ANDREA STRADA STEFANO ROSSI MATTEO GUARINO PS S.ANNA
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

ANDREA STRADA
STEFANO ROSSI
MATTEO GUARINO
PS S.ANNA
Ferrara
La sepsi non esiste

In Italy, Spain, the UK, France and the USA, a mean of 88%
of interviewees had never heard of the term “sepsis”
and of people who recognized it, 58% did not recognize
that sepsis is a leading cause of death: failure to
recognize symptoms of sepsis earlier may lead to a delay
access to care.
Crit Care Med 2012 37:167–170
A preceding survey in those same countries out of a sample
of 1058 doctors highlighted their difficulty in defining and
diagnosing the syndrome and only 17% agreed upon any
definition of sepsis.
Crit Care 2012 8:R409–R413
LA SEPSI E’ UNA “SINDROME”
TERMINE “OPERATIVO”
DIAGNOSI DI “LAVORO”
The Third International Consensus
Definitions for Sepsis and Septic Shock
(Sepsis-3) JAMA. 2016;315(8):801-810
La sepsi è una disfunzione d’organo minacciosa per la vita
per un’abnorme risposta all’infezione da parte dell’ospite
Lo shock settico è un tipo di sepsi.
La disfunzione circolatoria, metabolica e cellulare
è tale da aumentare la mortalità
A review of the process of care received by patients with sepsis
A report by the NCEPOD 2015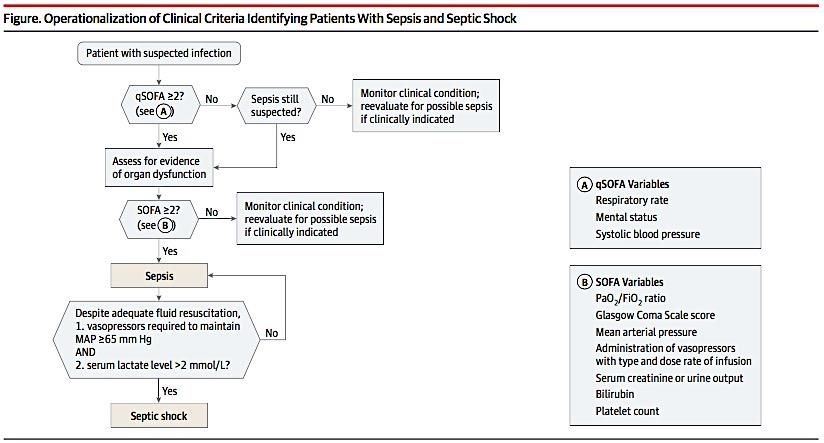
RITARDO DIAGNOSTICO:
in 182/505 (36%) casi di sepsi
in 167/324 (51.5%) casi di sepsi severa
in 63/193 (32.6%) di shock settico
Solo nel 52.9% dei pz era registrato il GCS alla diagnosi
Solo nel 61,7% dei pz vi era un valore del lattato
Accertamenti essenziali per la diagnosi di sepsi non fatti
nel 39.1% dei pz o ritardati nel 38.3%
A review of the process of care received by patients with sepsis
A report by the NCEPOD (2015)
6 ORE!!
PRONTO SOCCORSO Ragionar per bandiere rosse

