CARCINOMA OVARICO BRCA MUTATO - AIOM-SIGU-SIBIOP-SIAPEC-IAP Le raccomandazioni 2019
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
CARCINOMA OVARICO BRCA MUTATO
Le raccomandazioni 2019
AIOM-SIGU-SIBIOP-SIAPEC-IAP
Laura Cortesi
SS Genetica Oncologica
Dipartimento di Oncologia ed Ematologia
Azienda Ospedaliero Universitaria Policlinico di Modena
5200 new cases in 2018 in Italy
3186 deaths in 2015
78 % III - IV stage
I Numeri del Cancro in Italia, 2018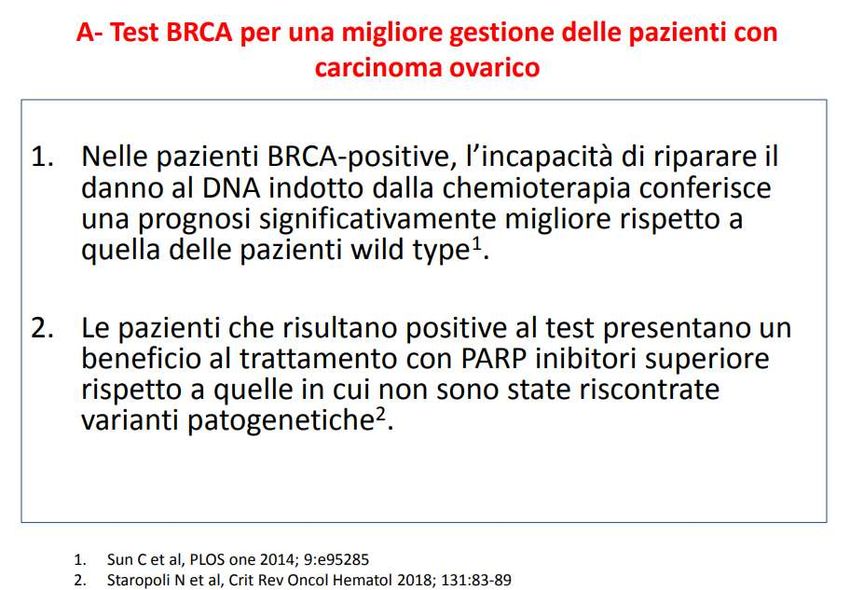
TP53/Rb
pathway KRAS TP53/Rb pathway
Chromosomal mutations Chromosomal
instability Mucinous instability
PTEN, 5%
15%
ARID1A, Clear cell 5% High-grade
PI3KA serous
63%
12%
KRAS, PTEN
mutations
Romero I et al. Endocrinology 2012; 153: 1593-1602
Homologous Recombination (HR) Deficiency
in High Grade Ovarian Cancer
BRCA2
BRCA1 Germline
Germline 6%
8%
BRCA1
Somatic
3%
BRCA2
Somatic
BRCA Mutation
Other
34%
3% 31%
BRCA1 (14%germline)
Methylation
11%
EMSY Others HR
MMR Amplification
Germline 6% deficiency
PTEN Loss
2%
CCNE1 Other HRD 5%
18%
Amplification 7%
15%
No HR deficiency HR deficiency
Levine, D. The Cancer Genome Atlas, Molecular profiling of serous ovarian cancer. 2011.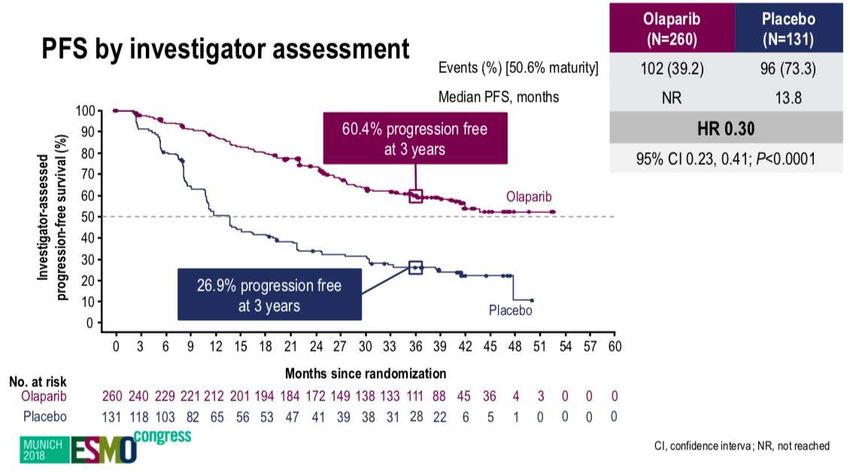
Germline BRCA test
BRCA mutation frequency in 1001 patients
with non mucinous ovarian cancer
Germline BRCA mutation detected in:
14.1% of the overall population
15.6% 60 yrs old
17.1% of high grade serous subtype
44% with no family history of both ovarian and breast cancer
Alsop K, et al. J Clin Oncol 2012; 30: 2654–63
BRCA mutation testing: why are patients with ovarian cancer being
tested for BRCA?
Important prognostic factor, other than stage
Prognostic and extent of surgical debulking
factor Estimate PFS and OS according to BRCA
status
Treatment Identification of patients more sensitive to
subsequent chemotherapy-based treatments
decisions or suitable for targeted therapies (PARPi)
Risk Identification of BRCA mutation carriers to
take preventive action (for them or their
assessment relatives)
