: The safety of mesh repair for primary inguinal hernias. Results of 3.019 operations from five diverse surgical sources. Am.Surg. 58:255-257.1992 Ernioplastica protesica “tension free”
…. “tension free”!!! • A 1986 article in a magazine published by Dr. Lichtenstein's alma mater, MCP Hahnemann University School of Medicine in Pennsylvania, recounted how he had been peppered by angry questions at the meeting. When Dr. Lichtenstein's time was up, the program director, eager to get things rolling again, suggested that those who still had questions take them into the hallway. Hundreds did so. • ''I was shocked,'' Dr. Lichtenstein remembered. ''So many people followed. Physicians were shouting questions at me, criticizing me, challenging me. There was a great deal of confusion and disorganization.''

Lichtenstein Hernia Center

Parviz AMID
Ambasciatore nel mondo della tecnica di
Lichtenstein
PLUG: una storia lunga ….
1974
LICHTENSTEIN
PLUG A SIGARETTA1987 1989 GILBERT TRABUCCO PLUG A CONO PLUG A PARACADUTE
The 'DIY Plug' - A cost effective plug hernia
repair
Sintler M1, Rittoo D1, Patel R2, Vohra RK1
1 Department of Vascular Surgery, Selly Oak Hospital, University Hospital Birmingham NHS
Trust, Selly Oak, Birmingham, United Kingdom
2 Russell's Hall Hospital, Dudley, West Midlands, United Kingdom
Do It Yourself
the cost is one-fourth that of the commercial system $40 vs $153Plug in polipropilene
Plug bioassorbibili Completamente Parzialmente
Henri
Fruchaud Première Guerre mondiale
Henri Fruchaud parvient tout de même à rester dans le
milieu médical en étant engagé comme caporal
brancardier au 90e régiment d'infanterie2. Il participe avec
son unité aux batailles de la Marne, d'Ypres, de l'Artois,
de Champagne, de Verdun et de la Somme3. Se
distinguant en toutes occasions, il est cité à plusieurs
reprises et est décoré de la Légion d'honneur, de
la médaille militaire et de la croix de guerre 1914-19182
Seconde Guerre Mondial
• Engagement dans la France Libre
• Mis à la tête du service de santé des forces françaises libres, il met en place une ambulance chirurgicale
