SEGNI LINGUISTICI PRECOCI DI DECADIMENTO COGNITIVO - G. GAGLIARDI CLUB - CIRCOLO LINGUISTICO DELL'UNIVERSITÀ DI BOLOGNA - GLORIA GAGLIARDI, PHD
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
Segni linguistici precoci
di decadimento
cognitivo
G. Gagliardi CLUB – Circolo linguistico
dell’Università di Bologna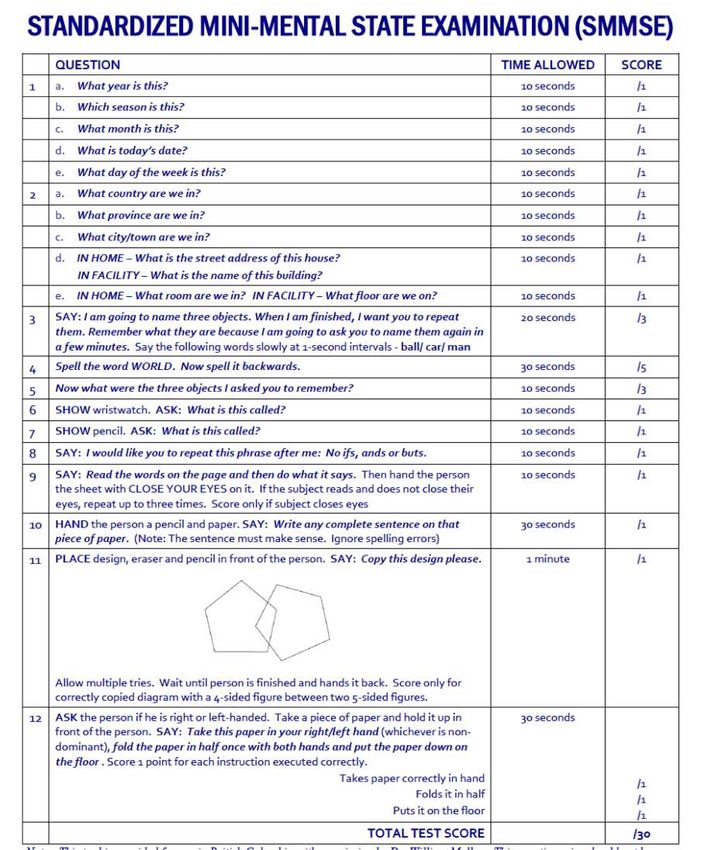
World Alzheimer Report 2018
The state of the art of dementia research
Quadro
Epidemiologico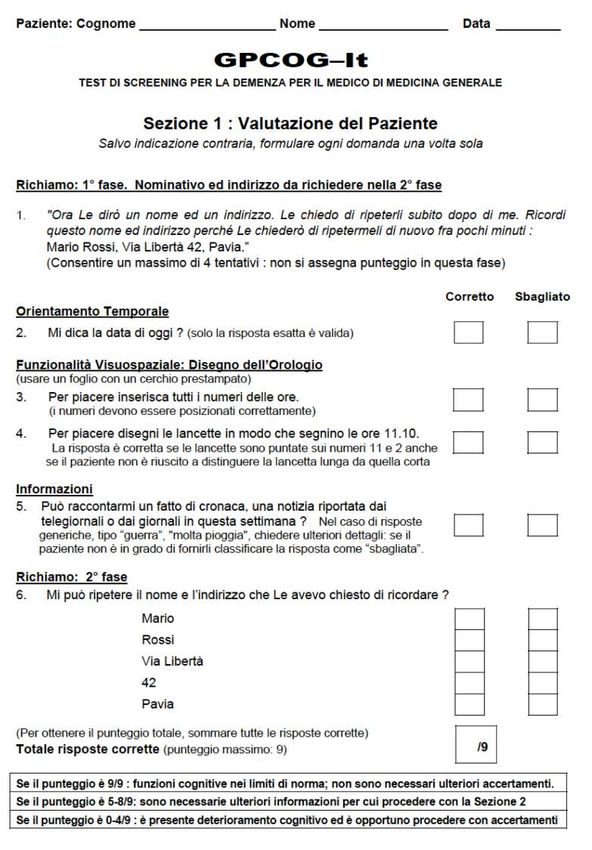
Aumento aspettativa di vita
20° secolo: da 54 a 80 anni
[Chattat, 2004]
Maggior incidenza patologie
neurodegenerative
Quadro
Epidemiologico
“Scenari demografici per l'area metropolitana bolognese al 2033”
(http://inumeridibolognametropolitana.it/studi-e-ricerche)
A cura di: Ufficio di Statistica del Comune di Bologna, Servizio Studi e Statistica per la programmazione strategica
della Città metropolitana di Bologna, Regione Emilia-Romagna, Istat
invecchiamento come fenomeno significativo della storia demografica
del territorio:
nella Città metropolitana il numero degli over 64 è salito dal 13% del
Censimento del 1971 all’attuale 25%, mentre il loro numero assoluto nello
stesso arco temporale è praticamente raddoppiato (da quasi 122 mila a
La situazione a 246.700).
