NAO IN PARTICOLARI SETTING: PAZIENTE FRAGILE E ANZIANO - PHD, MD SERGIO AGOSTI DIR. MEDICO CARDIOLOGO - CARDIO ALESSANDRIA
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

NAO in particolari
setting: paziente
fragile e anziano
PhD, MD Sergio Agosti
Dir. Medico Cardiologo
Ospedale San Giacomo, Novi Ligure
Prof. a contratto Università di Genova
Comitato scientifico nazionale
Fondazione Obiettivo Cuore, ARCA
DISCLOSURE INFORMATION
Agosti Sergio
negli ultimi due anni ho avuto i seguenti rapporti anche di
finanziamento con soggetti portatori di interessi
commerciali in campo sanitario:
Bayer
BMS/Pfizer
Boehringer
Daiichi-Sankyo
Sanofi
Amgen
Piam
Servier
Wynford Eagle

Thomas Sydenham, 1624 – 1689
“Primum Non Nocere”
Nelle nostra scelta prevale quasi sempre la riduzione del
rischio emorragico rispetto al rischio tromboembolico
SCELTA DI SICUREZZA
Journal of Clinical Pharmacology, 2005;45:371-377
Q13: Nella scelta di un NAO quanto pesano le seguenti
caratteristiche?
pochissimo poco abbastanza molto moltissimo
ARCA Liguria NAO Survey: our results. Sergio Agosti, Laura Casalino, Bruno Tarabella, Mauro
Barra, Raffaele Griffo, Giovanni Battista Zito et al. CARDIOLOGIA AMBULATORIALE, 2016, 4:
247-257
MAJOR BLEEDING
NOACs associated with a non significant RRR of 14%
compared to Warfarin
Ruff CT, Lancet, December 4, 2013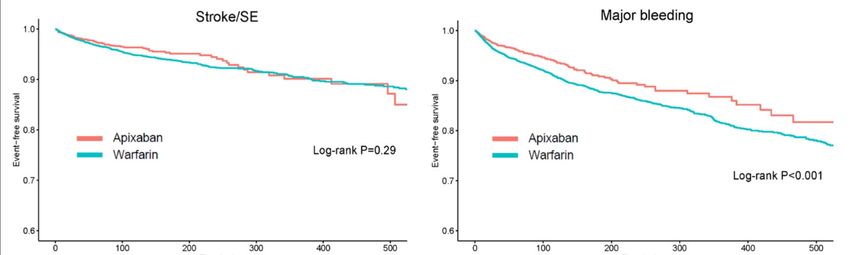
Haemorrhagic stroke
60% RRR
Intracranial hemorrhage risk with the new oral anticoagulants: a
systematic review and meta analysis Daniel Caldeira et al. J
Neurol 2014DOACs in the older persons with atrial fibrillation.
