Influence of heart rate in the selection of the optimal reconstruction window in routine clinical multislice coronary angiography
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
Radiol med (2008) 113:644–657
DOI 10.1007/s11547-008-0303-4
CARDIAC RADIOLOGY
CARDIORADIOLOGIA
Influence of heart rate in the selection of the optimal reconstruction
window in routine clinical multislice coronary angiography
Influenza della frequenza cardiaca sulla scelta della finestra temporale di
ricostruzione ottimale nella coronaro-TC utilizzata nella routine clinica
G. Runza1 • L. La Grutta1 • V. Alaimo1 • L. Damiani1 • A. La Fata1 • F. Alberghina1 • M. Galia1
G. Lo Re1 • G. Luccichenti2 • T. Bartolotta1 • F. Cademartiri3,4 • M. Midiri1 • M. De Maria1
R. Lagalla1
1
Department of Radiology, University Hospital “P. Giaccone”, Via del Vespro 127, 90127 Palermo, Italy
2
Department of Radiology, IRCCS – Fondazione Santa Lucia, Rome, Italy
3
Department of Radiology and Cardiology, University Hospital, Parma, Italy
4
Department of Radiology and Cardiology, Erasmus Medical Center, Rotterdam, The Netherlands
Correspondence to: G. Runza, Tel.: +39-091-6552349, Fax: +39-091-6552324, e-mail: grunza@sirm.org
Received: 28 May 2007 / Accepted: 31 October 2007 / Published online: 1 July 2008
© Springer-Verlag 2008
Abstract Riassunto
Purpose. The aim of our study was to assess the influence Obiettivo. Scopo del nostro studio è valutare l’influenza
of heart rate on the selection of the optimal reconstruction della frequenza cardiaca (FC) nella scelta della migliore
window with 40-slice multidetector-row computed fase di ricostruzione in angiografia coronarica mediante
tomography (40-MDCT) coronary angiography. TC a 40 strati (AC-TCMS).
Materials and methods. We studied 170 patients (114 Materiali e metodi. Centosettanta pazienti (114 uomini,
men, age 60±11.3 years) with suspected or known età 60±11,3 anni) con sospetta o nota malattia coronarica
coronary artery disease with 40-MDCT coronary sono stati sottoposti ad AC-TCMS. I pazienti (frequenza
angiography. Patients [mean heart rate (HR) 62.9±9.3 bpm, media 62,9±9,3 bpm, range 42–94 bpm) sono stati
range 42–94 bpm] were clustered in two groups (group A: suddivisi in due gruppi (gruppo A: FC≤65 bpm; gruppo B:
HR ≤65 bpm; group B: HR >65 bpm). Multiphase FC>65 bpm). I dataset multifasici dell’AC-TCMS sono
reconstruction data sets were obtained with a retrospective stati ricostruiti ogni 5% da 0% a 95% dell’intero
electrocardiogram (ECG)-gated 40-MDCT coronary intervallo R-R. Due radiologi hanno valutato in accordo i
angiography scan from 0% to 95% every 5% of the R-R dataset utilizzabili clinicamente per la refertazione.
interval. Two radiologists in consensus evaluated the best Risultati. Nel gruppo A le fasi di ricostruzione ritenute
data sets for diagnostic purposes. ottimali sono state il 70% (55/110, 71/110 e 69/110,
Results. In group A, the optimal reconstruction windows rispettivamente, per la coronaria destra – CDx – per
were at 70% (55/110, 71/110 and 69/110 for the right l’interventricolare anteriore – IVA – e per la circonflessa –
coronary artery, left anterior descending and the left CX) ed il 75% (26/110, 28/110 e 28/110, rispettivamente).
circumflex, respectively) and 75% (26/110, 28/110 and Nel gruppo B è stata utilizzata un ampia gamma di
28/110, respectively) of the R-R interval. In group B, a ricostruzioni, in particolare al 40% (32/60, 18/60 e 17/60,
wide range of reconstruction windows were employed, rispettivamente per la CDx, per l’IVA e per la CX) ed al
both in the end-systolic phase at 40% (32/60, 18/60 and 70% (12/60, 22/60 e 19/60, rispettivamente). Sei esami
17/60, for the right coronary artery, left anterior sono stati esclusi dallo studio per la presenza di artefatti
descending and circumflex, respectively) and diastolic da movimento respiratorio.
phases at 70% (12/60, 22/60 and 19/60, respectively). Six Conclusioni. La scelta della finestra temporale di
scans were excluded due to severe respiratory artefacts. ricostruzione è significativamente dipendente dalla FC
Conclusions. Optimal position of the image reconstruction media durante la scansione. Le ricostruzioni in fase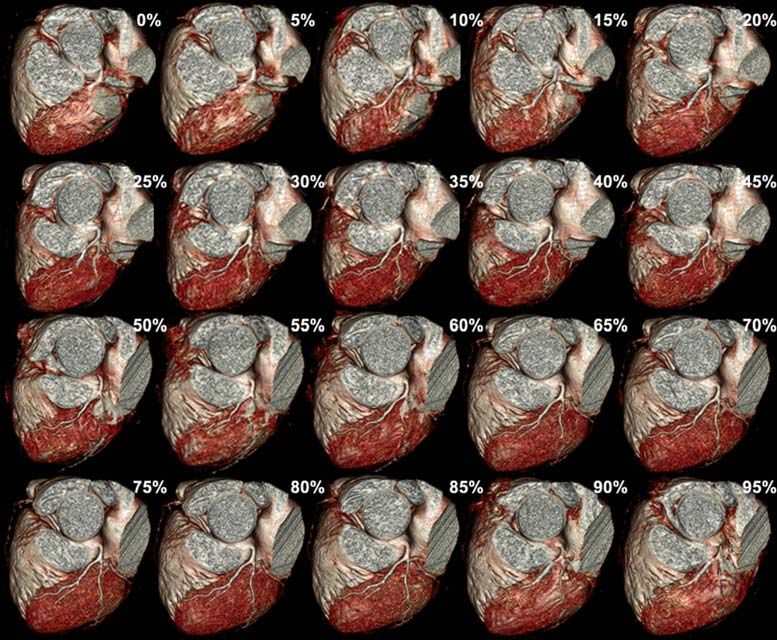
Radiol med (2008) 113:644–657 645
window relative to the cardiac cycle is significantly diastolica consentono spesso una valutazione ottimale con
influenced by the heart rate during scanning. Diastolic FC≤65 bpm. La scelta delle fasi sistoliche (30%–45%) è
reconstruction phases often allowed an optimal assessment consigliabile, invece, per FC più elevate.
in group A. Reconstruction phases from 30% to 45% are
advisable for higher heart rates. Parole chiave Tomografia computerizzata multistrato ·
Angiografia coronarica · Sincronizzazione retrospettiva
Keywords Multislice computed tomography · Coronary all’ECG · Frequenza cardiaca
angiography · Retrospective ECG gating · Heart rate
Introduction Introduzione
Coronary angiography with multidetector-row computed to- L’angiografia coronarica mediante tomografia computeriz-
mography (MDCT) is finding increasing use in routine clin- zata multistrato (AC-TCMS) viene sempre più spesso utiliz-
ical practice as a noninvasive diagnostic tool for evaluating zata nella routine clinica come strumento diagnostico non
coronary arteries. Scanners with increasing spatial and tem- invasivo per la valutazione delle arterie coronarie. Le ap-
poral resolution have been developed over the years [1–6]. parecchiature con una sempre migliore risoluzione spaziale
However, regardless of their diagnostic performance, arte- e temporale si sono alternate negli ultimi anni [1–6]. Tutta-
facts caused by heart motion are still the greatest obstacle in via, a prescindere dal miglioramento della performance
clinical practice, given their negative influence on the diag- diagnostica, gli artefatti da movimento cardiaco continuano
nostic accuracy of the technique. a costituire la più grossa difficoltà della routine clinica de-
Image quality is highly dependent on heart rate (HR) and terminando un peggioramento dell’accuratezza diagnostica
the reconstruction window selected using retrospective elec- della metodica.