La tendenza si confermerà nei prossimi anni
Bologna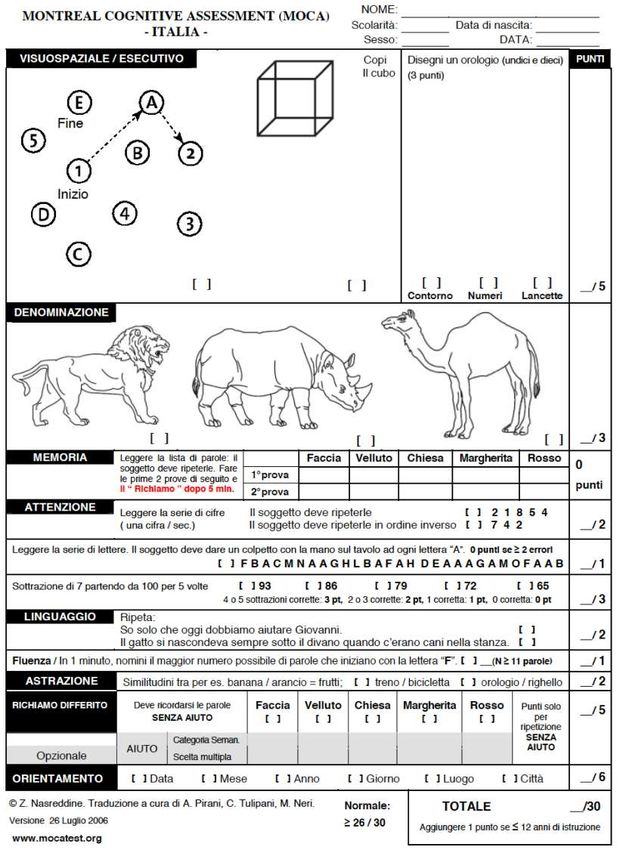
EUROPEAN COMMISSION (2012), “Report on the public
consultation on eHealth Action Plan 2012-2020”
Reale emergenza per il Sistema Sanitario e Assistenziale
Quadro pubblico:
una popolazione più longeva richiede infatti una redistribuzione più
epidemiologico efficiente delle cure e metodologie più accurate di prevenzione e
diagnosi precoce.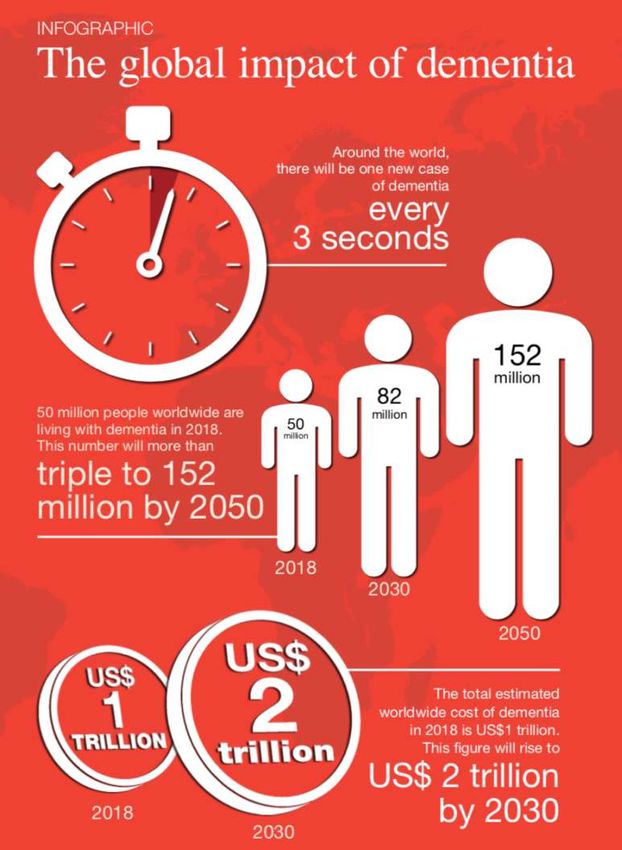
Quadro
Epidemiologico n tia,
de m e
w o rld with t w o th irds,
p le in t h e a i n . About
m i lli o np e o
K o r e a or S p
d de m e ntia,
o f th e 5 0 f South ia , mixe
s o n e s i ze o e m e n t
n n if e r Bute i a ro u n d the v e v a s c ular d TD).
“J e m u n i t y h e r s h a tio n ( F
a global
com
z h e im e r’s. Ot o r a l d e genera be reversed.
B u t e , have Al r f ro n totemp lls th a t can’t
le b y 2 050,
like
d y de m entia o o t h e b rain ce m i lli o n peop
t ut 152
Lewy bo have damage is e t o a b o
la d esh.”
t h e m t o r a n g
All of u n it y is likely o f R u ss ia o r B
m e
That com t’s more the siz
ha
to o n e t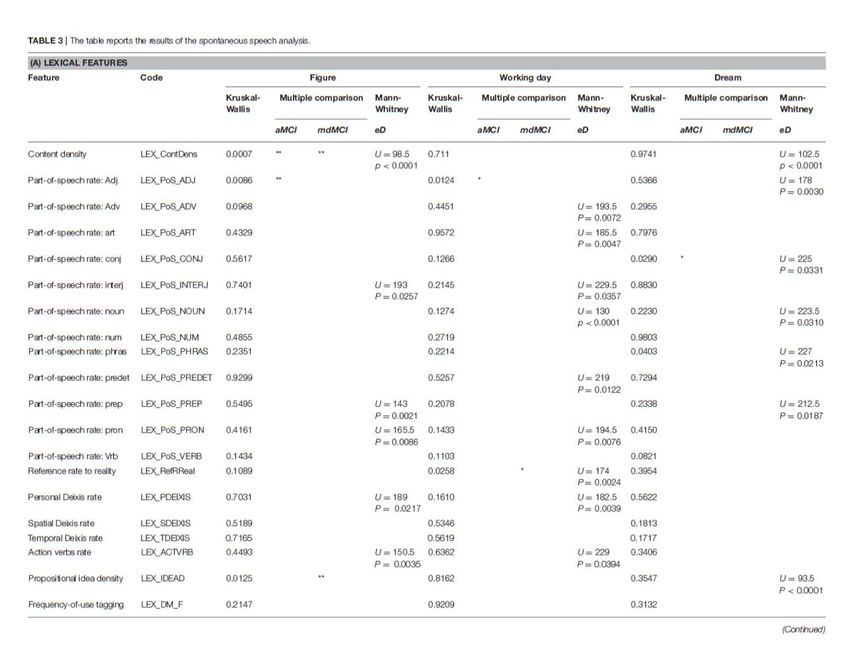
OPLON Care & Cure Opportunities for active and healthy LONgevity Smart Cities and Communities – DD 391/RIC, Ministero Università e Ricerca Obiettivo: proporre azioni e metodi finalizzati a prevenire la fragilità e promuovere la salute degli anziani, progettando e sviluppando strumenti e reti di diagnosi precoce e di care&cure.

