PAVIMENTO PELVICO PREVENZIONE PRE E POST-PARTUM - Milano 13 Dicembre 2019 Paola Pifarotti - Symposia Congressi
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
PAVIMENTO PELVICO
PREVENZIONE PRE E POST-PARTUM
Milano 13 Dicembre 2019
Paola Pifarotti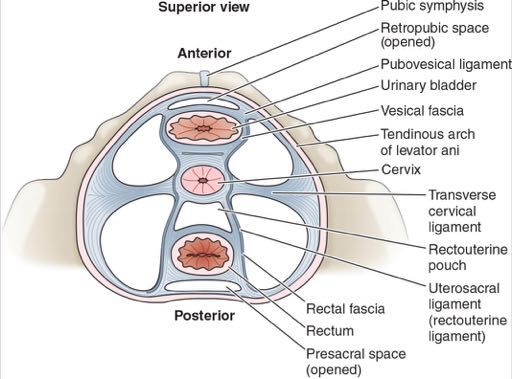
SOSTEGNO DEGLI ORGANI PELVICI muscoli del pavimento pelvico: Compartimento profondo: elevatori dell’ano (pubococcigei, ileococcigei, ischiococcigei)
SOSPENSIONE DEGLI ORGANI PELVICI fasce: fascia endopelvica (+vescico uretrovaginale, re6ovaginale)

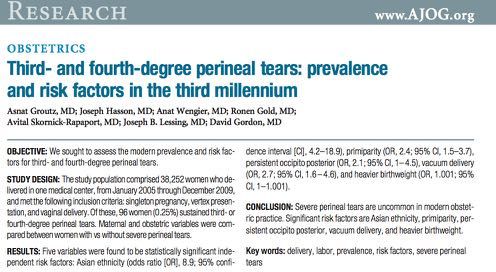
INTRODUCTION
Stress Urinary incontinence is the most common type of urinary incontinence in pregnant
women.
Detrimental effects on quality of life in approximately 54.3 % of all pregnant women.
SUI severity increase with pregnacy progression .
Pregnant women tend to consider this to be a common discomfort associated with
pregnancy and a consequence of childbirth in the post partum period.
PREVALENCE
The mean prevalence of SUI during pregnancy was 41% (25-75%), UUI
from 2% to35% and MUI from 3.8 to 13.1%.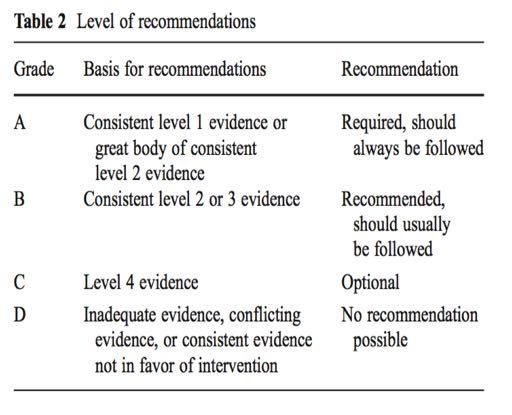
COMPONENTE MUSCOLARE e GRAVIDANZA
Studi MRI e US 3D mostrano progressiva riduzione del volume
muscolare:
AccentuaG da:
-riduzione superficie - Valsalva
-riduzione spessore - Stazioni fetali basse
Ulteriore decremento forza postparto: transitorio (ripr. entro 2 mesi)
Non chiarito se più vantaggioso:
-incremento forza muscolare: predispone a lacerazioni
-riduzione forza muscolare: predispone a stiramento delle strutture
connettivali, non completamente reversibile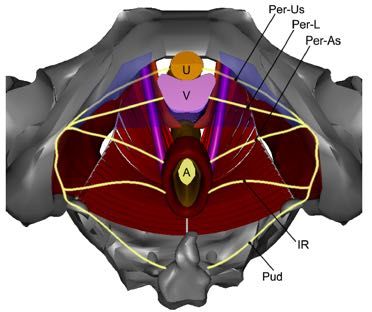
COMPONENTE CONNETTIVALE IN GRAVIDANZA aumento distensibilità con riduzione resistenza -lega4 a modificazione nella composizione del tessuto conne7vo: relaxina appare fa
HIATO GENITALE Ampiezze maggiori in: -origine degli elevatori ano solo da arco tendineo (predisposizione cos666va: 10% pz) -forza muscolare rido=a (elev. Ano) -gravidanze gemellari (distensione da fa=ore grava6vo) La gravidanza AUMENTA ampiezza di 30% (40% con Valsalva) Nel postparto PERSISTE distensione per il 70% a 4 mesi Ampiezze minori sono associate a > durata 2° stadio MA non chiara influenza su modalità finale parto
VESCICA / GIUNZIONE V.U. In gravidanza si osservano 1) dislocazione giunzione VU e modificazione angolo, con ev. ipermobilità: - lega? ad aumento lassità conne@vale (non muscolare) -origine endocrina + faDore grava?vo ØDislocazione GVU: aumenta con e.g. (1° trim.: 20% > 3° trim.: 40%), persiste fino a 6 mesi postparto ØIpermobilità durante Valsalva: in 30-40%; NON regredisce postparto
VESCICA / GIUNZIONE V.U. Possibili conseguenze: -frequenza/urgenza: da compressione (sopratt. 1°-3° trim.) -IUS: principalmente da ipermobilità, ev. contributo da compressione -ritenzione: meno freq., sopratt. fine 1° trim. > principalm. per effetto progesterone su detrusore, meno comumemente compressione GVU (solitamente cateterismo agevole)
RISK FACTORS FOR THE DEVELOPMENT OF SUI DURING PREGNANCY Epidemiological studies on UI during pregnancy show various factors associated with UI. Some risk factors like race, chronic disease, and fetal size are non-modifiable risk factors. However, several risk factors are modifiable and might promoted to prevent UI during pregnancy. AGE SUI during pregnancy is associated with advanced maternal age. OBESITY, HIGH BMI INDEX AND WEIGHT GAIN DURING PREGNANCY Obesity is the major risk factor that contributes to SUI during pregnancy. SMOKING Smoking contributes to the risk factors for SUI. CONSTIPATION Constipation during pregnancy is a common symptom (11%-38%)