trocardiogram (ECG) gating. Various studies have evaluat- La qualità dell’immagine è fortemente dipendente dalla
ed the optimal reconstruction window with 4-slice [7–9], frequenza cardiaca (FC) e dalla finestra temporale di rico-
16-slice [10–12] and recently 64-slice CT [13]. Increasing struzione selezionata utilizzando il gating retrospettivo
temporal resolution could lead to use of a single reconstruc- all’ECG. Numerosi studi hanno valutato l’intervallo otti-
tion window, thus limiting the amount of data to be recon- male di ricostruzione con la TC a 4 strati [7–9], con la TC
structed and therefore the amount of data to be archived, as a 16 strati [10–12] e recentemente con la TC a 64 strati
well as minimising the dose of ionising radiation delivered [13]. L’aumento della risoluzione temporale potrebbe con-
to the patient [14]. durre in futuro all’impiego di un singolo intervallo di rico-
The aim of our study was to evaluate the influence of HR struzione, ridimensionando l’ammontare dei dati ricostruiti
on the choice of the optimal reconstruction window for re- e, quindi, gli spazi di archiviazione, e minimizzando la dose
porting an examination performed with 40-slice MDCT di radiazioni ionizzanti assorbita dal paziente [14].
coronary angiography. Scopo del presente lavoro è valutare l’influenza della FC
nella scelta della fase di ricostruzione ottimale per la refer-
tazione di un esame di AC-TCMS a 40 strati.
Materials and methods
Study population Materiali e metodi
Between February and May 2006, 170 consecutive patients Popolazione studiata
(114 men, 56 women; mean age 60±11.3 years, range 19–80
years) underwent 40-MDCT coronary angiography (Bril- Nel periodo compreso tra febbraio e maggio 2006, 170 pa-
liance 40, Philips Medical Systems, Cleveland, OH, USA). zienti (114 uomini, 56 donne; età media 60±11,3 anni, ran-
Indications for examination were stable angina (61), atypical ge 19–80 anni) consecutivi sono stati sottoposti ad angio-
chest pain (37), unstable angina (5), follow-up of proximal grafia coronarica TC a 40 strati (Brilliance 40, Philips Me-
stents (20), follow-up of bypass grafts (30), elevated cardio- dical Systems, Cleveland, Ohio, USA). I pazienti hanno ese-
vascular risk (patients with metabolic syndrome – 11), sus- guito l’indagine per angina stabile (n=61), dolore toracico
pected coronary anomalies (2), suspected cardiac masses (2) atipico (n=37), angina instabile (n=5), follow-up di stent
and preoperative planning for valve replacement (2). prossimali (n=20), follow-up di by-pass (n=30), rischio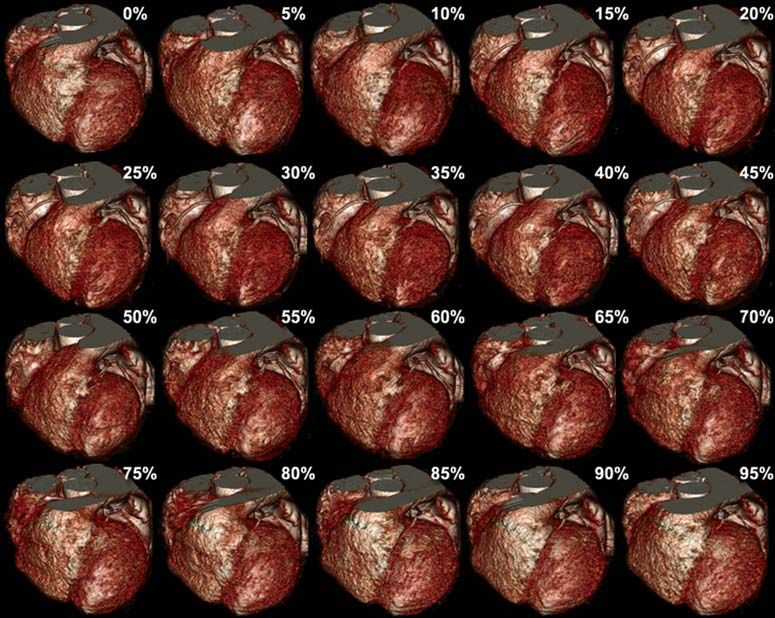
646 Radiol med (2008) 113:644–657
The normally recognised inclusion criteria for MDCT cardiovascolare elevato (pazienti affetti da sindrome meta-
coronary angiography are sinus cardiac rhythm with 120 μmol/l), allergia nota ai mezzi di contrasto
mean HR in 20 patients recorded during the scan was >70 iodati, possibile gravidanza, presenza di aritmie ipercineti-
bpm. The patient population (mean HR 62.9±9.3 bpm, che (ad esempio fibrillazione atriale, extrasistolia, ecc.),
range 42–94) was divided into two groups, with a threshold compromissione della funzione respiratoria, disordini tiroi-
of 65 bpm (group A: HR ≤65 bpm; group B HR>65 bpm). dei, stato clinico instabile o marcata insufficienza cardiaca.
A tutti i pazienti sono state spiegate le diverse fasi della pro-
Scan and reconstruction parameters cedura d’esame e la corretta modalità di esecuzione
dell’apnea inspiratoria.
All scans were performed with a 40-slice CT scanner (Bril- Nonostante la somministrazione di 20–40 mg di β-bloc-
liance 40, Philips Medical Systems, Cleveland, Ohio, USA). cante, in 20 pazienti la FC media registrata durante la
A quantification of coronary calcium was performed with scansione si è mantenuta >70 bpm. I pazienti (frequenza
prospective triggering at 70% of the R-R interval with the cardiaca media 62,9±9,3 bpm, range 42–94 bpm) sono sta-
following scan parameters: FOV 150–200 mm, kV 120, ti suddivisi in due gruppi, impiegando un valore soglia di 65
mAs 70, slice thickness 2.5 and 50% overlap. bpm (gruppo A: FC≤65 bpm; gruppo B: FC>65 bpm).
The angiographic scans were performed with the follow-
ing parameters: retrospective ECG gating, number of detec- Parametri di scansione e di ricostruzione
tors/collimation 40×0.625, voxel 0.34 mm3 (isotropic reso-
lution), gantry rotation time 420 ms (effective temporal res- Tutte le scansioni sono state effettuate con una TC a 40
olution, with linear reconstruction algorithm at 180°, 210 strati (Brilliance 40, Philips Medical Systems, Cleveland,
ms), feed/rotation 11.9 mm/s (pitch 0.2), voltage 120 kV, Ohio, USA). È stata eseguita una quantificazione del calcio
tube current 1,035 mAs, scan direction craniocaudal. Tube coronarico mediante gating prospettico al 70% dell’inter-
current modulation was not selected by the operator. vallo R-R, con i seguenti parametri di scansione: FOV
A bolus of 120 ml of nonionic iodinated contrast material 150–200 mm, kV 120, mAs 70, spessore 2,5 mm e sovrappo-
(Iomeprol, Iomeron® 400, Bracco, Milan, Italy) was injected sizione del 50%.