DOAC WARFARIN
>75 anni
Malik AH, Yandrapalli S, Aronow WS, et al. Meta-Analysis of Direct-Acting Oral
Anticoagulants Compared With Warfarin in Patients > 75 Years of Age. Am J Cardiol
2019;123(12):2051–7.DOAC vs Warfarin Vendite a totale Italia
DOACs e sicurezza… •DOACs e fragilità… •DOACs e bassi dosaggi… •DOACs ed insufficienza renale…
DOACs e sicurezza… •DOACs e fragilità… •DOACs e bassi dosaggi… •DOACs ed insufficienza renale…
Malattia
Stato funzionale Livello cognitivo
Stato Supporto
Ambiente di salute psicoaffettivo
Condizioni
Rete sociale
economicheCONCETTO DI FRAGILITA’
andatura lenta
scarsa attività fisica
“Fenotipo fragile”
perdita peso involontario
3 su 5 criteri
riferita astenia
riferita debolezza muscolare
Associato a peggioramento disabilità, ospedalizzazione e mortalità a 7 anniBo M. Practical use of Direct Oral Anti Coagulants (DOACs) in the older persons with atrial brillation. Eur J Intern Med 2019
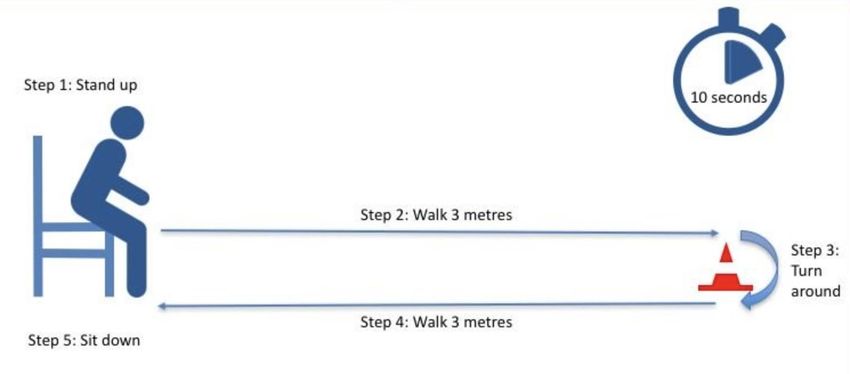
TUG Test Timed Up and Go Test
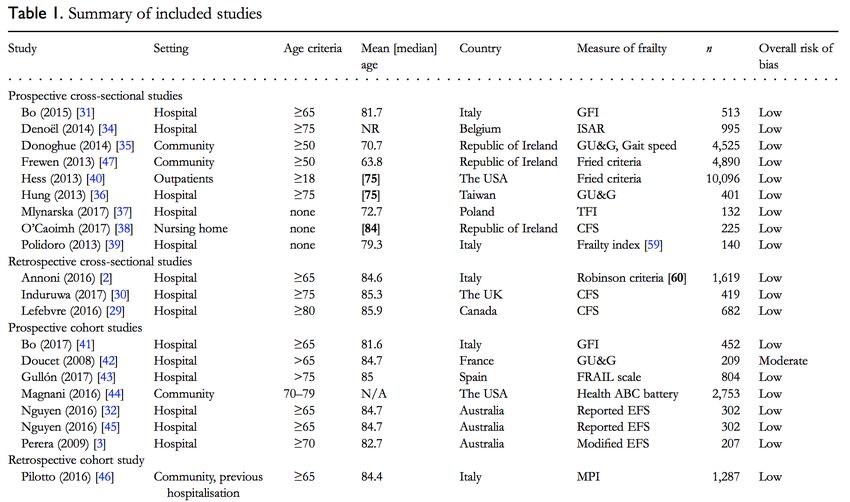
20 studi osservazionali
31 mila pazienti
Wilkinson C, Todd O, Clegg A, et al. Management of atrial brillation for older people with
frailty: a systematic review and meta-analysis. Age Ageing 2019;48(2):196–203.Riduzione prescrizione TAO nei pazienti con fragilità
timore sicurezza DOACs nel 5-20%
fino al 50%
paura cadute dei pazienti in TAO
difficoltà gestione
Nei pazienti con FA, la fragilità è associata a maggior rischio di
stroke durata ospedalizzazione
mortalità severità dei sintomi>75 anni PattiG,PecenL,LucernaM,etal.NetClinicalBene tofNon-VitaminKAntagonist vs Vitamin K Antagonist Anticoagulants in Elderly Patients with Atrial Fibrillation. Am J Med 2019;132(6):749–57
DOACs e sicurezza… •DOACs e fragilità… •DOACs e bassi dosaggi… •DOACs ed insufficienza renale…
BASSI DOSI DI DOAC PER «PROTEGGERE» DAL RISCHIO EMORRAGICO
Qual è la situazione italiana?