9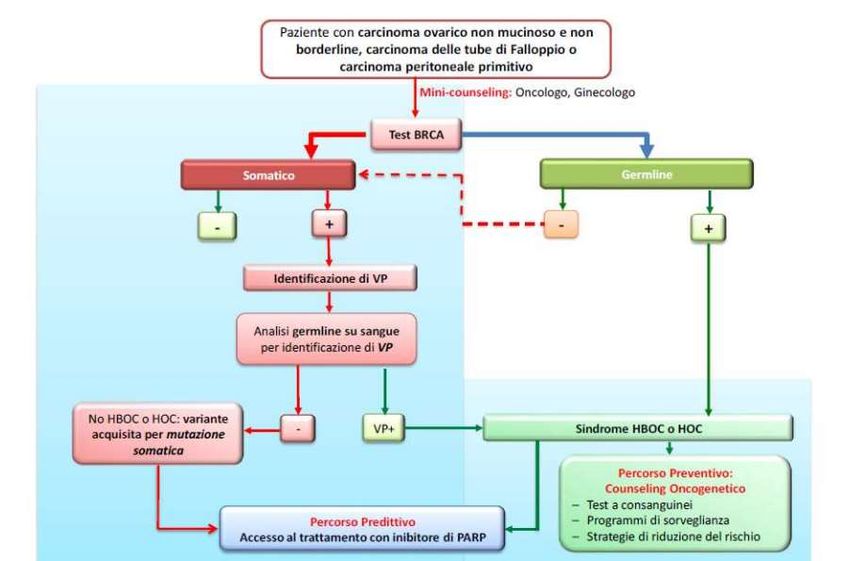
Bolton, JAMA 2012

DNA damaging RAD51 forms nucleoprotein filaments
BLM
WRNBRIP1
RAD51
ATR ATM RAD51
BRCA1
I RAD51
D2 Ub
L
A
B BRCA2
G
CHK1 C
F
CHK2 M E
TP53
ATM is a DNA damaging “sensor”that promote apoptosis by CHK2-TP53 and activates BRCA1 that blocks the
transcription by cell cycle arrest at the G1/S, S and G2/M checkpoints and by ubiquitination of FANCD2
otherwise induces the DSB repair by chromatin remodelling
Modified by Cortesi L., Curr Cancer Drug Targets 2018
Chemosensitivity/resistance
Tassone P. et al.; 2003:88; 1285-1291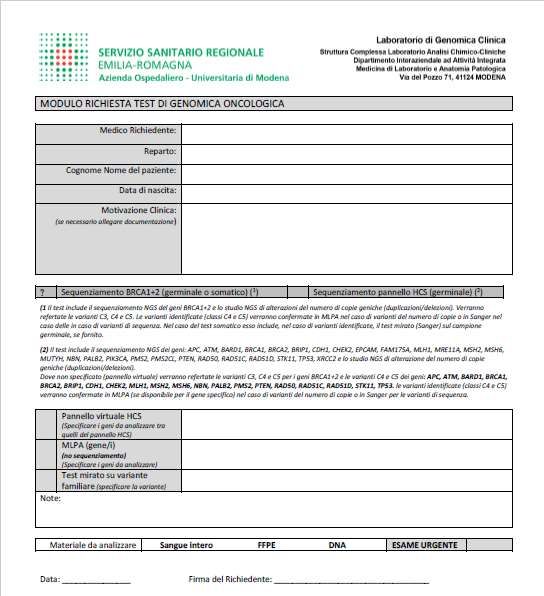
Alsop K, JCO 2012
Phase II trial of trabectedin in BRCA-mutated and/or BRCAness phenotype
recurrent ovarian cancer patients:
the MITO 15 trial
PFS: BRCA
Non BRCA
OS: BRCA
Non BRCA
Lorusso D., Ann of Oncol 2016BRCA status and response to chemotherapy
• 42% platinum resistant; 58% partially platinum • OVA-301 phase III study in recurrent ovarian cancer
sensitive • PLD +/- trabectedin
Kaye SB, et al. J Clin Oncol 2012 Monk , et al. Ann Oncol 2015Toss and Cortesi. J Canc Sci Therapy 2013; Cortesi L et al. Curr Cancer Drug Targets 2018; Murai J et al. Cancer Res. 2012 ; Livraghi and Garber, BMC Medicine 2015
Study 19: Phase II trial design, endpoints and
BRCA testing
N=265
Primary endpoint:
• ‘Platinum-sensitive’ n=136 Olaparib maintenance Progression-free survival (PFS)
recurrent high-grade monotherapy by RECIST 1.0
serous ovarian cancer (400 mg bid, capsules)
Secondary endpoints included:
• ≥2 prior regimens of Double-blind Overall survival (OS),
platinum-based randomization Treatment until progression safety and tolerability
chemotherapy 1:1
Exploratory endpoints:
• Complete or partial Placebo (bid, capsules) Time to first subsequent therapy
response to most n=129 or death (TFST), time to second
recent platinum-based subsequent therapy or death (TSST)
regimen
BRCA testing:
• Previous local germline BRCA testing (case report forms) BRCAm: n=136
• Retrospective germline BRCA testing or tumour BRCA BRCAwt:*
testing n=118