at a flow rate of 5 ml/s with an automatic power injector (Stel- Le scansioni angiografiche sono state effettuate con i se-
lant, MedRAD, Pittsburgh, PA, USA) connected to an 18- guenti parametri: modalità di sincronizzazione retrospettiva
gauge needle cannula with right antecubital access. To opti- al tracciato ECG, numero di detettori/collimazione
mise intraluminal enhancement of the coronary arteries, the 40×0,625 mm, voxel 0,34 mm3 (risoluzione isotropica), tem-
beginning of the scan was synchronised by using the bolus- po di rotazione 420 ms (risoluzione temporale effettiva, con
tracking technique (Philips Medical Systems, Cleveland, algoritmo di ricostruzione lineare a 180°, 210 ms), avanza-
Ohio, USA) with a region of interest (ROI) at the level of the mento/rotazione 11,9 mm/s (pitch 0,2), voltaggio del tubo
ascending aorta. The scan began automatically with a delay of radiogeno 120 kV, tensione del tubo radiogeno 1035 mAs,
Radiol med (2008) 113:644–657 647
8 s after the threshold of 120 HU was reached within the ROI. direzione della scansione cranio-caudale. Dall’operatore
A retrospective reconstruction was performed for each non è stata scelta la modalità di modulazione dell’ampe-
coronary artery (right coronary artery – RCA; left anterior raggio del tubo radiogeno.
descending coronary artery – LAD: left circumflex coronary Un bolo di 120 ml di mezzo di contrasto iodato non-ioni-
artery – LCX) in the various phases of the cardiac cycle, each co (Iomeprol, Iomeron® 400, Bracco, Milano, Italia) è sta-
5% of the R-R interval from 0% to 95%, for a total of 20 da- to iniettato con un flusso di 5 ml/s mediante iniettore auto-
ta sets. The reconstructions were performed with the follow- matico (Stellant, MedRAD, Pittsburgh, PA, USA) collegato
ing parameters: slice thickness 0.8 mm, reconstruction incre- ad un’agocannula da 18 gauge, posizionata in una vena an-
ment 0.4 mm, medium (CB) and sharp (CC) convolution ker- tecubitale destra. Allo scopo di ottimizzare l’enhancement
nels. The data sets were transferred to a dedicated worksta- intraluminale dei vasi arteriosi coronarici la sincronizza-
tion (Extended BrillianceTM Workspace, Version 3.0.1.3200, zione dell’inizio della scansione con il passaggio del bolo di
Philips Medical Systems, Cleveland, Ohio, USA). mezzo di contrasto è stata eseguita mediante tecnica del Bo-
lus Tracking (Philips Medical Systems, Cleveland, Ohio,
Data analysis USA), con una ROI (region of interest) posizionata al livel-
lo dell’aorta ascendente. La scansione è partita automati-
Data analysis was performed on all segments of the coro- camente con un ritardo di 8 secondi dopo il raggiungimen-
nary arteries with a diameter ≥1.5 mm. All reconstructed to all’interno della ROI di una soglia di 120 UH.
images were evaluated by two radiologists with level-3 ex- Per ogni coronaria (arteria coronaria destra, CDx; ar-
perience in MDCT coronary angiography by using multi- teria interventricolare anteriore, IVA; arteria circonflessa,
planar reconstructions (MIP) and maximum intensity pro- CX) è stata effettuata una ricostruzione retrospettiva nelle
jections (MIP) [15]. varie fasi del ciclo cardiaco ogni 5% dell’intervallo R-R
The data sets retrospectively reconstructed every 5% of dallo 0% al 95% per un totale di 19 dataset. Le ricostru-
the R-R interval were compared, and the data set with the zioni sono state effettuate con i seguenti parametri: spesso-
best image quality per individual vessel was identified. For re 0,8 mm, incremento 0,4 mm, filtri di convoluzione medio
each MDCT coronary angiography examination, a global as- (CB) e sharp (CC). I dataset sono stati trasferiti su una
sessment was made of image quality in relation to a single re- workstation dedicata (Extended BrillianceTM Workspace,
constructed data set or the integration of several data sets. A Versione 3.0.1.3200, Philips Medical Systems, Cleveland,
four-point scale was used to evaluate the coronary arteries Ohio, USA).
with a diameter ≥1.5 mm: absence of motion artefacts and
clear outline of the vessel (grade 1); minor artefacts with min- Analisi dei dati
imal blurring (grade 2); blurring artefacts without interruption
in the course of the vessel (grade 3); artefacts with severe L’analisi è stata effettuata in tutti i segmenti di arterie co-
doubling/interruption of the course of the vessel (grade 4) ronarie con diametro ≥1,5 mm. Tutte le immagini ricostrui-
[16]. A diagnostic assessment within grade 3 was considered te sono state indipendentemente valutate da due radiologi
acceptable in terms of image quality for routine clinical prac- con esperienza di livello 3 in AC-TCMS mediante riformat-
tice. The operators performed all evaluations by consensus. tazioni multiplanari (MPR) e proiezioni di massima inten-
sità (MIP) [15].
Statistical analysis Tra i dataset ricostruiti retrospettivamente ogni 5%
dell’intervallo R-R, è stato identificato quello con la mi-
Statistical analysis was performed with a dedicated software gliore qualità di immagine per singolo vaso coronarico ed
package (Statistica, version 5.0, StatSoft Italia, Vigonza, PD, in grado di consentire l’ottimale espressione di un giudizio
Italy). An estimation was made of the statistical difference diagnostico. Ad ogni AC-TCMS ottenuta è stato anche at-
between the two groups in terms of age (t test), Agatston cal- tribuito un giudizio sulla qualità d’immagine globale otte-
cium score (t test), gender and administration of beta-block- nuta mediante un singolo dataset di ricostruzione o l’inte-
ers (Fisher’s exact test). The chi-squared test was used to grazione di più dataset. È stata utilizzata una scala in gra-
evaluate the difference in distribution in the systolic and di- di per la valutazione delle arterie coronarie con diametro
astolic phases in the two groups for each coronary artery. ≥1,5 mm: assenza di artefatti di movimento con chiara de-
lineazione del vaso (grado 1); artefatti minori con minimo
blurring (grado 2); artefatti da blurring senza disconti-
Results nuità di decorso dei vasi (grado 3); artefatti severi con
sdoppiamento/discontinuità dei vasi (grado 4) [16]. Un
No significant difference was found with regard to age giudizio diagnostico entro il grado 3 è stato considerato
(group A: 60.7±10.7 years; group B: 59.0±12.3 years; accettabile in termini di qualità di immagine per la routine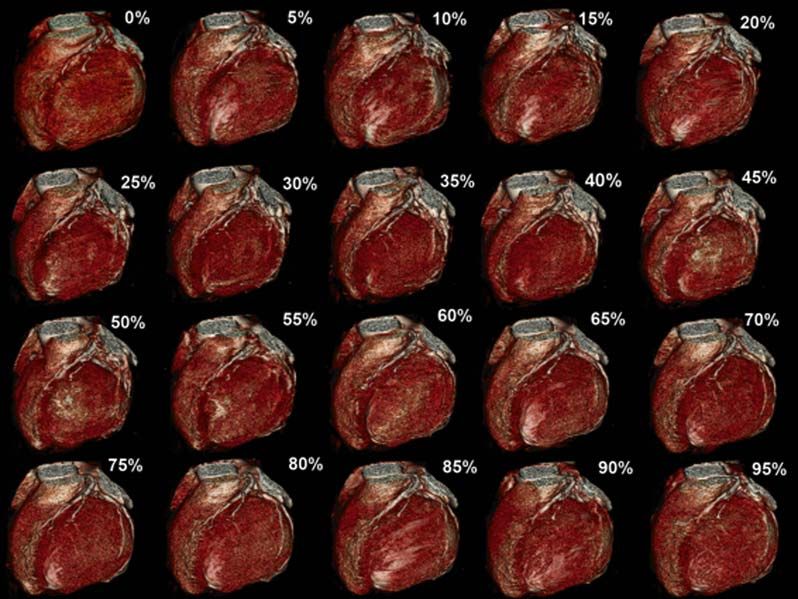
648 Radiol med (2008) 113:644–657
p=0.29), Agatston calcium score (group A: 185±278; group clinica. Tutte le valutazioni sono state svolte in accordo
B: 205±352; p=0.68) and administration of beta-blockers dagli operatori.
