La Sindrome della Enterocolite Allergica (detta anche FPIES)
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

La Sindrome della Enterocolite Allergica
(detta anche FPIES)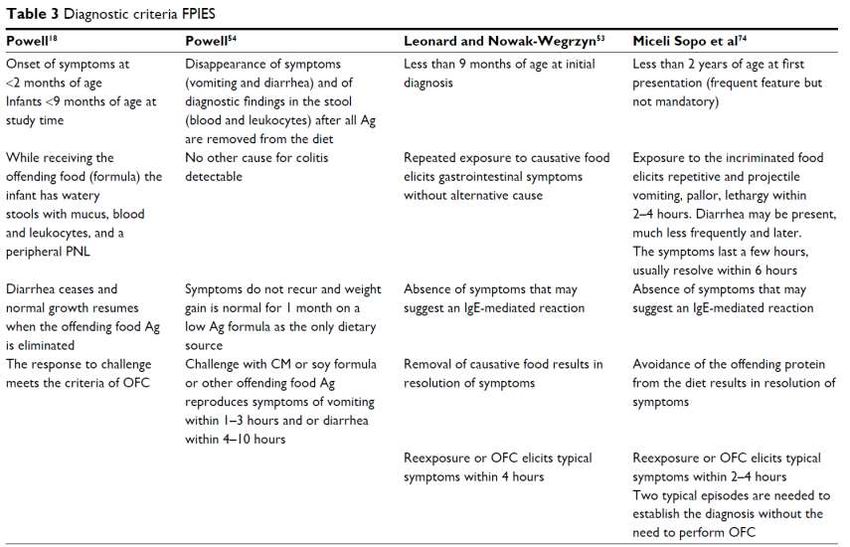
Lo fareste? - 1
Sarà SEA quella di Roberto?
• Conosco Roberto, 18 mesi, un giovedì di fine Settembre, mi racconta che …
• All’ età di 9 mesi aveva mangiato del merluzzo (circa 50 grammi) e dopo 2 ore
aveva ripetutamente vomitato per 3-4 ore (no pallore, no letargia, no diarrea).
Dopo i vomiti le condizioni tornavano normali.
• In precedenza aveva mangiato il merluzzo nello stesso quantitativo 3-4 volte
senza presentare reazioni avverse.
• Dopo circa un mese da quell’ episodio, aveva mangiato al nido circa 50 grammi
di limanda (famiglia della sogliola, ma pur sempre un pesce come il merluzzo)
e dopo 2 ore ha presentato un episodio analogo al precedente.
• Questa estate ha mangiato piccolissime quantità di tonno in scatola e di cozze-
vongole senza presentare reazioni avverse.
Lo fareste? - 2
Sarà SEA quella di Roberto?
• Il prick test con merluzzo cotto ed estratto di merluzzo è risultato negativo
• Le domande sono:
1. Fareste un TPO diagnostico (cioè a breve, diciamo entro un mese)?
2. Oppure ritenete che la diagnosi definitiva di SEA sia emettibile già con quello
che sappiamo fino ad ora?
3. O siete sicuri che non è nulla e dite a Roberto di andarsi a mangiare un bel
rombo al forno con patate?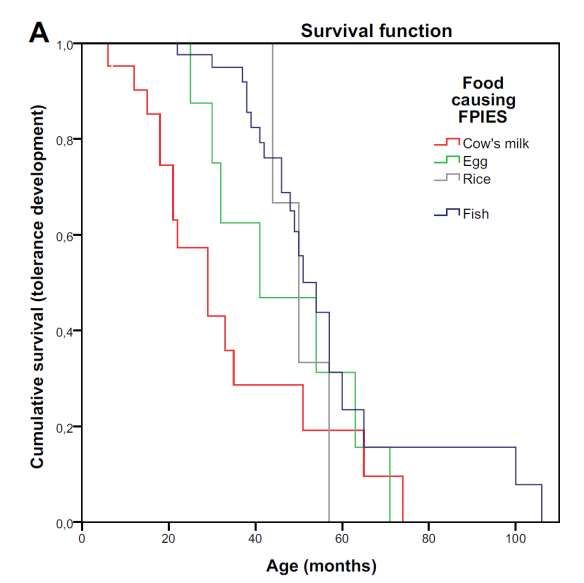
Lo fareste? - 3
Sarà SEA quella di Rebecca?