RISK FACTORS FOR THE DEVELOPMENT OF SUI DURING PREGNANCY PRE-PREGNANCY STRESS URINARY INCONTINENCE Urine leakage prior a current pregnancy or in previous pregnancies could be a sign of poor quality of the connective tissue of the PFM GESTATIONAL DIABETES MELLITUS Women with DM are at greater riskof incontinence. Gestational Diabetes Mellitus is found to be and independent risk factor for UI postpartum with significant impact on QOL. PELVIC FLOOR MUSCLE EXERCISE PFME, the repetetively selective voluntary contraction and relaxation of specific PFM, is considered the first-line intervention of prevention and treatment for SUI during pregnancy before consideration of other treatments. A Cochrane review suggest that PFME is commonly recommended during pregnancy and postpartum for prevention and treatment of SUI.
Odds ratios for UI postpartum among women who were incontinent compared to women who were continent in pregnancy vary from 1.7 to 7.8 during the 3- to 12- month postpartum period. Incident UI postpartum is also a risk factor for UI even 12 years after delivery.
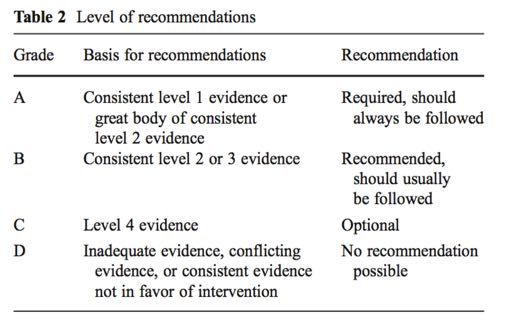
ACTION BEFORE ACTIONS DURING PREGNANCY
PREGNANCY
Constipation (grade B)
Smoking (grade B) Smoking (grade D)
Age (grade A) Caffeine (grade D)
Overweight (grade A) Crossed legs (grade D)
Bladder training (grade D)
Physical activity (grade B)
Pelvic floor muscle training (grade A)
Restricted weight gain (grade D)
Perineal massage (grade A)GRAVIDANZA-PARTO-PAVIMENTO PELVICO
+Multifactorial nature of obstetrical trauma
leading to pelvic floor disorders
Memon H. and Handa V, Women’s Health 2013There is little doubt that some women suffer significant trauma to pelvic floor
structures as a consequence of (successful or unsuccessful) attempts at vaginal
childbirth. Trauma might affect the pudendal nerve or its branches, the anal
sphincter, the puborectalis-pubococcygeus complex, and/or pelvic fascial structures.
Delivery-related pelvic floor trauma is a
reality, not a myth.
It is much less clear, however, whether such trauma is
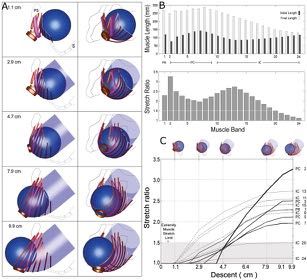
clinically relevantThe Biomechanics of Vaginal Birth and Common
Sequelae
12/01/14BIOMECHANICS OF THE LEVATOR MUSCLES
Ashton-Miller JA, Annu Rev Biomed Eng 2009MODIFICHE INDOTTE DAL PARTO Fenomeni di distensione cui possono seguire: -lacerazione -deformazione muscoloconne6vali non sempre reversibile (impa:o a l. termine di funzioni di supporto / sospensione) -ischemia (per even? prolunga?) -denervazione (danno n. pudendo / plesso lombosacrale con ripercussione su funzione muscolare e sostegno o con?nenza) Le alterazioni muscolari dire:e e da denervazione vengono recuperate per l’80-95% (denervazione: primi 2 mesi) Le alterazioni conne6vali sono meno facilmente reversibili
CONSEGUENZE A LUNGO TERMINE
Aumento rischio di IUS
Aumento rischio di POP
Aumento rischio di incon4nenza anale
Principali fa:ori predisponen4:
-composizione collagenica / resistenza muscolare cos4tuzionali
(lega4 sopra:. a fa:. gene4ci)
-addizione progressiva di alterazioni anatomofuzionali: maggiori
vs minoriURINARY INCONTINENECE
ETIOLOGY : multifactorial
ü SUI IS A COMMON CONDITION AFFECTING WOMEN WITH A NEGATIVE
INFLUENCE ON QOLà PREGNANCY AND IN PARTICULARLY VAGINAL DELIVERY
ARE IMPLICATED
Rotveit G, Urinary Incon;nence aMulticenter Study BJOG 2006 Only maternal age and method of delivery are associated with the risk of incontinence after delivery. Forceps and vacuum delivery are not significatetively associated with UI.