(61 patients in group A; 37 patients in group B; p=0.51). A
significantly higher number of women were found in group Analisi statistica
B (30 patients; p < 0.05).
The number of examinations assessed as having diagnos- L’analisi statistica è stata eseguita con un software dedica-
tic quality for routine clinical practice (absence of motion to (Statistica, versione 5.0, StatSoft Italia, Vigonza, PD, Ita-
artefacts with clear outline of the vessel; minor artefacts lia). È stata stimata la differenza statistica tra i due gruppi
with minimal blurring; blurring artefacts without interrup- per età (test t di Student), calcium score calcolato secondo il
tion in the course of the vessel) was 164. Acceptable image sistema di Agatston (test t di Student), sesso e somministra-
quality (grades 1–3) was found in 96.5% of our population zione di β-bloccanti (test esatto di Fisher). Il test del χ2 è
(Fig. 1; Table 1). Only six patients (3.5%) with a mean stato utilizzato per valutare la differente distribuzione delle
HR >65 bpm during the scan were considered grade 4, as fasi sistoliche e diastoliche nei due differenti gruppi per cia-
none of the available data sets allowed an acceptable diag- scuna arteria coronarica.
Fig. 1 Distribution of artefacts in the
study population examined with 40-
row multidetector computed tomogra-
phy coronary angiography.
Fig. 1 Distribuzione degli artefatti
ARTEFACTS nelle indagini AC-TCMS della popo-
lazione analizzata.
Table 1 Image quality of the 40-row multidetector computed tomography coronary angiography examination in the study population by vessel in the two
groups
Grade Artefacts Group A (HR ≤65 bpm) Group B (HR >65 bpm)
RCA LAD LCX RCA LAD LCX
1 Absent 80 (72.7%) 102 (92.7%) 94 (85.5%) 22 (36.7%) 28 (46.7%) 24 (40%)
2 Minor 24 (21.8%) 8 (7.3%) 12 (10.9%) 21 (35%) 23 (38.3%) 19 (31.7%)
3 Moderate 6 (5.5%) 0 4 (3.6%) 11 (18.3%) 5 (8.3%) 12 (20%)
4 Severe 0 0 0 6 (10%) 4 (6.7%) 5 (8.3%)
HR, heart rate; RCA, right coronary artery; LAD, left anterior descending coronary artery; LCX, left circumflex coronary artery
Tabella 1 Qualità delle immagini delle indagini AC-TCMS nella popolazione analizzata per singolo vaso nei due gruppi
Grado Artefatti Gruppo A (FC≤65 bpm) Gruppo B (FC>65 bpm)
CDx IVA CX CDx IVA CX
1 Assenti 80 (72,7%) 102 (92,7%) 94 (85,5%) 22 (36,7%) 28 (46,7%) 24 (40%)
2 Minori 24 (21,8%) 8 (7,3%) 12 (10,9%) 21 (35%) 23 (38,3%) 19 (31,7%)
3 Moderati 6 (5,5%) 0 4 (3,6%) 11 (18,3%) 5 (8,3%) 12 (20%)
4 Severi 0 0 0 6 (10%) 4 (6,7%) 5 (8,3%)
FC, frequenza cardiaca; CDx, arteria coronaria destra; IVA, arteria coronaria interventricolare anteriore; CX, arteria coronaria circonflessa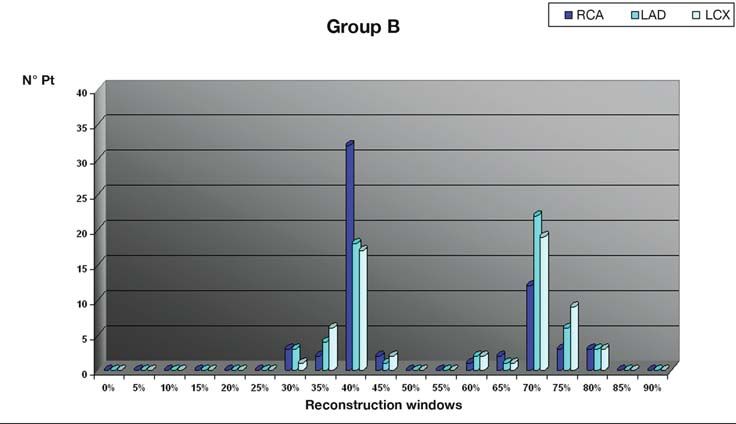
Radiol med (2008) 113:644–657 649 nostic evaluation due to the presence of excessive motion Risultati artefacts (doubling/interruption of the vessel). In group A, acceptable image quality was achieved in Nessuna differenza significativa è stata riscontrata tra i due 100% of patients, to a large extent without motion artefacts gruppi per età (gruppo A: 60,7±10,7 anni; gruppo B: (71.8%). In group B, acceptable image quality was achieved 59±12,3 anni; p=0,29), calcium score calcolato secondo il in 90% of patients, with a reduction in the number of exam- sistema di Agatston (gruppo A: 185±278; gruppo B inations without artefacts (36.7%). In group A, the optimal 205±352; p=0,68) e somministrazione di β-bloccanti (61 reconstruction windows for diagnostic quality images were pazienti nel gruppo A; 37 pazienti nel gruppo B; p=0,51). È at 70% (55/110, 71/110 and 69/110 for the RCA, LAD and stato riscontrato un numero significativamente più alto di LCX, respectively) and 75% (26/110, 28/110 and 28/110, pazienti di sesso femminile nel gruppo B (30 pazienti; respectively) of the R-R interval. The RCA was better visu- p65 bpm du- tolic phase was noted for the evaluation of the RCA (65%). rante la scansione sono stati considerati come grado 4 poi- At the same time, a significant number of reconstructions in ché nessun dataset disponibile consentiva una valutazio- the end-systolic phase were optimal for the evaluation of ne diagnostica accettabile a causa della presenza di ecces- the LAD (43.3%) and the LCX (43.3%) (Table 3). The use sivi artefatti da movimento (sdoppiamento/discontinuità of end-systolic and end-diastolic reconstructions for evalua- dei vasi). tion of the RCA, LAD and LCX was significantly different Nel gruppo A una qualità d’immagine accettabile (gradi in the two groups (p
650 Radiol med (2008) 113:644–657
Table 3 Optimal reconstruction windows in group B ni AC-TCMS prive di artefatti (36,7%). Nel gruppo A le fa-
si ottimali di ricostruzione per esprimere un giudizio dia-
R-R interval RCA LAD LCX
gnostico risultano al 70% (55/110, 71/110 e 69/110 per la
0% 0 0 0 CDx, la IVA e la CX) ed al 75% (26/110, 28/110 e 28/110,
5% 0 0 0 rispettivamente). La CDx è stata meglio visualizzata al
10% 0 0 0 40% in 18/110, al 35% in 4/110 ed al 30% in 1/110. In al-
15% 0 0 0 cuni casi anche la IVA (2/110 al 40%, 2/110 al 35%) e la
20% 0 0 0
25% 0 0 0
CX (3/110 al 40%) sono state visualizzate in fase telesisto-
30% 3 3 1 lica. Non sempre una sola finestra temporale consente una
35% 2 4 6 lettura ottimale dell’esame per tutti i vasi coronarici (Ta-
40% 32 18 17 bella 2). Nel gruppo B è stata utilizzata un’ampia gamma
45% 2 1 2 di fasi di ricostruzioni: in particolare al 40% (32/60, 18/60
50% 0 0 0
55% 0 0 0
e 17/60, rispettivamente) ed al 70% (12/60, 22/60 e 19/60,
60% 1 2 2 rispettivamente). È stata registrata una prevalenza delle
65% 2 1 1 fasi telesistoliche per la valutazione della CDx (65%). Allo
70% 12 22 19 stesso tempo, un consistente numero di ricostruzioni in fa-
75% 3 6 9 se telesistolica è stato riscontrato per la valutazione di IVA
80% 3 3 3
85% 0 0 0
(43,3%) e CX (43,3%) (Tabella 3). L’impiego delle rico-
90% 0 0 0 struzioni telesistoliche e telediastoliche per la valutazione
95% 0 0 0 di CDx, IVA e CX è risultato significativamente differente
nei due gruppi (p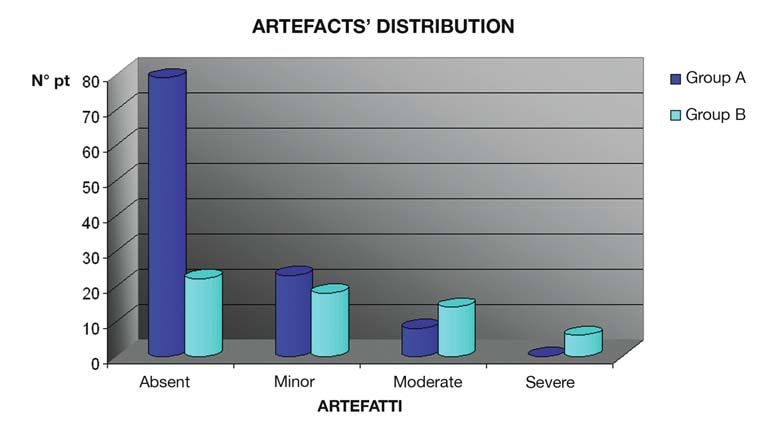