Demenze e MCI come entità nosologiche

Paziente adulto con disturbo cognitivo
Eziologia varia
Non solo
Alzheimer…NEUROPATOLOGIA
ESPRESSIONE CLINICA: decadimento cognitivo
Non solo
Alzheimer…
Condizioni neurologiche caratterizzate da decadimento
cognitivo progressivo dovuto ad una graduale perdita di
funzione neuronale Processi patologici sottostanti intaccano in maniera
selettiva network neurali anatomicamente interconnessi
e funzionalmente collegati dando luogo ad alcune
presentazioni cliniche caratteristiche, spesso
«parzialmente sovrapposte»
Decadimento cognitivo
Disordini del movimento
Malattie caratterizzate da placche amiloidi e NFT (es.
Alzheimer)
1. deposizione di peptide β amiloide (Aβ)
Nel parenchima cerebrale (placche senili)
Nei vasi cerebrali (angiopatia amiloide)
Demenze dovute a 2. Formazione di ammassi neurofibrillari (accumulo
intraneuronale di tau iperfosforilata)
processi Degenerazione Lobare Frontotemporale (PPA, Demenza
semantica, bvFTD)
neurodegenerativi FTLD -tau: Malattia di Pick (es. bvFTD), Degenerazione
corticobasale, paralisi sopranucleare progressiva (es.
parkinsonismo atipico)
FTDL-TDP-43-positive inclusions (anche nella Sclerosi
laterale amiotrofica)
FTDL-FUS-positive inclusions
AGD: Malattia a granuli argirofili
Sinucleinopatie (es. Demenza con corpi di Levy e Demenza
da Parkinson)
corpi di Lewy: aggregati proteici a base di alfa-sinucleina
Malattie da poliglutammine (es. Malattia di Huntington) Alzheimer
PRESENTAZIONE CLINICA : deficit di memoria episodica (amnesia anterograda),
linguaggio (in particolare memoria semantica), ragionamento astratto, funzioni
esecutive, attenzione, abilità visuo-spaziali e costruttive,
Demenza Vascolare:
causata da disturbi circolatori nel cervello: eventi acuti (es. ictus emorragico)
o eventi vascolari minori e processi «cronici» (es. patologia dei piccoli vasi
cerebrali, PPV)
PRESENTAZIONE CLINICA: Deficit eterogenei: interessate soprattutto le funzioni
Demenze: esecutive
Demenza «Mista»: Alzheimer + Vascolare
tipologia Demenza Fronto-temporale
Afasia Progressiva Primaria (PPA): non fluente/logopenica
Demenza Semantica (variante semantica PPA)
Variante comportamentale della Demenza Fronto-temporale
Demenza con Corpi di Levy (e demenza associata a Parkinson)
PRESENTAZIONE CLINICA: Fluttuazioni dei livelli di arousal,
allucinazioni, disautonomia, parkinsonismo, deficit di attenzione e
concentrazione, REM Sleep Behaviour Disorder PROBLEMA n° 1: IDENTIFICAZIONE della PATOLOGIA da
STUDIARE
Problema di categorizzazione: vorremmo delle CLASSI, ci troviamo
PROBLEMI davanti un continuum
1. Eziologia multifattoriale
2. Espressione dei sintomi Non esiste una soglia sul piano biologico che delimiti il
passaggio da una situazione di normalità cognitiva a una di
demenza severa e conclamata
Invecchiamento “Tipico”:
Typical cognitive aging occurs in about two-thirds of persons over age 70. It involves
modest atrophy of association cortices, hippocampus, caudate, and cerebellum along
with decreasing integrity of anterior white matter structures. Diffuse amyloid
plaques and rare neurofibrillary tangles may appear, but there is limited gliosis and
limited cell loss. In turn, these findings may associate with the decreased cognitive
Il MCI come processing speed and cognitive flexibility that are the hallmarks of cognitive aging.
entità nosologica Smith & Bondi [2013]
continuum cognitivo, che va dall’invecchiamento “tipico” alla
demenza passando per una fase di compromissione cognitiva
lieve.