• Il giorno di San Bruno ho conosciuto Rebecca.
• Nel Maggio precedente la bimba, che allora aveva 8 mesi, ha assunto a pranzo
un tuorlo d’ uovo alla coque e poi è andata a dormire.
• Dopo circa 1 ora i genitori l’ hanno trovata cosparsa del suo vomito. Rebecca
ha poi vomitato altre 3 volte, appariva pallida e letargica, ha presentato una
evacuazione diarroica ed è stata condotta in pronto soccorso.
• Qui ha presentato un altro vomito, è stata posizionata fleboclisi reidratante e
sono stati eseguiti esami ematochimici i quali hanno documentato leucocitosi
neutrofila (28.990/mmc, neutrofili 65%, linfociti 22%) e piastrinosi
(605.000/mmc) in riduzione il giorno dopo (globuli bianchi 10.470/mmc,
piastrine 531.000/mmc), la bambina è stata ricoverata in osservazione breve
intensiva (OBI).Lo fareste? - 4
Sarà SEA quella di Rebecca?
• L’ esame obiettivo era normale, tempo di refill circa 2 secondi.
• Saturazione di ossigeno = 98%, non sono state rilevate né la pressione
arteriosa né la temperatura.
• Non è chiaro quando la bambina sia tornata “normale”, cioè dopo quante ore,
di certo non ha vomitato più dopo le 20 e la mattina dopo stava bene.Lo fareste? - 5
Sarà SEA quella di Rebecca?
• La storia documenta almeno 3 precedenti e innocue assunzioni di tuorlo (e
probabilmente piccoli frammenti di albume) tra i 7 e 8 mesi, cotto alla coque,
in quantità progressivamente crescenti.
• Alla dimissione dall’ OBI è stato suggerito di risomministrare l’ uovo il
mercoledì successivo e se i sintomi si fossero ripetuti i genitori avrebbero
dovuto prenotare una visita allergologica.
• I genitori, sentita la pediatra di famiglia, non hanno risomministrato l’ uovo
“assoluto”.
• In verità, Rebecca, che adesso ha 13 mesi, ha assunto piccole quantità di uovo
attraverso biscotti (anche se ha mangiato più spesso biscotti Plasmon che non
contengono uovo), gelato fiordilatte (che non dovrebbe avere uovo nel suo
interno), e pezzettini di frittata grandi al massimo quanto mezzo cucchiaino di
caffè.
• E non ha presentato mai più episodi come quello del 27/5/2016.Lo fareste? - 6
Sarà SEA quella di Rebecca?
• I prick test con uovo crudo, estratto di albume ed estratto di tuorlo sono
risultati negativi.
• Le domande sono:
1. Fareste un TPO diagnostico (cioè a breve, diciamo entro un mese)?
2. Oppure ritenete che la diagnosi definitiva di SEA sia emettibile già con quello
che sappiamo fino ad ora?
3. O siete sicuri che non è nulla e dite a Rebecca di andarsi a mangiare una
frittata con cipolle?Per decidere con consapevolezza • Circa Roberto e Rebecca • Non sarebbe male avere a disposizione un aiutino • Ad esempio, sotto forma di criteri diagnostici a cui poter fare riferimento • Del tutto recentemente, Michelet ne ha riassunti alcuni
Una sintesi al 2017 Michelet et al, J Asth All 2017 1986
Jean-Cristophe nel 2014
Caubet et al, JACI 2014
• The diagnosis of FPIES was based on Powell’s clinical criteria (2,19):
• exposure to the incriminated food elicits repetitive vomiting, diarrhea, or both within
4 hours without any other cause for the symptoms;
• symptoms are limited to the gastrointestinal tract;
• avoidance of the offending protein from the diet results in resolution of symptoms;
• and a standardized OFC or isolated re-exposure elicits the typical symptoms.
• La voce bibliografica n. 2 corrisponde a Sicherer SH. Food protein-induced
enterocolitis syndrome: case presentations and management lessons. J
Allergy Clin Immunol 2005;115:149-56.