Radiol med (2008) 113:644–657 651 extracted by shifting the beginning of image reconstruction dotto al minimo. In numerosi casi la fase telesistolica può with regard to the R wave, with the aim of reducing motion fornire informazioni rilevanti; infatti, anche al termine del- and blurring artefacts to a minimum [17]. la contrazione miocardica il movimento delle arterie coro- A number of approaches can be used when performing narie risulta minimo [8]. the reconstructions. These include: (1) relative delay strate- Di solito, vengono eseguite multiple ricostruzioni in dif- gy, whereby the delay time is a percentage of the R-R inter- ferenti finestre temporali e l’operatore, successivamente, val; (2) absolute delay strategy, whereby the delay time is sceglie il dataset dove gli artefatti da movimento sono ri- constant after the previous R wave; (3) absolute reverse de- dotti al minimo, eventualmente utilizzando nello stesso pa- lay strategy, whereby the delay time is constant prior to the ziente differenti finestre temporali per la rappresentazione next R wave; (4) end of the time window positioned at the della CDx, dell’IVA e della CX [1–5]. Indubbiamente, la peak of the P wave [18]. A real optimisation of retrospective routine clinica è condizionata, in questo caso, da due fatto- gating is yet to be achieved. The four techniques described ri: il tempo necessario per le operazioni di ricostruzione da can be used indiscriminately, but this depends on the degree parte dell’operatore cui consegue certamente un aumento of experience of the operator, the software/hardware capa- degli spazi di archiviazione; la dose di radiazioni impiega- bilities and the time available for reconstruction. The car- ta nell’utilizzo del gating retrospettivo che pone in partenza diac cycle phase that provides the most information extends seri interrogativi sulla giustificazione dell’esame. from mid to end diastole. In this phase, the heart is in iso- Vari studi hanno indagato sul rapporto tra qualità d’im- volumetric filling, and motion is at a minimum. In many magine ed intervallo temporale ottimale di ricostruzione cases, the end-systolic phase can provide relevant informa- con differenti TC a 4, 16 e 64 detettori [7–13, 19]. Con la tion, as the motion of the coronary arteries is also at a mini- TC a 4 strati, l’IVA era meglio visualizzata al 50%–70%, la mum at the end of myocardial contraction [8]. CX al 50%–60%, la CDx al 40%–50% dell’intervallo R-R Multiple reconstructions are usually performed in differ- [7–9], indicando il bisogno di ricostruzioni separate per i ent reconstruction windows, and later the operator selects vari vasi. Con la TC a 16 strati la migliore qualità di imma- the data set where motion artefacts are at a minimum, possi- gine veniva solitamente raggiunta nella diastole media bly using different reconstruction windows in the same pa- (–350 ms, –400 ms o –450 ms, corrispondenti approssimati- tient for visualisation of the RCA, LAD and LCX [1–5]. Of vamente al 60%–70%) [10], con eventuali ricostruzioni ad- course, routine clinical practice in this case is conditioned dizionali telesistoliche per frequenze elevate [10–12]. Lo by two factors: (1) the time required by the operator to per- studio di Leschka et al. [13] con la TC a 64 strati ha messo form the reconstructions and any consequent increase in in evidenza che ricostruzioni addizionali durante la sistole archiving space, and (2) the radiation dose used for retro- non sono più necessarie, anche a frequenze elevate, dal mo- spective gating, which poses important questions for justifi- mento che anche con frequenze >65 bpm, il 4% dei segmen- cation of the examination. ti con miglior qualità d’immagine in sistole raggiungeva Various studies have investigated the relationship be- una qualità d’immagine diagnostica anche in diastole [13]. tween image quality and the optimal reconstruction window Dal momento che la AC-TCMS con gating retrospettivo è with 4-, 16- and 64-slice scanners [7–13, 19]. With 4-MD- caratterizzata dall’utilizzo di un’elevata dose di radiazioni CT, the LAD is best visualised at 50%–70%, the LCX at ionizzanti specialmente con la TC a 64 strati, i risultati di 50%–60% and the RCA at 40%–50% of the R-R interval questo studio potrebbero autorizzare in futuro all’utilizzo [7–9], thus indicating the need for separate reconstructions indiscriminato dell’ECG-pulsing, cioè ad un’acquisizione for the different vessels. With 16-MDCT, optimal image mirata esclusivamente nelle finestre temporali meso-tele- quality is usually obtained in mid diastole (350 ms, –400 ms diastoliche, con riduzione di dose del 48% negli uomini e or –450 ms, corresponding approximately to 60%–70%) del 45% nelle donne [4, 14]. Nonostante ciò tutti gli studi [10], with additional reconstructions in the end-systolic con TC a 64 strati per la valutazione dell’accuratezza dia- phase for higher HR where required [10–12]. The study by gnostica nell’individuazione delle stenosi emodinamica- Leschka et al. with 64-MDCT showed that additional recon- mente significative su popolazioni selezionate non applica- structions during systole were no longer necessary, even at no questa tecnica ed utilizzano più finestre temporali di ri- higher HR, as even at HR >65 bpm, the 4% of segments costruzione del ciclo cardiaco [1–5]. with better image quality during systole were also of diag- La recente introduzione di TC a 64 strati con doppio tu- nostic quality during diastole [13]. As MDCT coronary an- bo radiogeno-sistema rilevatore (dual source-CT), grazie giography is characterised by the use of high doses of ionis- ad una migliore risoluzione temporale (82,5 ms), offre la ing radiation, particularly with 64-MDCT, the results of this possibilità di ottenere una qualità d’immagine indipenden- study could pave the way for the widespread use of ECG te dalla FC e rende, pertanto, superfluo l’utilizzo dei ‚- pulsing, that is, an acquisition targeted exclusively at the bloccanti per ridurla [20, 21]. L’utilizzo di questa nuova mid- to end-diastolic reconstruction windows, thus reducing tecnologia di TCMS con la possibilità di modulare la cor-
652 Radiol med (2008) 113:644–657
the radiation dose by 48% in men and 45% in women rente del tubo radiogeno potrebbe consentire l’ottimizza-
[4, 14]. Despite this, most studies with 64-MDCT for the eval- zione dei meccanismi di ECG-pulsing con una riduzione
uation of diagnostic accuracy in the identification of haemo- della dose di radiazioni al paziente [20, 21]. Un ulteriore
dynamically significant stenoses in selected populations do avanzamento potrebbe essere rappresentato dalla TC a
not apply this technique and, instead, use reconstruction win- 256 strati con scansioni real-time prive di ECG-gating, che
dows from different phases of the cardiac cycle [1–5]. eliminerebbero la necessità della valutazione di ricostru-
With its significant improvement in temporal resolution zioni in differenti finestre temporali del ciclo cardiaco, ma
(82.5 ms), the recently introduced 64-slice dual-source CT al momento l’unica esperienza clinica riportata in Lettera-
offers the possibility of obtaining image quality indepen- tura è un work-in-progress limitato a due soli pazienti
dent of HR and therefore eliminates the need for beta-block- [22].