Il Mild Cognitive Impairment (MCI) [Petersen, 2004; 2011;
Winblad et al., 2004], come entità clinica, individua appunto
questa zona grigia.Terminologia
IDENTIKIT del paziente con MCI [Winblad et al., 2004]
1. il paziente non è né normale, né demente: pur manifestando
deficit cognitivi, non soddisfa i criteri per la diagnosi di
demenza;
2. il paziente mostra un declino cognitivo:
Mild Cognitive 1. il declino è avvertito dal paziente stesso e/o confermato da un
parente ed è dimostrato da un impairment in test cognitivo
Impairment oggettivo;
2. si evidenzia un declino cognitivo progressivo nel tempo,
mediante somministrazioni successive di test cognitivi oggettivi;
3. le attività di base del vivere quotidiano sono preservate, il
decadimento delle funzioni strumentali complesse è minimo. Spettro di condizioni eterogenee [Winblad et al., 2004]
Mild Cognitive
Impairment
Le diverse tipologie di Mild Cognitive Impairment rappresentano con altissima
probabilità le fasi prodromiche di diverse malattie neurodegenerative
Le forme amnesiche si evolvono di solito in AD [Petersen, 2011];
Le forme non amnesiche, meno comuni, possono invece svilupparsi in un’ampia
tipologia di malattie dementigene (tra le principali: demenze fronto-temporali,
demenze con corpi di Lewy e afasia progressiva primaria) PROBLEMA n° 2: LA VARIABILITÀ INTERINDIVIDUALE
C’è una discrepanza tra il grado di degenerazione corticale e la
sua manifestazione clinica [Katzman et al., 1988]:
Analisi post-mortem del cervello di 137 anziani, in 10 di essi
riscontrata la presenza di chiari segni di demenza di Alzheimer a
livello neuroanatomico, in assenza però di manifesti sintomi
cognitivi.
«Le differenze individuali nei processi cognitivi, e quindi nei
La «riserva» sottostanti network neurali, conseguenti alle diverse
esperienze a cui il soggetto è stato esposto (es. educazione,
occupazione lavorativa e attività ricreative intellettualmente
stimolanti), consentono ad alcuni pazienti di fronteggiare
meglio modificazioni cerebrali strutturali e funzionali,
costituendo dunque un fattore protettivo per il decadimento
cognitivo.» [Corsi & Gagliardi, in press]RISERVA: maggior resilienza del cervello al danno neuropatologico
RISERVA CEREBRALE
modello di tipo «passivo» («Brain Reserve», BR)
peculiarità individuali dell’anatomia cerebrale, risorse neurali
quantificabili che consentono all’individuo di far fronte ad un danno
neurale [Mortimer et al., 1981; Katzman, 1993; Satz, 1993]:
Dimensione dell’encefalo
Struttura
valore «soglia critica» («threshold») di tipo neurofisiologico, superato il
quale la patologia trova un’espressione clinica.
La «riserva» RISERVA COGNITIVA
Modello di tipo «attivo» («Cognitive Reserve», CR).
Costrutto teorico che descrive «l’insieme di abilità cognitive, capacità
strategiche e conoscenze acquisite che, nell’arco della vita, le esperienze
vissute hanno permesso di accumulare» [Mondini, 2013]
Risorse di tipo «funzionale»: il cervello può, in maniera attiva, aggirare
o compensare le limitazioni imposte dalla patologia
maggiore flessibilità ed efficienza delle reti neurali,
Riuso di network preesistenti o di istituzione di meccanismi compensatoriScreening e diagnosi Breve quadro dello stato dell’arte
Calzà et al. [2015]: Should we screen for cognitive decline and
dementia?
The stringent ethical question that arises from the hypothesis of
population/community-based screening programmes of cognitive
frailty is: should people who are asymptomatic be told that they
are more likely than others to develop a cognitive impairment? The
identification of “cognitively frail persons” in the context of a
population-based screening programme might lead to two opposite
scenarios:
Screening: i. to identify cognitive decline due to non neurological disorders, that
questioni etiche ii.
might be potentially reversible if early and correctly diagnosed;
to identify participants in an asymptomatic phase of a
neurodegenerative cognitive disorder.
While the benefit in the first case is evident, the questions in the
second scenario are related to the risk of disclosing an AD
diagnosis in asymptomatic or minimally symptomatic persons with
full insight, with no specific treatment options currently available
plus the risk of catastrophic reactions related to an “AD-stigma” Given the above debates and evidence, we suggest that the question
should be less “AD-centred” and re-directed as follow: what is the
potential benefit of population-based cognitive screening
programmes vs the hazard of AD overdiagnosis?
Potential benefits include secondary prevention based on:
i. the recognition and correction of fully reversible cognitive declines
due to non neurological disorders and diseases, malnutrition,
inappropriate poly-therapies, etc.;
ii. more appropriate management in hospitalization, prescribing,
surgery and anaesthesia;
Screening: iii. appropriate steps to prevent injury (preventing falls, burns from
leaving heaters or cookers on, dropping hot liquids etc.) in home-
questioni etiche care;
iv. better adherence and management of other medical conditions,
given that social isolation and depression are some of the biggest
contributors to deterioration;
v. to enable policy makers to take decisions based on scientific
evidences regarding medical and social economy in an ageing-
population, to predict and plan care needs and housing decisions.
Again, although the risk of AD overdiagnosis is probably still high at
the moment, “strategies to overcome this limitation might be on the
horizon”, thanks to the research in non-invasive biomarkers. Organizzazioni e gruppi di lavoro internazionali hanno elaborato
consensus/position paper negli ultimi decenni
Scopo di ricerca, ma impatto sulla pratica clinica
1984 (update: 2011): NINCDS-ADRA (The National Institute of
Neurological and Communicative Disorders and Stroke and the Alzheimer’s
Disease and Related Disorders Association) [McKhann et al. 1984]
Demenza come entità clinico-patologica. 3 regole:
La diagnosi 1.