• La voce bibliografica n. 19 corrisponde Powell GK. Food protein-induced
enterocolitis of infancy: differential diagnosis and management. Compr Ther
1986;12:28-37.JCC e SMS
da Gmail, 8 agosto 2017
• Dear Jean-Cristophe, I asked you for the paper you kindly sent me because in
your 2014 paper (attached) you mention FPIES diagnostic criteria and assign
them to Powell 1986 and Sicherer 2005 (both attached). I do not think that it
is: Powell in 1986 still refers to the chronic form of FPIES and Sicherer in
2005 refer to Powell 1986. Then I'll ask you, "Who has drawn up the criteria
you mention in 2014?" They really were the most used ones until a few years
ago. In short, does diagnostic criteria for acute FPIES having longer duration
do not have paternity?
• Dear Stefano, Those criteria were used for the study at Mount Sinai. Indeed,
they are based on previously published criteria (Powell 78 and 86, Sicherer
2005, Leonard 2012...). But now, anyway, we will use the new diagnostic
criteria published in the International guidelines...I più antichi e diffusi
Sicherer 1998 Powell modificati
(in uso al Mount Sinai Hospital)
1.Less than 9 months of age at initial
presentation (reaction). 1. Exposure to the incriminated food elicits
repetitive vomiting, diarrhea, or both
2.Repeated exposure to the incriminated food within 4 hours without any other cause
elicited diarrhea and/or repetitive vomiting for the symptoms.
within 24 hours without any other cause for
the symptoms. 2. Symptoms are limited to the
gastrointestinal tract.
3.There were no symptoms other than
gastrointestinal symptoms elicited by the 3. Avoidance of the offending protein from
incriminated food. the diet results in resolution of symptoms.
4.Removal of the offending protein from the 4. A standardized OFC or isolated re-
diet resulted in resolution of the symptoms, exposure elicits the typical symptoms.
and/or a standardized food challenge elicited
diarrhea and/or vomiting within 24 hours after
administration of the food.Quelli di Stephanie ed Ania
Leonard 2012 Leonard 2015
1.Less than 9 months of age at initial Major Criteria
diagnosis. 1. Repetitive vomiting or diarrhea within 6 h
of food ingestion.
2.Repeated exposure to causative food elicits 2. Absence of cutaneous and respiratory
gastrointestinal symptoms without alternative symptoms suggestive of an IgE-mediated
cause. allergy.
3. Removal of causative food results in
3.Absence of symptoms that may suggest an resolution of symptoms.
IgE-mediated reaction. 4. Reexposure or a food challenge elicits the
typical symptoms.
4.Removal of causative food results in
resolution of symptoms. Minor Criteria
1. Hypotension.
5.Re-exposure or oral food challenge elicits 2. Lethargy, pallor, or hypotonia.
typical symptoms within 4 h. 3. Negative skin-prick test and undetectable
specific IgE level.
4. Absence of fever or hypothermia (I miei e gli Internazionali
Miceli Sopo 2013 Consensus 2017
1.Less than 2 years of age at first presentation Major criterion
(frequent feature but not mandatory). Vomiting in the 1-4 hour period after ingestion of
the suspect food and the absence of classic IgE-
2.Exposure to the incriminated food elicits mediated allergic skin or respiratory symptoms
repetitive and important vomiting, pallor,
hyporeactivity and lethargy within 2–4 h. Minor criteria
Diarrhea may be present, much less frequently
1. A second (or more) episode of repetitive
and later. The symptoms last a few hours,
vomiting after eating the same suspect food
usually less than 6 h.
2. Repetitive vomiting episode 1-4 hours after
eating a different food
3.Absence of symptoms that may suggest an
3. Extreme lethargy with any suspected reaction
IgE-mediated reaction.
4. Marked pallor with any suspected reaction
5. Need for emergency room visit with any
4.Avoidance of the offending protein from the
suspected reaction
diet results in resolution of symptoms.