*BRCAwt patients did not have a detected BRCAm or had a BRCAm of unknown significance
bid, twice daily; BRCAwt, BRCA1/2 wild type; RECIST, Response Evaluation Criteria in Solid TumorsStudy 19: PFS in BRCA mutated pts
BRCAm (n=136)
Olaparib Placebo
Events: total pts (%) 26:74 (35.1) 46:62 (74.2)
1.0 Median PFS, months 11.2 4.3
0.9 HR=0.18
95% CI: 0.11, 0.31; pStudy 19: Somatic BRCA
No evidence of difference in treatment effect from gBRCA
• 165 patients with BRCAm status available from germline and tumour
• 18 patients identified with a BRCAm in the tumour in the absence of a mutation
being identified in the germline
Study 19 PFS and OS events: somatic tumour BRCA population
PFS (DCO 30 June 2010) OS (DCO 26 Nov 2012)
Olaparib Placebo Olaparib Placebo
(n=8) (n=10) (n=8) (n=10)
Events n (%) 3 (38) 6 (60) 4 (50) 6 (60)
• Data appear consistent with the predicted biology, with fewer patients on
the olaparib arm showing progression events or death events at the
respective data cut offs
Ledermann et al; Lancet Oncol 2014; 15: 852–61
25Study 19: PFS In BRCA Wild Type Pts
FDA Approval EMA Approval
*
* Obligation to conduct post-authorisation measures:
Study OPINION only on BRCA wt will be
presented on June 2021Niraparib: Phase III ENGOT-OV16/ NOVA Trial
Platinum-sensitive recurrent high-grade serous ovarian cancer
Treatment with 4-6 cycles of platinum-based therapy
Response to platinum treatment
Germline BRCA mutant Nongermline BRCA mutant
2:1 Randomization 2:1 Randomization
Niraparib Niraparib
Placebo Placebo
300 mg once daily 300 mg once daily
Treat until progression of disease Treat until progression of disease
Primary endpoint: PFS by central, blinded review
• HRD-positive population
─ Tested at 100 events to achieve PENGOT-OV16/ NOVA Niraparib Significantly
Improved PFS for All Patient Populations
gBRCAmut Non-gBRCAmut Overall Non-gBRCAmut HRDpos
HR=0.27, PRucaparib in Relapsed, Platinum-Sensitive
High-Grade Ovarian Carcinoma (ARIEL2 Part 1):
An International, Multicenter, Open-Label, Phase II Trial