ers to reduce HR [20, 21]. The use of this new MDCT tech- Nella routine clinica, tuttavia, nonostante la sommini-
nology could optimise tube current modulation and reduce strazione di β-bloccanti per ridurre la FC o nell’impossibi-
the radiation dose delivered to the patient [20, 21]. A further lità di poterli somministrare per l’esistenza di controindica-
development could be 256-MDCT with its real-time scan- zioni, ci si può confrontare, a volte inaspettatamente (ansia
ning and ECG gating, which would eliminate the need for e reazione agli elevati flussi di infusione del mezzo di con-
reconstructions in different time windows of the cardiac cy- trasto, specialmente, nel sesso femminile), con FC media
cle, although at present, the only study reported in the liter- >65 bpm. Peraltro, la moltitudine di applicazioni cliniche
ature is a work in progress limited to two patients [22]. della AC-TCMS e le variabili caratteristiche del paziente
In routine clinical practice, however, despite the admin- che ne conseguono non sempre permettono di raggiungere
istration of beta-blockers to reduce HR or where their ad- una FC ottimale [23].
ministration is contraindicated, the HR may unexpectedly Il nostro studio intende, quindi, valutare, utilizzando una
rise above 65 bpm (due to anxiety and reaction to high flow TC a 40 strati, l’influenza della FC media sulla scelta della
rates of contrast material, particularly in women). More- finestra temporale di ricostruzione del ciclo cardiaco, indi-
over, the numerous clinical applications of MDCT coronary pendentemente da un valore soglia (≤65 bpm) e riconoscen-
angiography and the variability in patient characteristics do done una riduzione, anche se modesta, del valore diagnosti-
not always allow an optimal HR to be achieved [23]. co direttamente proporzionale all’aumento della FC media
Our study, therefore, aimed to evaluate the influence of (6 pazienti del gruppo B esclusi dalla valutazione diagno-
HR on the choice of reconstruction window, independently stica per gli eccessivi artefatti da movimento).
of a threshold (≤65 bpm), while recognising a reduction, al- Nel gruppo A (FC≤65 bpm) (Figg. 1, 2) le finestre tem-
though modest, of the diagnostic value directly proportional porali di ricostruzione risultano ottimali al 70% (55/110,
to the increase in HR (six group B patients were excluded 71/110 e 69/110 per la CDx, l’IVA e la CX, rispettivamente)
with nondiagnostic quality images due to severe motion ed al 75% (26/110, 28/110 e 28/110 per la CDx, l’IVA e la
artefacts). CX, rispettivamente). Nel Gruppo B (FC>65 bpm) (Figg.
In group A (HR ≤65 bpm, Figs. 1, 2), the optimal recon- 3–5) è stata utilizzata, invece, un’ampia gamma di ricostru-
struction windows were at 70% (55/110, 71/110 and 69/110 zioni, con rilievo particolare di quelle telesistoliche al 40%
for the RCA, LAD and LCX, respectively) and 75% (32/60, 18/60 e 17/60, rispettivamente). In questo gruppo 6
(26/110, 28/110 and 28/110, respectively). In group B (HR indagini sono state considerate non diagnostici per gli ec-
>65 bpm – Figs. 3–5), in contrast, a broad range of recon- cessivi artefatti da movimento.
structions were used, particularly in the end-systolic phase, Mentre nel gruppo A (Fig. 7) le finestre temporali di ri-
at 40% (32/60, 18/60 and 17/60, respectively). In this group, costruzione più utilizzate sono quelle al 70%–75% con al-
six examinations were judged nondiagnostic due to exces- cune eccezioni (40%: 18/110 per la CDx, 2/110 per l’IVA e
sive motion artefacts. 3/110 per la CX; 35%: 4/110 per la CDX, 2/110 per l’IVA;
Whereas the most used reconstruction windows in group 30%: 1/110 per la CDX), con frequenze elevate (gruppo B)
A (Fig. 7) were at 70%–75% with some exceptions (40%; (Fig. 8) il numero delle ricostruzioni per una AC-TCMS
18/110 for RCA, 2/110 for LAD and 3/110 for LCX), with diagnostica aumenta significativamente ed appare impre-
high HR (group B, Fig. 8), the number of reconstructions scindibile l’utilizzo delle fasi telesistoliche. Con la risolu-
required to achieve diagnostic quality images at MDCT zione temporale raggiunta dalla nostra apparecchiatura
coronary angiography significantly increased, suggesting TC, l’utilizzo dell’ECG-pulsing risulta prematuro. La riso-
that the use of the end-systolic phase is indispensable. With luzione temporale migliore di scanner a 64 strati potrebbe
the temporal resolution achieved by our 40-MDCT scanner, consentirne l’utilizzo. Tuttavia il modello attuale di ECG-
the use of ECG pulsing appears impracticable. The better pulsing non appare ancora consigliabile per le valutazioni
temporal resolution of a 64-slice scanner could allow for its cliniche dal momento che tutti gli studi di accuratezza dia-
use. Nonetheless, the current ECG-pulsing model does not gnostica della AC-TCMS riportati in letteratura si servono,Radiol med (2008) 113:644–657 653
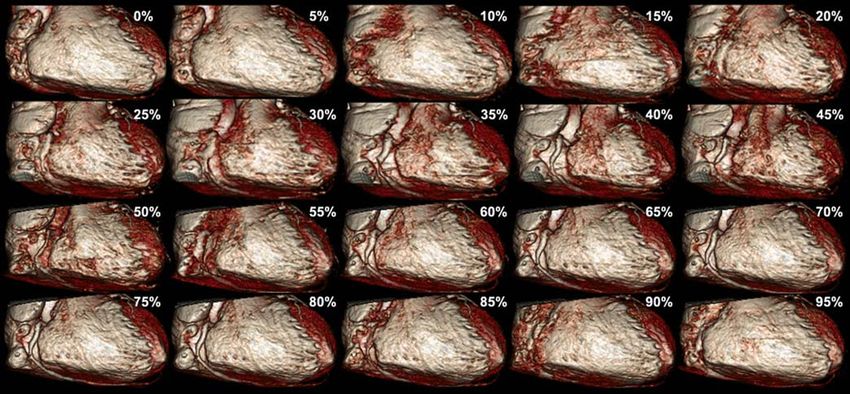
Fig. 2 Volume-rendered reconstructions performed every 5% of the R-R interval from 0% to 95% of the cardiac cycle for a total of 20 data sets in a group
A patient with a mean heart rate of 49 bpm. The images clearly show that both the end-systolic (40%) and the mid- to end-diastolic (from 60% to 80%) re-
construction windows are of diagnostic quality in the evaluation of the right coronary artery.