6. Need for intravenous fluid support with any
suspected reaction
5.Re-exposure or oral food challenge elicits
7. Diarrhea in 24 hours (usually 5-10 hours)
typical symptoms within 2−4 h. Two typical
episodes are needed to deliver the definitive 8. Hypotension
diagnosis. 9. HypothermiaLa nota della Consensus 2017
• The diagnosis of FPIES requires that a patient meets the major criterion and
>3 minor criteria.
• If only a single episode has occurred, a diagnostic OFC should be strongly
considered to confirm the diagnosis, especially because viral gastroenteritis is
so common in this age group.
• Furthermore, although not a criteria for diagnosis, it is important to recognize
that acute FPIES reactions will typically completely resolve over a matter of
hours compared with the usual several-day time course of gastroenteritis.
• The patient should be asymptomatic and growing normally when the offending
food is eliminated from the diet.La diagnosi di SEA acuta per Robert e Rebecca
Quale sarà il più appropriato?
Ovvero della costruzione di un test
• Nessuno dei test ha alle spalle un iter procedurale alla regola
• Tutti sono stati elaborati in base all’ esperienza maturata su casistiche
relativamente piccole e non sempre tutti i pazienti sono stati sottoposti, in
cieco, sia al test indice (i criteri anamnestici) che al gold standard (il TPO)
• Per cui, io scelgo di essere conservativo
• Scelgo, insomma, di riservare la dieta di eliminazione a chi ha davvero forti
probabilità di essere affetto da SEA
• E quindi a chi ha presentato almeno 2 episodi di una certa severità, cioè con
pallore e letargia
• Per chi ha «meno» emetto il sospetto di SEA, elimino l’ alimento e programmo
il TPO al più prestoLo fareste? - 7
Sarà SEA quella di Roberto?
• All’ età di 20 mesi (11 mesi dopo l’ ultimo episodio di reazione avversa)
Roberto ha effettuato il TPO con merluzzo cotto
• E lo passa (= non vomita)Lo fareste? - 8
Sarà SEA quella di Rebecca?
• All’ età di 14 mesi (6 mesi dopo l’ ultimo episodio di reazione avversa) Rebecca
ha effettuato il TPO con uovo crudo
• E lo passa (= non vomita)Troppo tardi?
Vazquez-Ortiz et al, JACI IP 2017
• Forse Roberto e Rebecca
avevano già acquisito la
tolleranza al momento del
TPO?
• Possibile ma improbabile
• La freccia verde (come la
curva di sopravvivenza dell’
uovo) indica l’ età in cui
Rebecca ha fatto il suo TPO
• La freccia viola (come la
curva di sopravvivenza del
pesce) indica l’ età in cui
Roberto ha fatto il suo TPOTi piace vincere facile ? - 1
Ruffner et al, JACI in Practice 2014
• Melanie ei suoi amici del CHOP descrivono, retrospettivamente, 462 casi
di SEA, attualmente la più numerosa casistica mai pubblicata
• Da sola fa quanto tutti gli altri casi pubblicati messi insieme
• Gli autori adottano la seguente definizione di caso: “reproducible, delayed
episodes (2-6 hours after exposure to the food) of pronounced
gastrointestinal symptoms of prolonged vomiting with or without diarrhea
• If patients had hypotension, needed intravenous fluids, or had significant pallor,
they were identified as having severe reactions”
Pochi casi con letargia e palloreItaliani Conservativi
Miceli Sopo et al, CEA 2012
• L’ 80% dei casi presentava pallore e letargia
LethargyTi piace vincere facile ? - 2
Ruffner et al, JACI in Practice 2014
• Adottando criteri
diagnostici più o meno
conservativi possono
essere falsati i dati
epidemiologici
• Melanie e i suoi amici
trovano che meno del
50% dei casi reagirono ad
un solo alimento
“Another potential reason for a larger number of patients is that we
included patients with milder symptoms. We did not restrict our cohort
to only patients with cyanosis and severe hypotension”L’ Evoluzione dei criteri
Serafini et al, JACI IP 2015
• Le prime elaborazioni dei criteri diagnostici per SEA acuta prevedevano una età
massima al prima episodio di 9 mesi, durò fino al 2012
• Miceli Sopo et al spostarono il limite a 2 anni, per via della SEA da pesce che
può insorgere, appunto, dopo il 1° anno di vita
• Poi, Serafini et al pubblicarono la storia di una bambina che presentò il suo
primo episodio di SEA acuta da funghi all’ età di 7 anni
• E il criterio dell’ età venne abolito, già nei criteri di Leonard et al del 2015 non
è più presente
• L’ età di esordio della SEA acuta dipende dall’ età a cui si mangia l’ alimento
colpevole, pare banaleE questo come si classifica? - 1
La SEA è una AA non IgE-mediata?