Monotherapy, measurable disease, and pretreatment
and archival biopsies
LOH, loss of heterozygosity; ORR, objective response rate; PK, pharmacokinetics
Swisher EM, et al. Lancet Oncol. 2017;18(1):75-87.ARIEL2 (Part 1): Progression-Free Survival
ARIEL3: Study Design
Patient eligibility Stratification
Rucaparib
600 mg BID
• High-grade serous or endometrioid epithelial • HRR status by NGS mutation analysis n = 375
ovarian cancer, primary peritoneal, or fallopian Mutation in BRCA1, BRCA2, or
─
tube cancers non-BRCA HRR gene†
Randomisation 2:1
• ≥2 prior lines of platinum-based treatments ─ No mutation in BRCA or HRR gene
• No prior PARP inhibitors • Response to recent platinum
• Sensitive to penultimate platinum ─ CR
• Responding to most recent platinum (CR or PR)* ─ PR
─ Excludes patients without assessable disease • Progression-free interval after
following surgery before more recent platinum- penultimate platinum
based therapy ─ 6 toARIEL3: Investigator-Assessed PFS
BRCA mutant HRD ITT
Median, Median,
Median, Months 95% CI
Months 95% CI Months 95% CI
Rucaparib 16.6 13.4-22.9 Rucaparib 10.8 8.3-11.4
Rucaparib 13.6 10.9-16.2 n = 375
n = 130
n = 236 Placebo 5.4 5.3-5.5
Placebo 5.4 3.4-6.7
Placebo 5.4 5.1-5.6 n = 189
n = 66
n = 118 HR, 0.36;
HR, 0.23;
HR, 0.32; 95% CI, 0.30-0.45;
95% CI, 0.16-0.34;
95% CI, 0.24-0.42; PFDA Approval
In Italia
solo
BRCAm
Rucaparib HGSOC with CR or PR to PBC
Regardless BRCA/HRD status
PARP i approved as
treatment Rucaparib HGSOC
gBRCAm/sBRCAm
Platinum Sensitive
Expert Review of Anticancer Therapy 2019Sulla base di queste evidenze, si ribadisce la raccomandazione di proporre l’invio al test BRCA sin dal momento della prima diagnosi di carcinoma epiteliale ovarico non mucinoso e non borderline, di carcinoma delle tube di Falloppio o di carcinoma peritoneale primitivo. La proposta di esecuzione del test BRCA al momento della diagnosi deve avvenire fornendo una adeguata informazione su tutti gli aspetti collegati ai possibili risultati del test e rispettando i tempi decisionali della paziente.