2.
the diagnosis is clinico-pathological: it cannot be certified clinically, and
needs a post-mortem confirmation to be ascertained;
the diagnosis of AD can only be ‘probable’;
3. the diagnosis of AD can only be made when the disease is advanced and
reaches the threshold of dementia
2007–2010: IWG (The international Working Group on the New Criteria for
the Diagnosis of Alzheimer Disease) [Dubois et al. 2007; 2010]
Demenza come entità clinico-biologica
1. Biomarkers can be considered as surrogate markers of the histopathological
changes.
2. According to this, and in contrast with other working groups, the clinical
diagnosis can be established in vivo 2011: NIA/AA (the National Institute on Ageing and the Alzheimer’s
Association)
the workgroup identified Alzheimer's disease as a continuum with
three distinct stages: Preclinical, Mild Cognitive Impairment and
Dementia.
Expand the criteria for Alzheimer’s dementia beyond memory loss
as the first or only major symptom
Recognize the potential use of biomarkers—indicators of
La diagnosi underlying brain disease—to diagnose Alzheimer’s disease.
Core criteria for dementia:
1. difficulties in independent functioning; decline from a previous level
of functioning;
2. no delirium or major psychiatric disorders; cognitive impairment
based on history and mental status examination;
3. cognitive impairment in at least two of the following domains:
learning and memory; reasoning; visuo-spatial abilities; language;
personalityClassificazione e criteri per la diagnosi delle demenze
“Introduction to the diagnosis of dementia”
Gauthier & Rosa-Neto (eds.) 2011 «Case Studies in Dementia: Common and Uncommon
Presentations»
[…] the clinician must establish through a systematic history with the
subject and an informant if there is a decline in memory, language, praxis,
gnosis, and/or executive abilities, and if this decline is associated with
impairment in activities of daily living (ADL).
Although the history is the cornerstone of the diagnosis of dementia,
complementary laboratory tests usually include:
basic blood tests (hematologic, endocrine, hepatic, renal function, screening,
La diagnosi B12, VDRL, HIV)
brain imaging using Computer Scanning (CT) or Magnetic Resonance Imaging
(MRI) studies
Special tests will depend on the suspected cause of dementia and include:
Special blood tests (coeruloplasmin for Wilson’s disease, for example)
Special brain imaging such as Positron Emission Tomography (PET) for glucose
metabolism (FDG-PET), amyloid load (PIB, for instance)
Electroencephalography (in Creutzfeldt–Jacob disease)
Lumbar puncture (some protein markers in AD, in neurosyphilis)
Immunology work-up for antibody-mediated dementias (paraneoplastia
syndromes, Hashimoto’s encephalitis)
Genetic and molecular studies (metabolic and inherited diseases).Diagnosi
MMSE Mini Mental State Examination
Trail-making test B
CDT
test di screening sviluppato
MoCA da Nasreddine et al. [1996]:
coinvolge specificamente i
Montreal domini cognitivi
Cognitive maggiormente
compromessi nel MCI
AssessmentCDT Clock Drawing Test
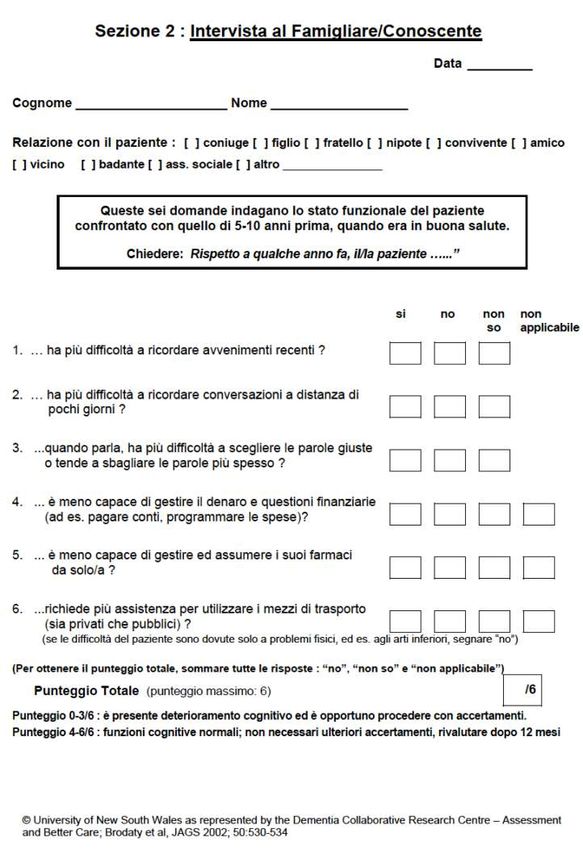
Breve test di screening per valutare le funzioni cognitive in
Medicina Generale.
2 parti:
VALUTAZIONE DEL PAZIENTE:
GP-Cog Memorizzazione e recall di informazione verbale
Orientamento temporale
Abilità visuo-spaziali
Linguaggio
INTERVISTA AL CAREGIVERGP-Cog parte 1
GP-Cog parte 2
MMSE e MoCA sono brevi test di screening cognitivo di routine
su una scala di 30 punti.
Sebbene rimanga il test più utilizzato nella pratica clinica, il MMSE
presenta degli svantaggi non trascurabili:
scarsa complessità: non è uno strumento utile ai fini della diagnosi
precoce della demenza e del riconoscimento dell’MCI, soprattutto in
MMSE vs. persone con alto livello di scolarizzazione (effetto ceiling anche in
presenza di processi patologici).