Fig. 2 Riformattazioni Volume Rendering effettuate ogni 5% dell’intervallo R-R dallo 0% al 95% del ciclo cardiaco per un totale di 20 dataset, in un pa-
ziente del gruppo A, con frequenza cardiaca media di 49 bpm. È ben dimostrata la possibilità di utilizzo a scopo valutativo diagnostico delle finestre tem-
porali di ricostruzione sia in fase telesistolica (40%) che in meso-telediastolica (dal 60% all’80%), per la valutazione dell’arteria coronaria destra.
Fig. 3 Volume-rendered reconstruc-
tions performed every 5% of the R-
R interval from 0% to 95% of the
cardiac cycle for a total of 20 data
sets in the same group A patient as
Fig. 2, with a mean heart rate of 49
bpm. The left coronary artery tree
(left main, left anterior descending,
left circumflex and intermediate
branch) can also be evaluated with
the reconstruction windows in the
end-systolic (40%) and mid- to end-
diastolic (from 60% to 80%) cardiac
phases in precisely the same way as
the right coronary artery.
Fig. 3 Riformattazioni Volume Ren-
dering effettuate ogni 5% dell’inter-
vallo R-R dallo 0% al 95% del ciclo
cardiaco per un totale di 20 dataset,
nello stesso paziente del gruppo A
riportato in Fig. 2, con frequenza
cardiaca media di 49 bpm. Anche
per l’albero coronarico sinistro
(tronco comune, arteria coronaria
interventricolare anteriore, arteria
circonflessa e ramo intermedio) è
possibile utilizzare a scopo valutati-
vo diagnostico le finestre temporali
di ricostruzione sia in fase telesisto-
lica (40%) che in meso-telediastoli-
ca (dal 60% all’80%), in maniera
del tutto sovrapponibile a quelle per
l’arteria coronaria destra.654 Radiol med (2008) 113:644–657
Fig. 4 Volume-rendered reconstruc-
tions performed every 5% of the R-R
interval from 0% to 95% of the car-
diac cycle for a total of 20 data sets in
a group B patient with a mean heart
rate of 84 bpm. The reconstruction
windows useful for diagnostic pur-
poses are those in systole (from 30%
to 45%), although image quality is
reduced and diagnosis is limited to
the proximal and mid segments of the
coronary artery tree.
Fig. 4 Riformattazioni Volume Ren-
dering effettuate ogni 5% dell’inter-
vallo R-R dallo 0% al 95% del ciclo
cardiaco per un totale di 20 dataset,
in un paziente del gruppo B, con fre-
quenza cardiaca media di 84 bpm. Le
finestre temporali di ricostruzione
utilizzabili a scopo diagnostico, an-
che se con una ridotta qualità
dell’immagine e limitatamente ai
segmenti prossimali e medi dell’albe-
ro coronarico, sono quelle che com-
prendono la sistole (dal 30% al
45%).
Fig. 5 Volume-rendered reconstructions performed every 5% of the R-R interval from 0% to 95% of the cardiac cycle for a total of 20 data sets in a group
B patient with a mean heart rate of 81 bpm. The reconstruction windows useful for diagnostic purposes of the right coronary artery are those in systole (from
30% to 45%).
Fig. 5 Riformattazioni Volume Rendering effettuate ogni 5% dell’intervallo R-R dallo 0% al 95% del ciclo cardiaco per un totale di 20 dataset, in un pa-
ziente del gruppo B, con frequenza cardiaca media di 81 bpm. Le finestre temporali di ricostruzione utilizzabili a scopo diagnostico per l’arteria corona-
ria destra sono quelle che comprendono la sistole (dal 30% al 45%).Radiol med (2008) 113:644–657 655
Fig. 6 Volume-rendered recon-
structions performed every 5% of
the R-R interval from 0% to 95%
of the cardiac cycle for a total of
20 data sets in a group B patient
with a mean heart rate of 73 bpm.
The reconstruction windows use-
ful for diagnostic purposes of the
left anterior descending and left
circumflex coronary arteries are
those in mid- to end-diastole
(from 60% to 80%). In this case,
reconstructions in the systolic
phase are of poor quality.
Fig. 6 Riformattazioni Volume
Rendering effettuate ogni 5%
dell’intervallo R-R dallo 0% al
95% del ciclo cardiaco per un to-
tale di 20 dataset, in un paziente
del gruppo B, con frequenza car-
diaca media di 73 bpm. Le fine-
stre temporali di ricostruzione
utilizzabili a scopo diagnostico
per l’arteria coronaria interven-
tricolare anteriore e l’arteria co-
ronaria circonflessa sono quelle
in fase mesotelediastolica (dal
60% all’80%). In questo caso le
ricostruzioni in fase sistolica ri-
sultano avere una qualità di im-
magine inferiore.
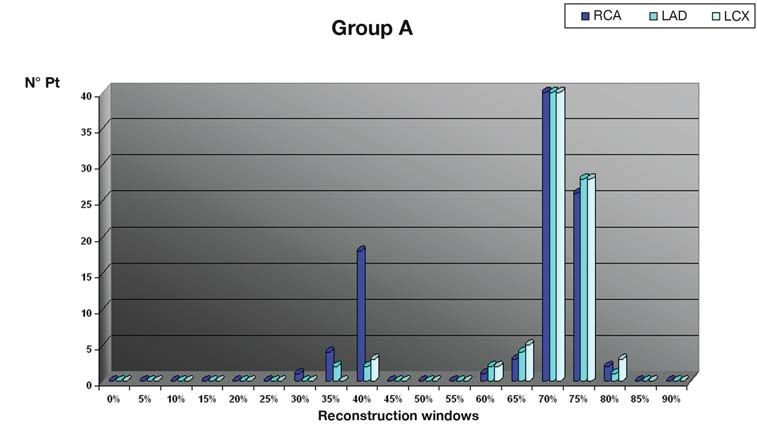
N° Pt
Fig. 7 Distribution of the recon-
struction windows used for the di-
agnostic evaluation in group A di-
vided by coronary vessel (RCA,
right coronary artery; LAD, left
anterior descending coronary
artery; LCX, left circumflex coro-
nary artery).
Fig. 7 Distribuzione delle finestre
temporali di ricostruzione utiliz-
zate per la valutazione diagnosti-
ca nel gruppo A suddivise per sin-
golo vaso coronarico (CDx, arte-
ria coronaria destra; IVA, arteria
coronaria interventricolare ante-
Reconstruction windows riore; CX, arteria coronaria cir-
conflessa).
appear advisable for clinical evaluation, as all of the pub- comunque, per la valutazione di più ricostruzioni in diffe-
lished studies of diagnostic accuracy of MDCT coronary an- renti finestre temporali del ciclo cardiaco.
giography perform the evaluation with a number of different
reconstruction windows of the cardiac cycle.