Dati IMS utilizzo di DOAC nel 2017
dabigatran apixaban rivaroxaban edoxaban
38,1% 36,3% 41,6%
42,2%
57,8% 61,9% 63,7% 58,4%
Dabigatran 110 mg Apixaban 2.5 mg Rivaroxaban 15 mg Edoxaban 30 mg
Dabigatran 150 mg Apixaban 5 mg Rivaroxaban 20 mg Edoxaban 60 mg
Nella realtà italiana, il medico ricorre al «basso dosaggio»
in oltre il 37% dei pazientiDifferences between the four NOAC randomized controlled trials
that impact the robustness of cross-study comparisons
Challenges in comparing the non-vitamin K antagonist oral anticoagulants for atriale
fibrillation-related stroke prevention. Camm AJ, Fox KAA, Peterson E. Europace. 2017 Oct 13.G Ital Cardiol 2017;18(9 Suppl 2):3S-9
DOACs e sicurezza… •DOACs e fragilità… •DOACs e bassi dosaggi… •DOACs ed insufficienza renale…
stroke or systemic embolism
major bleeding
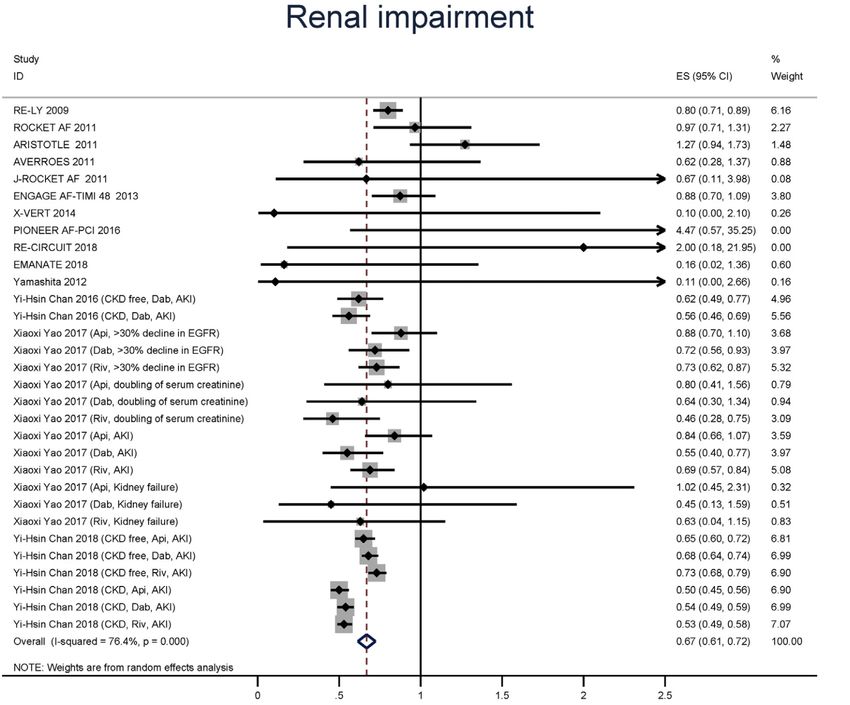
The American Journal of Medicine, Vol 130, No 9, September 2017Raccomandazioni dell’EHRA nei pazienti con IR (2018)
190 mila pazienti, 11 trials e 3 registri…
Thrombosis research 174 (2019) 16-23Thrombosis research 174 (2019) 16-23
XARENO – An Ongoing Real-World Study
of Rivaroxaban in Renally Impaired Patients
Official study title: Factor XA – inhibition in RENal patients with non-valvular atrial fibrillation Observational registry
Objective: To assess CKD progression and safety of anticoagulation strategies in NVAF patients with eGFR 15–49 ml/min /1.73 m2 in
routine clinical practice
Pre-study phase Follow-up phase Investigators to collect data at initial
visit, at 3 months and then quarterly
Rivaroxaban for
≥3 months n≥1000
Patient
Study selection and VKA
population: choice of type, for ≥3 months n≥1000
dose and
Patients with duration of drug
NVAF (N=2500) used at
and eGFR/CrCl discretion of
15–49 ml/min attending
physician
No OAC (ASA or
no treatment) nAXADIA: A Safety Study Assessing Oral Anticoagulation With Apixaban Versus Vitamin-K Antagonists in Patients With Atrial Fibrillation and End- Stage Kidney Disease on Chronic Hemodialysis Treatment Detailed Description: AXADIA is an investigator‐driven, prospective, parallel‐group, single country, multi‐center phase IIIb trial to assess the safety of apixaban versus the vitamin-K antagonist phenprocoumon in patients with NVAF and ESKD on hemodialysis treatment. The trial will be conducted in about 25-30 sites in Germany and will enroll about 220 patients Primary goal: to assess the safety of two types of oral anticoagulants in patients with ESKD on hemodialysis with non-valvular atrial fibrillation (NVAF). The novel FXa inhibitor apixaban (at a reduced dose of 2x 2.5 mg/day) will be compared to the vitamin-K antagonist (VKA) phenprocoumon (target range: International Normalized Ratio (INR) 