MoCA Il MoCA
sonda un numero maggiore di domini: comprende infatti prove che
indagano le funzioni esecutive (working memory e task di
concentrazione) e l’astrazione, assenti nel MMSE
prevede compiti più impegnativi (es. linguaggio)
Non sono sufficientiItem linguistici sono contenuti in tutti gli strumenti… perché?
Il linguaggio: Le demenze evidenziano, al loro esordio, una compromissione
linguistica. Uno dei primissimi sintomi
un possibile Il Linguaggio, in quanto comportamento cognitivo complesso è
vettore per la un buon candidato per essere MARKER CLINICO di
deterioramento cognitivo, anche nelle fasi pre-cliniche!
diagnosi
BIOMARKER : «caratteristica oggettivamente misurabile,
precoce? considerabile un indicatore di un processo biologico normale, di un
processo patogenico o le risposte farmacologiche ad un intervento
terapeutico»
[Biomarkers Definitions Working Group, 2001]Alzheimer
Il linguaggio presente all’onset un disordine linguistico, ingravescente
nelle patologie Liv. semantico-lessicale: deterioramento della memoria semantica,
con problemi di word-finding (cfr. anomie e parafasie semantiche),
dementigene deficit di comprensione a livello frasale, diminuzione della fluenza
verbale, bassa informatività
Liv. fonetico: abbassamento della velocità di eloquio, alto numero di
esitazioni
Review: Liv. morfo-sintattico : le frasi sono corrette ma progressivamente
Taler & Philips,2008 subiscono una riduzione/semplificazione, saltuari errori di flessione
Boschi et al., 2017 Liv. pragmatico: difficoltà nella coesione referenziale e temporale,
problemi di coerenza e di pianificazione del discorso
Con la progressione della malattia i sintomi linguistici diventano
pervasivi:
Breakdown completo nella comprensione
Produzione ristretta a ecolalia e stereotipie Afasia Progressiva Primaria: deficit selettivo linguistico all’onset
(primi due anni)
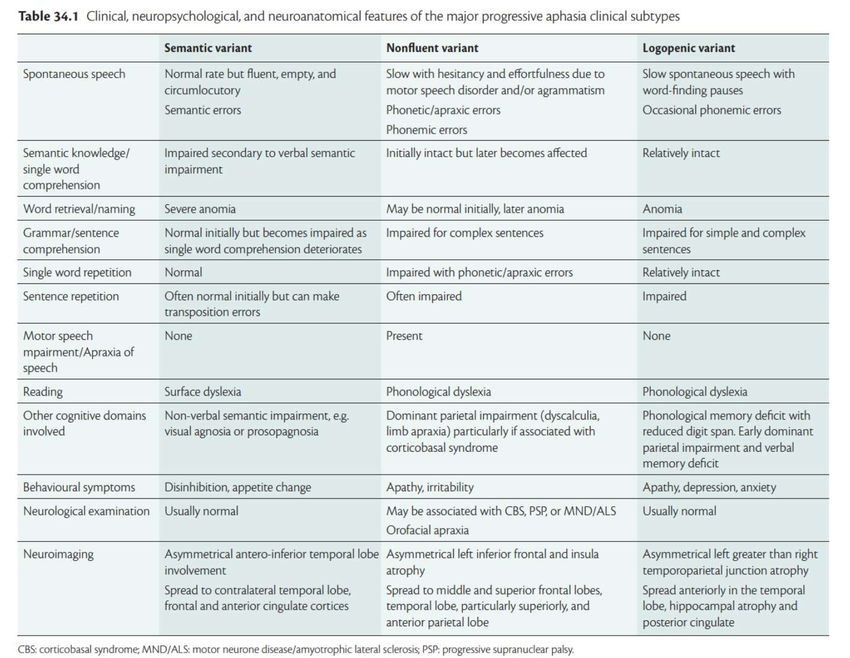
Il linguaggio 3 VARIANTI [Gorno-Tempini et al., 2011]
«Non fluente»/ «agrammatica»
nelle patologie «Semantica» (o «demenza semantica»)
«Logopenica»
dementigene
Pattern di atrofia
Sintomi
Review:
Taler & Philips,2008
Boschi et al., 2017Afasia Progressiva Primaria e Demenza semantica
OPLON [OPportunities for active and healthy LONgevity”, Smart
Cities and Communities – DD 391/RIC]:
sviluppare strumenti di diagnosi precoce della fragilità finalizzati alla
prevenzione del declino e alla promozione della salute dei soggetti
anziani.