CONSEGUENZA A LUNGO TERMINE
POP:
FDR: ruolo principale di f.d.r. aggiuntivi (età, obesità); ostetrici:
gravidanza, parto operativo, LBW
Disfunz. sessuale:
spesso associata a lesioni alto grado pav. pelvico (OASIS)
TC NON è protettivo se non in parte:
grande quota di aumento rischio è legata a modificazioni gravidiche,
Protettivo solo a breve terminaLongitudinal Cohort Study 1011 women classified as CS without labor, CS during active labor, CS after complete cervical dilatation, spontaneous vaginal birth,or operative vaginal birth.
Cohort Study
Communit
y-based
Study
N Eng J Med 2013
15307 women enrolled in Epidemiology of Incontinece in the Country
of Nord-Trodelag (EPICONT)2625 Perimenopausal women (GAZEL cohort) The prevalence of severe SUI in this population of perimenopausal women was 15%. Significant risk factors were BMI, DIABETES, INCONTINENCE SURGERY,PARITY and YOUTHFUL DELIVERY (age less than 22 years). No protective effect against SUI by cesarean section was found.
Registry-based national
cohort study
BJOG 2012
5236 Singleton primiparae who delivered in the period 1985–1988 with no further births
- Two decades aAer one birth, vaginal delivery was associated with a 67%
increased risk of UI, and UI > 10 years increased by 275% compared with
caesarean secKon.
- It is necessary to perform eight or nine cesarean secKons to avoid one case of UI.
- Weight control is an important prophylacKc measure to reduce UI. Current BMI
was the most important BMI-determinant for UI, which is important, as BMI is
modifiable.2009
ANAL INCONTINENCE
PREVENZIONE Suggerita possibile u/lità di interven/ anteparto in protezione pavimento pelvico: 1) EpiNo: Validità diba=uta: - certamente sicuro, aumenta sicurezza donne a parto - non certezze su sua effeAva efficacia preven/va; verosimile impa=o minore
PREVENZIONE
2) Esercizi pav. pelvico:
-non evidenti differenze rispetto ad esiti principali pav. pelvico al
parto (2° stadio più breve, no riduzione lesioni)
MA
- minore frequenza / gravità IUS in gravidanza e nel post-partum
- non influenza su inc. anale
3) Massaggi perineali:
- riduzione durata 2° stadio, ma NO apparente protezione da lesioni
intraparto (dati contrastanti);
- riduzione dolore postpartoCONCLUSIONI ØCI SONO EVIDENZE CHE LA PERCENTUALE DI IUS DOPO CESAREO ELETTIVO E’PIU’ BASSA DI QUELLA OSSERVATA DOPO UN PARTO VAGINALE Ø IL TAGLIO CESAREO FORNISCE UNA PARZIALE PROTEZIONE DALLA IUS Ø PER QUANTO RIGUARDA LA PREVENZIONE DI UN DANNO DA PARTO IL RISCHIO/BENEFICIO NON CI PERMETTE DI PROPORRE UN TAGLIO CESAREO ELETTIVO
CONCLUSIONI LA GRAVIDANZA DA SOLA E’ UN FATTORE DI RISCHIO IL PARTO VAGINALE E’ ASSOCIATO AL POSSIBILE SVILUPPO DI DANNI PERINEALI MA IL SINTOMO SI MANIFESTA IN BASE ALLA SUSCETTIBILITA’ INDIVIDUALE L’OBESITA’ E L’ETA’ MATERNA COSTITUISCONO IMPORTANTI FATTORI DI RISCHIO PER LO SVILUPPO DELLA IUS DURANTE E DOPO LA GRAVIDANZA PER RENDERE FATTIBILE UNA PREVENZIONE E’ IMPORTANTE IDENTIFICARE LA POPOLAZIONE A RISCHIO E RIDURRE QUESTO IMPORTANTE PROBLEMA CHE ALTERA LA QUALITA’ DI VITA DELLE DONNE
Puoi anche leggere