OLV NEL BPCO SEVERO Prof. FRANCESCO PUGLIESE UOD Anestesia e Terapia Intensiva Trapianti d' Organo Policlinico Umberto I Roma - Siaarti
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

OLV NEL BPCO SEVERO
Prof. FRANCESCO PUGLIESE
UOD Anestesia e Terapia Intensiva Trapianti d’ Organo
Policlinico Umberto I Roma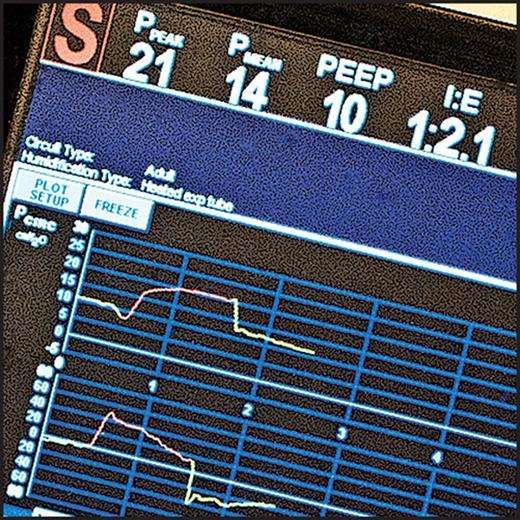
BPCO ENFISEMA, ASMA, BRONCHIECTASIE, BROCHIOLITI
1990: SESTA CAUSA DI MORTE
…2020: TERZA CAUSA DI MORTE
Mechanical ventilation in patients with chronic obstructive pulmonary disease and bronchial asthma
Syed Moied A, Manazir A Indian Journal of Anaesthesia 2015
PROGRESSIVO AUMENTO DEI PAZIENTI BPCO SOTTOPOSTI A CHIRURGIA
AUMENTATO RISCHIO CHIRURGICO
Fase clinica BPCO È indice di un’importante
riduzione della funzione
e di una prognosi
sfavorevole. Quando il
FEV1 è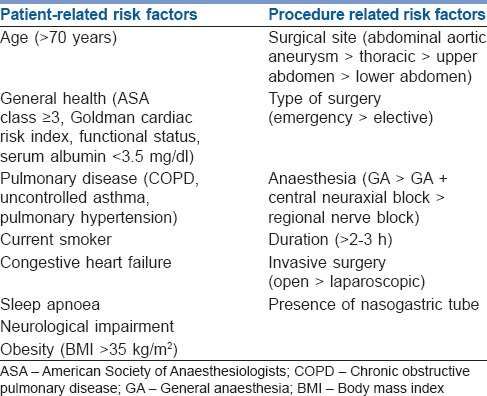
Entità dell’ostruzione Segni e sintomi Alterazioni funzionali
FEV1
(% del teorico)
Alterazioni funzionali di limitato valore clinico:
80 • Frequenza-dipendenza della compliance
• Aumento del volume di chiusura e dell’N2-slope
Tosse del fumatore • Riduzione del potere di ritorno elastico
Lieve • Modesta riduzione degli indici di espirazione forzata
Assenza di segni anomali
60
Dispnea/fischi e sibili da sforzo • Riduzione del FEV1 (attorno al 50%)
Moderata Tosse con espettorazione • Aumento della CFR e riduzione della DLCO
• Comparsa di un variabile grado di ipossiemia
(in presenza di normocapnia)
40
Accentuazione della dispnea
Saltuariamente: fischi e sibili a riposo • Grave limitazione al flusso aereo (FEV1
Fattori di rischio indipendenti delle complicanze polmonari nel post-operatorio

LIMITAZIONE FLUSSO ESPIRATORIO Aumento del flusso inspiratorio AUMENTO DELLA FATICA MUSCOLARE
Aumento del volume polmonare
IPERINFLAZIONE DINAMICA Air trapping
Aumento della pressione intratoracica
Aumento del work of breathing
AUTO-PEEP
…”Furthermore, during OLV in lateral decubitus, the compression atelectasis of dependent lung regions,
the loss of elastic recoil after thoracotomy, and mediastinal surgical manipulations can markedly reduce
the aerated lung capacity, impair ventilation distribution, and worsen ventilation/perfusion mismatch”
Ann Thorac Med. 2014.