légère destinée à être placée en soutien du corps expéditionnaire projeté en Afrique de l'Ouest au mois
de septembre. Embarqué sur le Westernland, il participe donc à la bataille de Dakar, campagne du
Gabon, campagne d'Erythrée.
• … Abyssinie, Palestine , Damas, Beyrouth .. mettre au point un poste chirurgical mobile consistant en
deux camions pouvant être assemblés entre eux et projetés en avant du dispositif principal de
l'ambulance.
• En décembre 1941… Libye … bataille de Bir Hakeim. Devant opérer les blessés dans des conditions
épouvantables sous les bombardements ennemis, Henri Fruchaud reste sur place malgré l'arrivée de la
relève le 30 mai 1945Henri
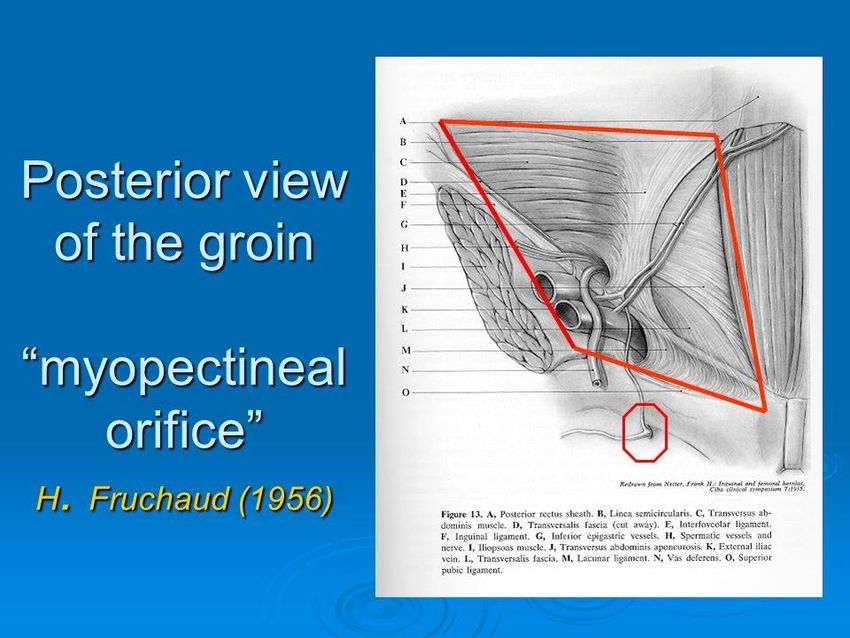
Fruchaud ANATOMIE CHIRURGICALE DE LA REGION DE L’AINE - 1956
MIOPECTINEAL ORIFICE
Istituto di Anatomia Di Algeri
Prof. Renè BourgeonORIFIZIO MIO-PETTINEO VISIONE UNITARIA DELLA PATOGENESI DELL’ERNIA INGUINO-CRURALE
HENRI FRUCHAUD ANATOMIE CHIRURGICALE DE LA REGION DE L’AINE - 1956
MIOPECTINEAL ORIFICE
“GROIN HERNIA DISEASE”
“…it may be said that a well man is an unknown hernia bearer”
“…in the adult repairing inguinal hernias into the femoral canal is
like closing the curtain instead of shutting the windows”
“…the treatment of inguinal or femoral hernias must not be the
closure of the inguinal canal or femoral hernias but the deep
reconstruction of the abdominal wall in the whole groin region.”OUTPATIENT
TREATMENT
TENSION Lichtenstein
FREE
FruchaudIstituto di Anatomia Di Algeri
Prof. Renè BourgeonIn una vasca con un buco è più efficace un tappo dall’interno che un tappo dal di fuori
ORIFIZIO MIOPETTINEO DI FRUCHAUD
PRINCIPIO DI PASCAL
UTILIZZO DELLO SPAZIO
PREPERITONEALE
SOTTOMBELICALEGreat
Prothesis for
Reinforcement
of Visceral Sac
(GPRVS sec.
Stoppa)• Dissezione preperitoneale • Riduzione sacco erniario • Parietalizzazione degli elementi • Protesi in mersilene a “chevron”
LAPAROSCOPIA - Transabdominal Preperitoneal Prosthesis (TAPP) - Total Extraperitoneal Prosthesis (TEP)
TEEP
TAPP
OUTPATIENT STOPPA
TREATMENT GPRVS
TENSION Lichtenstein
FREE
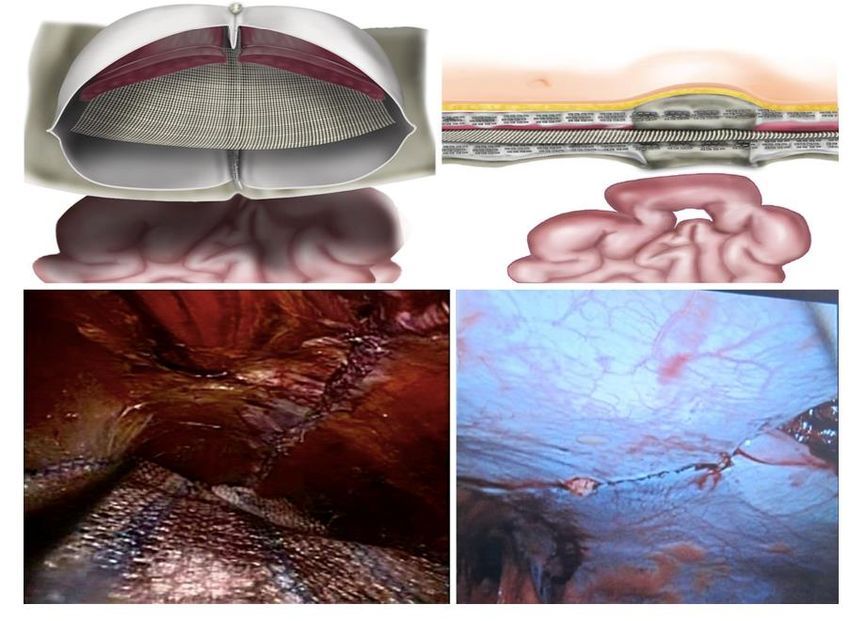
FruchaudLAPAROPLASTICA PROTESICA SEC.