Modulo con due obiettivi:
NEUROPSICOLOGICO: sondare l’effettiva abilità diagnostica dei
Lo studio principali strumenti psicometrici utilizzati nella pratica clinica
LINGUISTICO: identificare marker linguistici in grado di
discriminare i pazienti cognitivamente normotipici rispetto ai
soggetti affetti da decadimento cognitivo
Tecnica: NLP, identificazione automatica di parametrici acustici,
ritmici, lessicali e sintattici
[Roark et al., 2011; Satt et al., 2013; König et al., 2015]
Lo studio è stato approvato dal Comitato Etico dell’Azienda Ospedaliera di Reggio Emilia (n. 2013/0013438). 96 partecipanti
48 maschi; 48 femmine
età (range): 50 - 75
scolarità: licenza media (8 y.e.) o licenza elementare (5 y.e.) con
buona stimolazione intellettiva nel corso della vita
2 gruppi:
Lo studio: il Control Group (CG): 48 soggetti
Pathological Group (PG): 48 soggetti
campione a-MCI 16 soggetti
md-MCI 16 soggetti
early Dementia: 16 soggetti
Alzheimer 6
FTD 3
Mista 6
Corpi di Levy 1Lo studio: il
campione
no age differences were observed between the subgroups,
while the level of education of the eD group is significantly
lower compared with the CG (p-value: 0.0171).Lo studio: il campione
Intervista anamnestica
Informazioni anagrafiche; lavoro; figli; familiarità per patologie
neurodegenerative; storia clinica e farmacoterapia
Valutazione neuropsicologica
Domini cognitivi indagati: logica, memoria, attenzione, linguaggio,
abilità visuo-spaziali, abilità prassiche, funzioni esecutive
Strumenti standardizzati:
Lo studio: Mini Mental State Examination (MMSE);
Fluenza Verbale: Fonemica (PF) e Semantica (SF)
valutazione Clock Drawing Test (CDT),
neuropsicologica Montreal Cognitive Assessment (MoCA);
General Practitioner Assessment of Cognition (GPCog);
Paired Associate Learning (PAL, subtest del Cambridge Neuropsychological
Test Automated Battery – CANTAB
Questionario sulla Riserva Cognitiva (Cognitive Reserve Index
Questionnaire, CRI-q
Correzione dei punteggi grezzi di MMSE, MoCA, PF e SF per età e
scolarità, come indicato nelle relative procedure di standardizzazione Registrazione dell’eloquio spontaneo durante alcuni compiti:
1. «Descrivi questa immagine».
L’immagine (tratta da Esame del Linguaggio – II [Ciurli et al., 1996]), in
bianco e nero, ritrae un salotto nel quale vi sono una donna, un uomo, due
bambini ed un gatto che compiono alcune semplici azioni (ad es. guardare
la televisione, giocare con dei cubetti, ecc.).
1. «Descrivi una giornata lavorativa»
Elicitazione 2. «Descrivi l’ultimo sogno che ricordi»
delle Oltre ad elicitare la verbalizzazione, questi compiti permettono di
valutare l’eventuale compromissione delle funzioni mnesiche. In
verbalizzazioni tutte e tre le prove è importante :
ricordare ciò che si sta dicendo (memoria di lavoro),
spontanee ricordare ciò che si è già riferito (memoria episodica) o si vorrà
raccontare (memoria prospettica);
conoscere il significato dei termini utilizzati (memoria semantica)
avere ricordi rispetto al passato più o meno remoto (memoria
autobiografica recente e remota).
Registratore: Olympus—Linear PCM Recorder LS-5 (in WAV files; 44.1
KHz, 16 bit) Trascrizione ortografica allineata con Transcriber
Output files: .trs extension (xlm); codifica dei caratteri in Unicode UTF-8 character
encoding.
Unità di allineamento: ENUNCIATO
”the linguistic counterpart to the speech act”: the minimal linguistic entity that is
pragmatically interpretable” [Austin, 1962].
Criterio di identificazione: percezione dei break prosodici [Cresti and Moneglia,
2001]
Annotazione di fenomeni paralinguistici e extralinguistici
Tag racchiusi tra parentesi quadre per una rapida rimozione [Leech, 2005]
Trascrizione Tokenizzazione
Lemmatizzazione, PoS tagging e Parsing a dipendenze
Turin University Linguistic Environment TULE [Lesmo, 2007]
TUT - Turin University TreeBank tagset [Bosco et al., 2000]
Revisione manuale: DGA - Dependency Grammar Annotator
Annotazione
semi-
automatica Calcolo indici linguistici e stilometrici descritti in letteratura (e
risultati significativi negli studi condotti su lingue diverse
dall’italiano) oppure creati ex novo.
Le misure acustiche vengono calcolate direttamente sul segnale
vocale, utilizzando un Voice Activity Detector (”ssvad” [Mak and Yu,
2014]).
Le features Segmentazione e identificazione delle zone di speech nel segnale
Trascrizione fonetica allineata (Kaldi-DNN-ASR package, allenato sul
corpus APASCI [Angelini et al., 1994])
I tratti lessicali e sintattici sono stati invece derivati dall’annotazione
automatica revisionata manualmente dal linguistaFeature Description Refs
Silence segments duration Silence segments of the signal identified using a voice activity detector (VAD). Mean, median and Std. Satt et al., 2013
Deviation were taken into account.
Speech segments duration Speech segments of a signal identified using a voice activity detector (VAD). Mean, median and Std. Satt et al., 2013
Deviation were taken into account.
Temporal regularity of voiced The measure captures the temporal structure of the voiced segments, providing information on the rate Satt et al., 2013
segment of change in the different spectrum bands.
To calculate the temporal regularity of voiced segment durations, we used the sequence of the duration
values, and calculated the real cepstrum of the sequence (i.e. the result of taking the inverse Fourier
transform of the logarithm of the estimated spectrum of a signal).
Verbal Rate The number of words in the sample divided by the Total Locution Time (i.e. speech time including Singh et al., 2001;
pauses). Roark et al., 2011
#words/TLT
Transformed Phonation Rate “The arcsine of the square root of the Phonation Rate.” Singh et al., 2001;
arcsin (√PR ). Roark et al., 2011
Where PR is the phonation rate
PR = TPT/TLT
Le features TPT: total phonation time (i.e. speech time without pauses)
TLT: total locution time (i.e. speech time including pauses).
The arcsin transformation (or “angular transformation”) provides a normally distributed measure within
each participant group.