• A 3-month-old child was brought to our allergy clinic because of, at the age of
2 months and 3 hours after his first ingestion of infant formula (80 ml), he
had a very abundant vomiting episode. Furthermore, the baby looked less
lively, but neither pallor nor lethargy were noted, then he slept peacefully.
• One week later this episode, he ingested other 80 ml of formula milk; in the
areas of the neck and upper chest, where milk touched the skin, rash and
wheals appeared in a few minutes. Then, after 30-45 minutes he
presented one abundant vomiting and, after another hour, also a second
vomiting. He also appeared sleepy but not lethargic. These symptoms resolved
after about 90 minutes. He had no diarrhea in both episodes.
• Prick-to-prick (PtP) with pasteurized cow milk (CM) and SPT with alpha-
lactalbumin commercial extract (Lofarma, Milan, Italy) resulted positive
(mean wheal = 5 mm and 3 mm respectively), while SPT with casein and beta-
lactoglobulin commercial extracts (Lofarma, Milan, Italy) resulted negative.E questo come si classifica? - 2
La SEA è una AA non IgE-mediata?
• When the baby was 4 months old, we performed an oral food challenge (OFC) with
formula milk in hospital setting.
• The child ingested 40 ml and in a few minutes we observed urticaria on his neck, in
the areas where the bib was wet with CM.
• After 2 hours he started to be less lively and responsive, and at 3 hours from the
ingestion of the milk he presented an abundant vomiting. Later, his general condition
improved and he appeared more responsive.
• Then, we performed a rub test with CM on his abdomen and after 10 minutes smaller
wheals of urticaria surrounded by erythematous halos appeared.
• Two weeks later, we also performed PtP and OFC with 20 grams of parmesan cheese;
they both resulted negative.E questo come si classifica? - 3
La SEA è una AA non IgE-mediata?
• Sebastian e Francesco hanno storie simili, rispettivamente con il latte vaccino e
con l’ uovo di gallina, a quella di Leonardo
• Quale allergia alimentare si esprime con vomito a 2 e più ore di distanza dall’
inizio dell’ ingestione dell’ alimento colpevole?
• E’ possibile che la SEA acuta comprenda più fenotipi e che in alcuni di essi le
IgE specifiche possano svolgere un ruolo patogenetico?
• E’ dunque ipotizzabile una modifica in tal senso dei criteri diagnostici vigenti?I miei e gli Internazionali
Miceli Sopo 2013 Consensus 2017
1. Less than 2 years of age at first presentation Major criterion
(frequent feature but not mandatory). Vomiting in the 1-4 hour period after ingestion
of the suspect food and the absence of classic
2. Exposure to the incriminated food elicits IgE-mediated allergic skin or respiratory
repetitive and important vomiting, pallor, symptoms
hyporeactivity and lethargy within 2–4 h.
Diarrhea may be present, much less frequently Minor criteria
and later. The symptoms last a few hours,
1. A second (or more) episode of repetitive
usually less than 6 h.
vomiting after eating the same suspect
food
3. Absence of symptoms that may suggest an 2. Repetitive vomiting episode 1-4 hours after
IgE-mediated reaction. eating a different food
3. Extreme lethargy with any suspected
4. Avoidance of the offending protein from the reaction
diet results in resolution of symptoms. 4. Marked pallor with any suspected reaction
5. Need for emergency room visit with any
5. Re-exposure or oral food challenge elicits suspected reaction
typical symptoms within 2−4 h. Two typical 6. Need for intravenous fluid support with any
episodes are needed to deliver the definitive suspected reaction
diagnosis.
7. Diarrhea in 24 hours (usually 5-10 hours)
8. Hypotension
9. HypothermiaGRASSIT TE GRASSITTE
Puoi anche leggere