RIVES STOPPA
Il nordafrica, l’Algeria
“Pied Noir”
Primari nel nord della Francia: Reims ed Amien
Amicissimi: ferie in barca in comune
Anatomisti: Rives-retromuscolare, Stoppa-
preperitoneale
Uso di protesi: poliestere (mersilene) e
polipropilene
GREPA (Groupe d’Etude Paroi Abdominale):
European Hernia Society
… una tecnica ancora giovane!Tenuta linea alba Trazione dei muscoli laterali “opponenti” ai retti I muscoli retti non hanno un muscolo “opponente” che ne favorisca la medializzazzione. La lesione della linea alba porta ad un grave indebolimento strutturale in quanto tre coppie di muscoli tendono sempre a diastasare retto e linea alba
RIVES - STOPPA
Riparazione
anatomico-funzionale
Rimane integro l’insieme anatomo-funzionale
muscoli retti-muscoli laterali dell’addomeConcettualità
reinserimento dei retti sulla linea mediana
Anatomia
piano di dissezione “facile”, esangue, rispettoso di
innervazioni
Materiale protesico
il posto migliore in cui posizionare una reteRECIDIVE: risultati ottimali
Recidive: “di confine” agli estremi superiori ed
inferiori della protesi
Evitabili con accorgimenti di tecnicaRegione ipogastrica
PROTESI
POLIESTERE (MERSILENE- FRANCIA)
,,, POLIFILAMENTO
MAGGIORE PERICOLO DI INFEZIONE
POLIPROPILENE (USA)
,,,MONOFILAMENTO
PIU’ RESISTENTE ALLE INFEZIONIIDEAL PROSTHESIS
5 KEY POINTS FOR AN OPTIMAL ACTION
Expeted Clinical Results Prosthesis characteristics
Fast Integration
Hydrophilicity
Limited fibrotic reaction Porosity
Comfort Compliance
Durability Stability
Antiadesion barrier
Adhesion prevention“Rapid tissue ingrowth for an efficient support... without extensive fibrosis
leading to discomfort, pain and erosion…good resistance to
infections”.
Hydrophilicity
α α
Porosity
Optimal Macroporosity > 1.5mm
Optimal Microporosity > 10µ
LIGHTWEIGHT: macroporosità e spessore filoLIMITI PROTESI SINTETICHE INFIAMMAZIONE CRONICA • Reazione da corpo estraneo • Shrinkage • Reazione aderenziale: occlusione, erosione, fistola • Rigidità parietale INFEZIONE CRONICA
RIPARAZIONE TESSUTALE
SCAFFOLD
RIGENERAZIONE
TESSUTALENUOVE PROTESI Sintetiche riassorbibili Biologiche
STIMOLO
• Meccanico
PROTESI • Chimico
• Fisico
CELLULE TOTIPOTENTI
FIBROBLASTI CELLULE
ENDOTELIALI
COLLAGENE I o NEOVASCOLARIZZAZION
III E
TESSUTO
NEOFORMATOFISSAZIONE PROTESI
punti transfissi transparietali attraverso
piccole incisioni cutanee mediante ago di
ReverdineCome e dove fissare la protesi
Punti protesi-
strutture
ossee
Reverdine
Colla
Protesi autofissantiIncisione “anteriore” della fascia del retto
Opzione per “lembo” posteriore
Ricostituzione piano posteriore con possibilità
di attuare tecnica di Rives
?Protesi direttamente a contatto con il grasso
sottocutaneo:
- maggior rischio di infezione protesica
Tecnica spesso non attuabile per “sofferenza
ischemica” del peritoneo
Nessuna
possibilità di
reinserimento
dei retti sulla
cerniera
medianaIncisione posteriore della fascia del retto
Mobilizzazzione lembo “posteriore”
Chiusura peritoneo-fasciale “anteriore” con
riavvicinamento mediano dei retti
Come ricostruire piano posteriore senza indurre
aumento di pressione addominale?Cosa e come fare ?
Problema
1) Anatomico
2) Funzionale: non aumentare la
pressione endoaddominale
Utilizzo di protesi cha consenta:
• riparazione parietale
• allargamento della cavita
addominaleLAPAROPLASTICA RIVES-STOPPA REINSERIMENTO SULLA LINEA MEDIANA DEI MUSCOLI RETTI
COMPONENT SEPARATION
RIVES - STOPPA
Riparazione
anatomico-funzionale
Rimane integro l’insieme anatomo-funzionale
muscoli retti-muscoli laterali dell’addomeSEPARAZIONE ANTERIORE
SEPARAZIONE
POSTERIORE
Muscolo trasverso:
• espiratorio
• corsetto muscolare in grado di contenere la pancia
• conferisce stabilità all’addomeAbdominal Wall Reconstruction -AWR
Rives - Stoppa
Complex Abdominal Wall Reconstruction - cAWR
Component SeparationTEEP
TAPP
OUTPATIENT STOPPA
TREATMENT GPRVS ACS
TENSION Lichtenstein Component
FREE Separation
PCS/TAR
Rives
Fruchaud StoppaTEEP
Robot
TAPP
OUTPATIENT STOPPA Laparo
TREATMENT GPRVS ACS
TENSION Lichtenstein Component
FREE Separation
PCS/TAR
Rives
Fruchaud StoppaRETROMUSCOLARE – SOVRAFASCIALE
tessuti riccamente vascolarizzati, presupposto fondamentale per
una buona integrazione protesicaGRANDI LAPAROCELI
Difetto di parete
• FISIOLOGICO: chiudere la parete
addominale senza aumentarne la pressione
•ANATOMICO: cosa fare quando non c’è
“stoffa”Puoi anche leggere