Pressure-controlled versus volume-controlled ventilation during one-lung ventilation in
elderly patients with poor pulmonary function
Fei Lin, Linghui Pan, Bin Huang, Lin Ruan, Rui Liang, Wei Qian and Wanyun Ge
Ann Thorac Med 2014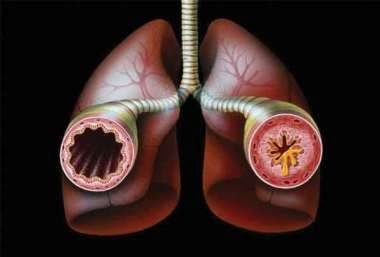
ZONE DI WEST
PAZIENTE SVEGLIO:
DISTRIBUZIONE IN POSIZIONE LATERALE
SIMILE A QUELLA IN POSIZIONE ORTOSTATICA
DOPO INDUZIONE DELL’ ANESTESIA:
IL POLMONE PROCLIVE SI SPOSTA
VERSO UNA ZONA PIU’ COMPLIANTE, MENTRE
IL POLMONE DECLIVE SI SPOSTA
VERSO UNA ZONA MENO COMPLIANTE, PIU’ PIATTA,
DELLA CURVA PRESSIONE/VOLUME
L’ APERTURA DEL TORACE AUMENTA LA
COMPLIANCE DEL POLMONE NON DIPENDENTE
CHE, INSIEME ALL’ AUMENTATA PRESSIONE
ADDOMINALE (PAB) DIRETTA SUL POLMONE
INFERIORE DOPO PARALISI MUSCOLARE
DIAFRAMMATICA, DIRIGE LA MAGGIOR PARTE
DEL VOLUME CORRENTE VERSO IL POLMONE
SUPERIORE
Distribuzione della ventilazione in relazione alla posizione e alle varie fasi dell’ intervento
CONTRASTARE L’ IPERINFLAZIONE POLMONARE
RIDURRE LA PEEP INTRINSECA
RIDURRE L’ IPERCAPNIA !!!????
QUALI STRATEGIE?
PEEP
RECLUTAMENTO ALVEOLARE
VCV/PCV
I:EPEEP: SI? NO? QUANTA? - EFFETTO SOMMATORIO DELLA PEEP CON LA PEEP INTRINSECA - SPESSO NECESSARIA, NON FONDAMENTALE, TALVOLTA DELETERIA - RISCHIO DI IPOSSIA PER VALORI ECCESSIVI DI PEEP - NON IMPOSTARLA IN MANIERA EMPIRICA - CALCOLARE LA ‘’BEST PEEP’’ Setting Individualized Positive End-Expiratory Pressure Level with a Positive End- Expiratory Pressure Decrement Trial After a Recruitment Maneuver Improves Oxygenation and Lung Mechanics During One-Lung Ventilation. Carlos Ferrando et al. Anesth Analg 2014;118:657–65 Amato M. et al. Driving Pressure and Survival in the Acute Respiratory Distress Syndrome.N Engl J Med 2015;372:747-55.
RECLUTAMENTO ALVEOLARE
Il paziente BPCO presenta una
SCARSA TENDENZA ALLE ATELETTASIE ed una
ELEVATA COMPLIANCE
Tuttavia, la OLV e la chirurgia stessa possono
aumentare il rischio di atelettasie
Non considerare questa strategia come primo
step percorribile
Setting Individualized Positive End-Expiratory Pressure Level with a Positive End- Recruitment maneuvers in acute respiratory distress syndrome: the safe
Expiratory Pressure Decrement Trial After a Recruitment Maneuver Improves Oxygenation way in the best way
and Lung Mechanics During One-Lung Ventilation. Santos RS, Silva PL, Pelosi P, Rocco PR
Carlos Ferrando et al. Anesth Analg 2014;118:657–65 World J Crit Care Med 2015 ReviewRECLUTAMENTO ALVEOLARE: Si? No? Come? Quanto?
Diverse strategie proposte, ma nessuna validata in Letteratura
TALVOLTA NECESSARIA, NON FONDAMENTALE. DELETERIA?
Aumentato rischio di instabilità emodinamica da incremento della pressione intratoracica
Rischio di danneggiamento del parenchima polmonare (barotrauma, sovradistensione)
Setting Individualized Positive End-Expiratory Pressure Level with a Recruitment maneuvers in acute respiratory distress syndrome: the safe way in the
Positive End-Expiratory Pressure Decrement Trial After a Recruitment best way
Maneuver Improves Oxygenation and Lung Mechanics During One-Lung Santos RS, Silva PL, Pelosi P, Rocco PR
Ventilation. World J Crit Care Med 2015 Review
Carlos Ferrando et al. Anesth Analg 2014;118:657–65SOVRADISTENSIONE
SHIFT MEDIASTINICO
ATELETTASIE INSTABILITA’ EMODINAMICA
IPOVENTILAZIONE
SHUNT
…E LA PRESSIONE DI PERFUSIONE????
ATTENZIONE ALLE ZONE DI WEST!!!!!!!!!!!PCV/VCV
DIBATTITO APERTO
Volume-controlled versus pressure-controlled ventilation-volume guaranteed mode during one-lung ventilation.