Riconoscimento precoce della sepsi
in Pronto Soccorso: il quickSOFA
Stefano Rossi
UO Pronto Soccorso e Medicina d’Urgenza
(Direttore: A. Strada – Coordinatore A. Pesci)
Azienda Ospedaliero – Universitaria S. Anna, FerraraManagement of Sepsis
Managing resuscitation
Fluids: For patients with sepsis-induced hypoperfusion,
provide 30mL/kg of intravenous crystalloid within 3hours
(strong recommendation; low QOE) with additional fluid
based on frequent reassessment (BPS), preferentially using
Managing infection dynamic variables to assess fluid responsiveness (weak
recommendation; lowQOE).
Antibiotics: Administer broad-spectrum intravenous
antimicrobials for all likely pathogens within 1 hour
after sepsis recognition (strong recommendation;
moderate quality of evidence [QOE]). Resuscitation targets: For patients with septic shock
requiring vasopressors, target a mean arterial pressure
Source control: Obtain anatomic source control as (MAP) of 65mm Hg (strong recommendation; moderate
rapidly as is practical (best practice statement [BPS]). QOE).
Antibiotic stewardship: Assess patients daily for
deescalation of antimicrobials; narrow therapy based on Vasopressors: Use norepinephrine as a first-choice
cultures and/or clinical improvement (BPS). vasopressor (strong recommendation; moderate QOE).Source: http://epmonthly.com/article/sepsis-gets-an-upgrade/ Score bed-side Un punteggio maggiore o uguale a 2 associato a segni di infezione suggerisce un aumentato rischio di decesso Mortalità < 1% con 0 punti e superiore al 20% con 3 punti
I numeri del Pronto Soccorso Pronto Soccorso Generale Anno N° Accessi Differenza (%) 2017 44.733 - 2018 48.760 +4.027 (+9%) 2019 (primo trimestre) 12.290 +257 (+2%) Codici GIALLI 2018: 39,9% del totale accessi Tempo medio di attesa codici GIALLI 2018: 50 minuti Inteso come tempo accettazione triage – ingresso ambulatorio Età >=75 anno 2018: 33%
Ruolo dell’Infermiere di PS
INFERMIERE
AMBULATORIO
TRIAGE VISITA
Intervista Vie venose
Parametri vitali Monitoraggio
Protocolli Esami
Esami ?? FarmaciIdentificazione della SEPSI
Identificazione della SEPSI 2
La SEPSI è una patologia tempo dipendente
• Protocollo STEMI
• Protocollo STROKE
• Protocollo SEPSI ???
I malati con un punteggio SOFA ≥ 2 hanno un rischio
di mortalità circa del 10% di una popolazione
ospedaliera con presunta infezione.
(mortalità per STEMI circa 8%).
Seymour CW et al. JAMA. 2016;315(8):762-774Infermiere in Ambulatorio Visita • Team work (tempo dipendente) • Monitoraggio • Accessi venosi • Prelievi ematici • EGA • ECG • Emocolture • Somministrazione terapia • …
Matteo Guarino
Specializzando presso la Scuola di Medicina d'Emergenza – Urgenza
(Direttore: Prof. R. De Giorgio)
Azienda Ospedaliero - Universitaria S. Anna, Ferrara, ItaliaTHAM-THAM
(Tachypnea; Hypotension; Altered Mentation)
Matteo Guarino
Specializzando presso la Scuola di Medicina d'Emergenza – Urgenza
(Direttore: Prof. R. De Giorgio)
Azienda Ospedaliero - Universitaria S. Anna, Ferrara, ItaliaqSOFA – Score
Mortality is equal to about 1% for a
score equal to 0 and exceeds 20%
when the points are 3.
The score has a better
performance than the SIRS criteria
for predicting mortality in patients
with infection (AUROC of qSOFA
0.81 vs. AUROC of SIRS criteria
0.76) (PSinger M et al. The third international consensus definitions for sepsis and septic
shock (Sepsis-3). JAMA 2016;315(8):801-10Askim et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2017) 25:56
• qSOFA failed to detect two thirds of severe sepsis cases among
patients admitted to an ED with suspicion of infection.
• Further, the qSOFA failed to be a risk stratification tool as the
sensitivity to predict 7-day and 30-day mortality was low.
• RETTS-triage and the SIRS criteria showed a higher sensitivity vs
qSOFA.
• Since the ED not only should identify those who are critically ill of
sepsis at time of arrival, but also represent an important
identification point for those patients that are likely to become so.
Askim et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2017) 25:56…IN ADDITION…
qSOFA was specific but poorly sensitive for organ dysfunction (96.1%, 29.7% respectively)
SIRS was associated with organ dysfunction and mortality, and
abandoning the concept appears premature.
Although qSOFA≥2 showed high specificity, poor sensitivity may limit utility
as a bedside screen.
More prognostic and clinical information is conveyed using Sepsis-2
regarding number of organ dysfunctions.
The SOFA score may require recalibration.…AND EVEN MORE…
…AND EVEN MORE…
Modified qSOFA
• Systolic Blood Pressure ≤ 100 mmHg • 1 pt
• Change in mental status • 1 pt
• Respiratory Rate ≥ 22/min • 1 pt
• SpO2/FiO2 • 0 pt > 315
• 1 pt 314< S/FSpO2/FiO2
SpO2/FiO2
A STUDY PROPOSAL
(ricoveri da PS con diagnosi “sepsi/shock settico” aa 2017-2018)
Totale 1000
Maschi 461 (46,1%)
Femmine 539 (53,9%)
Deceduti 332 (33,2%)
Età 79,4±12,9
qSOFA 1,25±1
mqSOFA 1,74±1,54
LOS (dimessi vivi) 9,9±8,5
Dimessi Deceduti
(n=668) (n=332) P
Maschi 317 (47,5%) 144 (43,4%)
NS
Femmine 351 (52,5%) 188 (56,6%)
Età 77,9±13,6 82,4±10,6STREET recommendations • qSOFA non definisce la sepsi • qSOFA è una bandiera rossa per la sepsi e attiva delle azioni • qSOFA è più uno strumento di ricerca che per la pratica clinica ( in attesa del Spo2/Fio2?) • qSOFA non sostituisce gli EARLY WARNING SCORES, il monitoraggio al letto del malato e l’arte della Medicina
Puoi anche leggere