Percorso pz. Con carcinoma ovarico
SOSPETTO CA
OVARICO
COG pretest effettuata Pz.sottoposta a
da ginecologi chirurghi chirurgia per
e oncologi FORMATI e
firma CI per tessuto e sospetto
sangue ca.ovarico:diagno
si estemporanea
Carbo+Taxolo
e Olaparib di
mantenimento
4 Diagnosi
settimane
definitiva di C.O.
COG post test non mucinoso e
Se analisi non borderline
Comunicazione somatica +
del risultato: se per LOH
gBRCA+ avvio conferma su
COG familiari sangueL’identificazione di variante patogenetica germinale nei geni BRCA in una paziente con carcinoma ovarico permette di intraprendere un percorso di consulenza oncogenetica nei familiari al fine di identificare i portatori ad alto rischio, cui proporre programmi mirati di diagnosi precoce dei tumori associati alle sindromi a trasmissione eredo-familiare BRCA- relate e strategie finalizzate alla riduzione del rischio. La presa in carico delle donne con tumore ovarico BRCA- relato deve prevedere un approccio bio-psicosociale, che tenga conto dell’impatto della diagnosi e dei trattamenti sulla sfera fisica e psico-emotiva di ciascuna donna affetta da tumore ovarico, così come delle implicazioni psicologiche della problematica eredofamiliare e del coinvolgimento dei familiari sani a rischio nel percorso decisionale.
Il test BRCA su pazienti con carcinoma ovarico può essere effettuato su sangue periferico oppure su tessuto tumorale. Tuttavia, è preferibile effettuare in prima istanza il test su tessuto tumorale, al fine di poter identificare varianti di natura sia germinale che somatica. Per il test somatico, i preparati istologici devono essere rivalutati da un patologo che individuerà le aree più rappresentative della lesione e con maggiore quantità di cellule tumorali. Il test su tessuto presenta ancora delle problematiche tecniche che lo limitano a selezionati laboratori specializzati. I laboratori devono offrire un test validato e i risultati devono essere disponibili in tempi rapidi. Alle pazienti che hanno in prima istanza effettuato il test germinale con esito non informativo (nessuna variante patogenetica identificata) e che sono candidate ad un trattamento con PARP inibitori, va proposto il test somatico
Nel referto deve essere indicato il significato clinico della variante genetica BRCA identificata e devono essere elencate le informazioni essenziali utilizzate per la classificazione. Recentemente, sono stati sviluppati dal consorzio ENIGMA criteri specifici per l’interpretazione del significato clinico (accertamento di rischio ereditario) delle varianti costituzionali dei geni BRCA.
Si richiede ai medici prescrittori del test BRCA di utilizzare un adeguato protocollo di comunicazione e raccolta del consenso scritto, attraverso la definizione di appositi moduli informativi e di consenso informato. Le informazioni da dare alla paziente dovranno riguardare i potenziali benefici in termini prognostici e terapeutici, la possibilità di rilevare per se stessi il rischio di sviluppare un altro tumore e l’opportunità per i propri familiari di effettuare test predittivi di rischio oncologico. È necessario per gli oncologi ed i ginecologi oncologi che non hanno una specifica esperienza in genetica oncologica eseguire un percorso formativo che includa anche gli aspetti etici del test BRCA. Andrà individuata un’équipe di genetica clinica oncologica, cui fare riferimento qualora siano indicati o richiesti dalla paziente approfondimenti sugli aspetti genetici.