Song SY, Jung JY, Cho MS, Kim JH, Ryu TH, Kim BI. Korean J Anesthesiol 2014
“…In conclusion, the PCV-VG mode did not provide
significantly improved oxygenation compared with the
VCV mode during OLV for patients with normal
pulmonary function. However, this ventilation mode
during OLV attenuated airway pressure despite the
increase tidal volume compared with the VCV mode.”PCV/VCV DURANTE OLV, RECENTI STUDI AVVALORANO L’ EFFICACIA DELLA PCV NEL PAZIENTE ANZIANO CON FUNZIONALITA’ RESPIRATORIA COMPROMESSA. Pressure-controlled versus volume-controlled ventilation during one-lung ventilation in elderly patients with poor pulmonary function Fei Lin, Linghui Pan, Bin Huang, Lin Ruan, Rui Liang, Wei Qian and Wanyun Ge Ann Thorac Med 2014 “The patients were enrolled into the study having poor pulmonary function (forced expiratory volume in 1 s
VENTILAZIONE MONOPOLMONARE PROTETTIVA
PROPOSTA DA QUALCHE ANNO
DIBATTITO APERTO
Low tidal volume is indicated during one-lung ventilation
Slinger P et al Anesth Analg 2006
Is small tidal volume with low positive end expiratory pressure during one-lung ventilation an
effective ventilation method for endoscopic thoracic surgery?
Yun du G et al. Korean J Anesthesiol 2014
Noninvasive Measurement of Carbon Dioxide during One-Lung Ventilation with Low Tidal Volume for
Two Hours: End-Tidal versus Transcutaneous Techniques
Zang H et al PLoS One 2015Intraoperative mechanical ventilation strategies for one-lung ventilation
Senturk M, Slinger P, Cohen E Best Practice & Research Clinical Anaesthesiology September 2015
…”With respect to oxygenation, some studies have found
no relevant difference in oxygenation between low and
high TV, whilst some studies have found a significant
difference in favour of a higher TV. However, one of the
most important reasons for both hypoxaemia and ALI is
the decline of functional residual capacity (FRC) below the
closing capacity (CC) and a high TV cannot be the
solution of this main problem.”
Relationship of FRC (functional residual capacity) and CC (closing
capacity) in different ventilatory settings. Right: FRC falls below CC during
mechanical ventilation; a larger tidal volume (TV) can obtain better gas
exchange (note the larger area above the CC line); however, a cyclic
recruitment cannot be avoided. Left: Applying PEEP while keeping the TV
low: PEEP obtains an FRC above the CC. Cyclic recruitment is avoided,
and the ventilation (now the area above the ‘new’ FRC) is still better than
the one without PEEP.“…How ‘low’ is ‘low enough’? A TV of 6–8 mL/kg is considered ‘protective’ for two-lung ventilation. When applied to only one lung, this would indicate a doubly high value, which may not be protective anymore. However, halving the TV again to 3– 4 mL/kg would descend below dead-space ventilation. Empirically, a TV of 5–6 mL/kg seems rational, but this needs to be proven.” Intraoperative mechanical ventilation strategies for one-lung ventilation Senturk M, Slinger P, Cohen E Best Practice & Research Clinical Anaesthesiology September 2015
I:E
Adeguare il rapporto I:E in base agli obiettivi clinici:
Miglioramento dell’ ossigenazione
Limitazione dell’ iperinflazione dinamica
Limitazione dell’ ipercapnia
Difficoltà di impostazione di un adeguato rapporto
I:E in un paziente ‘’ostruttivo esposto a condizioni restrittive’’RIASSUMENDO Best PEEP RECLUTAMENTO PCV/VCV NECESSARIO UN COSTANTE AGGIORNAMENTO SULLE INNOVAZIONI TECNOLOGICHE QUALI STRATEGIE PER IL FUTURO?
Thoracic epidural anaesthesia for awake thoracic surgery in severely dyspnoeic patients excluded from general anaesthesia
Gabor Kissa,*, Antoine Claretb, Jacques Desbordesa and Henri Porteb Interactive CardioVascular and Thoracic Surgery 19 (2014)
POSSIBILE UTILIZZO DI DECAP IN PAZIENTE IPERCAPNICO
Low-flow veno-venous extracorporeal CO2 removal: first clinical experience in lung transplant recipients
Ruberto F, Bergantino B, Testa MC, D’Arena C, Bernardinetti M, Diso D, De Giacomo T, Venuta F, Pugliese F
Int J Artif Organs 2014
“…We employed a new device (ProLUNG) recently introduced into the clinical arsenal that exploits a simple
hemoperfusion technique sustained by blood flows lower than 500 ml/min to remove CO 2 from the venous
blood. It was used as an adjunctive support to mechanical ventilation during and after four lung
transplantations in our center.”Puoi anche leggere