2.0-3.0) regarding bleeding rates during chronic administration for prevention of stroke or systemic embolism. The primary hypothesis: oral anticoagulation with apixaban will improve the safety by significantly reducing bleeding rates in patients with ESKD on hemodialysis and NVAF compared to the VKA phenprocoumon. A pharmacokinetic sub-study will be performed with 28 patients included in the apixaban treatment group to evaluate the systemic exposure of apixaban before and after hemodialysis session in this special population. ClinicalTrials.gov Identifier: NCT02933697
RENAL-AF: RENal hemodialysis patients ALlocated
apixaban versus warfarin in Atrial Fibrillation patients
Selected inclusion criteria Selected exclusion criteria
• Atrial fibrillation • Moderate or severe mitral stenosis
• CHA2DS2-VASc ≥2 • OAC needed for reason other than AF
Randomize
• Hemodialysis • Need for aspirin > 81 mg
• Candidate for OAC • Need for dual antiplatelet therapy
• Life expectancy < 3 months
Apixaban 5 mg oral twice daily Warfarin
(2.5 mg BID in selected patients) (target INR 2–3)
Open label with blinded event adjudication
Primary outcome: ISTH major and clinically relevant non-major
bleeding
Secondary outcomes:
• PK in patients randomized to apixaban
• Stroke and systemic embolism
• Death
• Tolerability/persistence/adherence parameters
Sponsor: Christopher Granger, Duke University Medical Center Philadelphia, 16-18 Nov 2019Apixaban and Warfarin Dosing in Modified ITT
Patients randomized to apixaban and received at least one dose Apixaban N = 77
First apixaban dose
2.5 mg BID 22 (28.6%)
5.0 mg BID 55 (71.4%)
Aspirin 29 (36.7%)
Patients randomized to warfarin and received at least one dose Warfarin N = 68
Time in therapeutic range (2.0-3.0), Median (Q1, Q3)1 44.3% (23.2%, 59.0%)
• Patients were 3 times as likely to be subtherapeutic (INR 3.0)
Total
Randomized
1 Time in therapeutic range was calculated by the Rosendaal method
N=154Time to Major or Clinically Relevant Non-
Major Bleed for Intention to Treat
Event 5.0% 15.3% 20.7% 24.2% 31.5%
Rates: 4.3% 8.7% 16.6% 20.6% 25.5%
Apixaban
Warfarin
HR (95% CI):
1.20 (0.63, 2.30)Retrospettivo, 25mila pt
Circulation. Oct. 2018;138:1519–1529Retrospettivo, 25mila pt
Circulation. Oct. 2018;138:1519–1529CONCLUSIONI • Sicurezza è determinante principale nella scelta TAO • Riconoscere “Fenotipo Fragile”, paziente a maggior rischio ischemico ed emorragico, ma meno trattato • DOACs presentano beneficio clinico netto migliore di VKA nei pazienti anziani •Over prescrizione bassi dosaggi non del tutto motivata • Insufficienza renale non è un limite alla prescrizione dei DOACs, apertura a cl cr
www.arcaliguria.it
GRAZIE PER L’ATTENZIONE
www.agostisergio.itPuoi anche leggere