Somatic Mutation Information
Individual, only for
OC treatment
Germline Mutation
Information FamilyNeed to make explicit the AGREEMENT
between subject and researcher
in keeping with the principles of
AUTONOMOUS CHOICE
INFORMED
CONSENTCONSENSO INFORMATO AL TEST BRCA
Acconsento all’esecuzione sul mio campione biologico del test genetico finalizzato
alla ricerca di mutazioni di BRCA1 e BRCA2, considerate fattori predisponenti ai
tumori della mammella e dell’ovaio e predittivi di risposta a terapie specifiche in
particolare:
test completo BRCA1 e BRCA2 [ ]
test mirato BRCA1 o BRCA2 [ ]
Firma: ………………………………………………….. Data : ………………………….
Firma di chi ha raccolto e illustrato il consenso:
Dott…………………………………………………… Data : ………………………….CONSENSO INFORMATO AL TEST BRCA
Consapevole delle finalità e delle limitazioni Dichiaro inoltre di:
[ ] volere [ ] non volere essere informata/o circa i risultati delle analisi
[ ] volere [ ] non volere rendere partecipe la mia famiglia circa la decisione di eseguire tali analisi
[ ] volere [ ] non volere rendere partecipi i miei familiari riguardo i risultati delle analisi
[ ] volere [ ] non volere rendere partecipe dei risultati il mio medico di famiglia Dr:…………….…..
[ ] volere [ ] non volere che il Materiale Biologico estratto venga conservato anche dopo l'esecuzione del test
[ ] volere [ ] non volere che il Materiale Biologico venga usato, sempre con garanzia di massima riservatezza, per
studi o ricerche scientifiche riguardanti la predisposizione genetica ai tumori della
mammella e dell’ovaio e la possibilità di utilizzare un trattamento mirato per la neoplasia
ovarica
[ ] volere [ ] non volere essere informata/o di eventuali nuovi risultati o possibilità diagnostiche derivanti dai
nuovi studi o ricerche future
Di essere a conoscenza della possibilità di REVOCARE il presente consenso in qualsiasi momento
Una copia di questo consenso informato e del foglio informativo restano in mio possessoModello
richiesta
tessuto
somatico
all’anatomia
patologica di
riferimentoModello di richiesta al nostro laboratorio
Sanger Sequencing
SNVs &
Indel confirmation
NGS
on both
FFPE Ion Torrent Oncomine
sample Tumor & Genomic
BRCA Assay
Promega
Ion Reporter DNAs
Maxwell 16
LEV FFPE Oncomine >5% allele
DNA kit
pipeline frequency
10ng + C3, C4, C5 variants
tumor DNA
CUSTOM
5 slides Ion Torent Chef / Ion Torrent S5 BIOINFORMATIC
of 10 µm
PIPELINE CNVs
MLPA FISH
for sequence
alignment and
variant calling
confirmation on confirmation on
Genomic DNA FFPE SampleSanger Sequencing
+ (pos) NGS on tumor sample DNA
(pos) Sanger on Genomic DNA Germline variant
SNVs &
Indel confirmation (pos) NGS on tumor sample DNA
on both Somatic variant
Thermo (neg) Sanger on Genomic DNA
Minor Variant Finder Tumor & Genomic
Software DNAs
>5% allele
frequency
C3, C4, C5
variants
MLPA FISH
CNVs (pos) NGS on tumor sample DNA Germline CNV
(pos) MLPA on Genomic DNA
(pos) NGS on tumor sample DNA
(neg) MLPA on Genomic DNA Somatic CNV
confirmation on confirmation on (pos) FISH on FFPE Sample
Genomic DNA FFPE Sample
MRC-Holland Coffalyser.net SoftwareMafficini A et al,. Oncotarget. 2016 Jan 12;7(2):1076-83
PROPORTION OF PATHOGENIC VARIANTS
(C4-C5),
NON-PATHOGENIC VARIANTS IN TESTING
SEROUS HIGH GRADE OC
15%
Germline Mutation (23)
15%
70% Somatic mutation (22)
NON PATHOGENIC (43)
150 OC TESTED FOR SOMATIC BRCA1/2Puoi anche leggere