Conclusioni
Sulla base della nostra esperienza clinica con AC-TCMS la
Conclusions scelta della finestra temporale di ricostruzione del ciclo
cardiaco appare influenzata dalla frequenza cardiaca me-
On the basis of our clinical experience with MDCT coronary dia registrata durante la scansione. L’utilizzo di protocolli
angiography, the choice of the reconstruction window of the di ricostruzione preimpostati in base alla frequenza cardia-656 Radiol med (2008) 113:644–657
N° Pt
Fig. 8 Distribution of the reconstruc-
tion windows used for the diagnostic
evaluation in group B divided by
coronary vessel (RCA, right coronary
artery; LAD, left anterior descending
coronary artery; LCX, left circumflex
coronary artery).
Fig. 8 Distribuzione delle finestre
temporali di ricostruzione utilizzate
per la valutazione diagnostica nel
gruppo B suddivise per singolo vaso
coronarico (CDx, arteria coronaria
destra; IVA, arteria coronaria inter-
Reconstruction windows
ventricolare anteriore; CX, arteria
coronaria circonflessa).
cardiac cycle appears to be influenced by the mean HR ca media durante la scansione potrebbe consentire una ri-
recorded during the scan. The use of preset reconstruction duzione dei tempi di ricostruzione per l’operatore e della
protocols based on mean HR during the scan could enable quantità di spazio occupato sui sistemi di archiviazione del-
the reduction in reconstruction time for the operator and the le immagini.
quantity of space occupied in image archiving systems. Le ricostruzioni in fase diastolica consentono nella mag-
Reconstructions in the diastolic phase in most cases en- gior parte dei casi un’ottimale valutazione per frequenze
able an optimal diagnostic evaluation with mean HR ≤65 cardiache medie ≤65 bpm. Per frequenze >65 bpm, rico-
bpm. With HR >65 bpm, reconstructions from 30% to 45% struzioni dal 30% al 45% sono consigliabili per ottenere
are advisable to obtain acceptable image quality for diag- una qualità d’immagine accettabile, necessaria a fornire un
nostic purposes. giudizio diagnostico.
References/Bibliografia
1. Leber AW, Knez A, von Ziegler F et al 4. Mollet NR, Cademartiri F, van 8. Hong C, Becker CR, Huber A et al
(2005) Quantification of obstructive Mieghem CA et al (2005) High- (2001) ECG-gated reconstructed multi-
and nonobstructive coronary lesions by resolution spiral computed tomography detector row CT coronary angiography:
64-slice computed tomography: a coronary angiography in patients effect of varying trigger delay on image
comparative study with quantitative referred for diagnostic conventional quality. Radiology 220:712–717
coronary angiography and intravascular coronary angiography. Circulation 9. Kopp AF, Schroeder S, Kuettner A et al
ultrasound. J Am Coll Cardiol 112:2318–2323 (2001) Coronary arteries:
46:147–154 5. Pugliese F, Mollet NR, Runza G et al retrospectively ECG-gated multi-
2. Leschka S, Alkadhi H, Plass A et al (2006) Diagnostic accuracy of non- detector row CT angiography with
(2005) Accuracy of MSCT coronary invasive 64-slice CT coronary selective optimization of the image
angiography with 64-slice technology: angiography in patients with stable reconstruction window. Radiology
first experience. Eur Heart J angina pectoris. Eur Radiol 16:575–582 221:683–688
26:1482–1487 6. Flohr TG, Stierstorfer K, Ulzheimer S 10. Hamoir XL, Flohr T, Hamoir V et al
3. Raff GL, Gallagher MJ, O’Neill WW, et al (2005) Image reconstruction and (2004) Coronary arteries: assessment of
Goldstein JA (2005) Diagnostic image quality evaluation for a 64-slice image quality and optimal
accuracy of noninvasive coronary CT scanner with z-flying focal spot. reconstruction window in retrospective
angiography using 64-slice spiral Med Phys 32:2536–2547 ECG-gated multislice CT at 375-ms
computed tomography. J Am Coll 7. Giesler T, Baum U, Ropers D et al gantry rotation time. Eur Radiol
Cardiol 46:552–557 (2002) Noninvasive visualization of 15:296–304
coronary arteries using contrast-
enhanced multidetector CT: influence
of heart rate on image quality and
stenosis detection. AJR Am J
Roentgenol 179:911–916Radiol med (2008) 113:644–657 657
11. Bley TA, Ghanem NA, Foell D et al 16. Shim SS, Kim Y and Lim SM (2005) 22. Kondo C, Mori S, Endo M et al (2005)
(2005) Computed tomography coronary Improvement of image quality with Real-time volumetric imaging of
angiography with 370-millisecond beta-blocker premedication on ECG- human heart without
gantry rotation time: evaluation of the gated 16-MDCT coronary angiography. electrocardiographic gating by 256-
best image reconstruction interval. AJR Am J Roentgenol 184:649–654 detector row computed tomography:
J Comput Assist Tomogr 29:1–5 17. Ohnesorge B, Flohr T, Becker C et al initial experience. J Comput Assist
12. Sanz J, Rius T, Kuschnir P et al (2005) (2000) Cardiac imaging by means of Tomogr 29:694–698
The importance of end-systole for electrocardiographically gated 23. Hendel RC, Patel MR, Kramer CM et
optimal reconstruction protocol of multisection spiral CT: initial al (2006)
coronary angiography with 16-slice experience. Radiology 217:564–571 ACCF/ACR/SCCT/SCMR/ASNC/NAS
multidetector computed tomography. 18. Cademartiri F, Luccichenti G, Marano CI/SCAI/SIR 2006 appropriateness
Invest Radiol 40:155–163 R et al (2003) Non-invasive criteria for cardiac computed
13. Leschka S, Husmann L, Desbiolles LM angiography of the coronary arteries tomography and cardiac magnetic
et al (2006) Optimal image with multislice computed tomography: resonance imaging: a report of the
reconstruction intervals for non- state of the art and future prospects. American College of Cardiology
invasive coronary angiography with Radiol Med 106:284–296 Foundation Quality Strategic Directions
64-slice CT. Eur Radiol 16:1964–1972 19. Hoffmann MH, Shi H, Manzke R et al Committee Appropriateness Criteria
14. Jakobs TF, Becker CR, Ohnesorge B et (2005) Noninvasive coronary Working Group, American College of
al (2002) Multislice helical CT of the angiography with 16-detector row CT: Radiology, Society of Cardiovascular
heart with retrospective ECG gating: effect of heart rate. Radiology Computed Tomography, Society for
reduction of radiation exposure by 234:86–97 Cardiovascular Magnetic Resonance,
ECG-controlled tube current 20. Flohr TG, McCollough CH, Bruder H American Society of Nuclear
modulation. Eur Radiol 12:1081–1086 et al (2006) First performance Cardiology, North American Society
15. Budoff MJ, Achenbach S, Fayad Z et al evaluation of a dual-source CT (DSCT) for Cardiac Imaging, Society for
(2006) Task Force 12: training in system. Eur Radiol 16:256–268 Cardiovascular Angiography and
advanced cardiovascular imaging 21. Johnson TR, Nikolaou K, Interventions, and Society of
(computed tomography): endorsed by Wintersperger BJ et al (2006) Dual- Interventional Radiology. J Am Coll
the American Society of Nuclear source CT cardiac imaging: initial Cardiol 48:1475–1497
Cardiology, Society for Cardiovascular experience. Eur Radiol 16:1409–1415
Angiography and Interventions, Society
of Atherosclerosis Imaging and
Prevention, and Society of
Cardiovascular Computed
Tomography. J Am Coll Cardiol
47:915–920Puoi anche leggere