Standardized Phonation Time The number of words in the sample divided by the total phonation time (i.e. speech time excluding Singh et al., 2001;
pauses). Roark et al., 2011
Livello acustico Standardized Pause Rate
#words/TPT
The number of words in the sample divided by Pauses. Singh et al., 2001;
Roark et al., 2011
#words/#pauses
Root Mean Square energy Physically, energy is a measure of “how much signal” exists at any one time, and it is used in continuous López-de-Ipiña et al.,
speech to detect voiced sounds, which have higher intrinsic energy than unvoiced segments. 2013
The energy of a signal is typically calculated by windowing the signal at a particular time, squaring the
samples and taking the average. The square root of this result is the engineering quantity known as the
root-mean square (RMS) value.
Mean and Std. Deviation of the measures were taken into account.
Pitch Pitch is the main acoustic correlate of tone and intonation, and the perceptual correlate of frequency; as López-de-Ipiña et al.,
a matter of fact, it depends on the number of vibrations per second produced by the vocal cords. 2013
Mean and Std. Deviation were taken into account.
Spectral Centroid The measure captures the perceptual brightness of a sound. It is obtained by evaluating the “centre of López-de-Ipiña et al.,
gravity” of the spectrum using the Fourier transform’s frequency and magnitude information. 2013
Mean and Std. Deviation were taken into account.
Higuchi Fractal Dimension The feature describes the complexity of the signal. The algorithm measures fractal dimension (i.e. self- López-de-Ipiña et al.,
similarity, namely identical/similar structures repeating over a pattern) of discrete time sequences 2013
directly from time series.
Mean and Std. Deviation were taken into account.Feature Description Refs
Percentage of vocalic intervals The proportion of vocalic intervals within the utterance, that is, the sum of vocalic Ramus et al., 1999
intervals divided by the total duration of the utterance.
Std. deviation of vocalic and The standard deviation of the duration of vocalic and consonantal intervals within Ramus et al., 1999
consonantal interval durations each utterance, noted as ΔV and ΔC.
Pairwise Variability Index, raw and This rhythm metric takes into account the temporal succession of the vocalic and Grabe & Low, 2002
normalized consonantal intervals instead of joining all the values and calculating the standard
deviation. It is based on a pairwise comparison of the durations of either two vocalic
or consonantal intervals, therefore expressing the level of variability in consecutive
measurements.
• Raw Pairwise Variability Index (rPVI):
⎡m −1 ⎤
Le features r PVI = ⎢∑ dk − dk + 1 / ( m −1)⎥
⎣ k =1 ⎦
where m is number of intervals, vocalic or intervocalic, in the text and d is the
duration of the kth interval.
• Normalised Pairwise Variability Index (nPVI):
Livello ritmico n PVI = 100 ×
⎡m −1
⎢∑
d k − d k +1
⎢ k =1 (d k + d k +1 ) / 2
/ ( )⎥⎥
m −1
⎤
⎣ ⎦
Variation coefficient for ΔV and ΔC A variation coefficient (“varco”) is a value describing relative variation. VarcoΔC is Dellwo, 2006
calculated as the percentage of the ΔC of the average duration of intervals (meanC);
analogously, VarcoΔV is calculated as the percentage of the ΔV of the average
duration of intervals (meanV).
VarcoΔC= ΔC*100/meanC
VarcoΔV= ΔV*100/meanVFeature Description Refs
Content Density The ratio of open-class words to closed-class words. The measure is calculated over Part of Speech tags, Roark et al., 2011
where open-class words are nouns, verbs, adjectives, adverbs; the rest are considered closed-class words.
Content Density=OCW/ CCW
Part-of-Speech rate This class of features investigates the average rate of occurrence for each part-of-speech (PoS) category: Holmes & Singh,
Adjectives, Adverbs, Articles, Conjunctions, Interjections, Nouns, Numerals, Prepositions, Pronouns, Verbs. 1996;
e.g.: #Adjectives/#words Bucks et al.,
2000;
Reference Rate to Reality The ratio of the total number of nouns to the total number of verbs. Vigorelli, 2004
RefRReal = #Nouns/#Verbs
Personal, Spatial and Temporal Deixis The feature probes the rate of deictic expressions in the spoken text (i.e. linguistic elements that point to the March et al.,
rate time, place, or situation in which a speaker is speaking; in other words, their denotational meaning varies 2006; Cantos-
depending on extralinguistic context). The main types of deixis are: Gomez et al.,
• Person deixis (e.g. I, you, we, me, mine, yours…) 2009
• Place deixis (e.g. here, there, this, that…)
• Time deixis (e.g. now, today, tomorrow, soon…)
e.g.: #PersonDeixis/#words
Relative pronouns and negative The rate of Relative Pronouns (e.g. who, whose…) and Negative Adverbs (e.g. not, neither…) in the spoken
adverbs rate text.
Le features Lexical Richness: Type-Token Ratio, W This class of measures quantifies the richness of vocabulary/lexical diversity.
- Brunet’s Index and R - Honoré’s
Statistic Type-Token Ratio: the ratio of the number of different words (vocabulary - V) to the total text length.
Holmes & Singh,
1996;
Brunet, 1978;
TTR is dependent on the text size: it is bigger when texts are small and decreases as the texts get larger. Honoré, 1979;
W - Brunet’s Index: it quantifies lexical richness without being sensitive to text length. It is calculated
Livello lessicale according to the following equation:
W = N V(-.165)
where N is the total text length and V is the total vocabulary used by the participant.
This measure generally varies between 10 and 20. The lower the value, the richer the speech.
R - Honoré’s Statistic: calculates lexical richness by highlighting the proportion of words that are used only
once with reference to the total number of words in the text: the larger the number of words used by a
speaker that occur only once (hapax legomena), the richer the lexicon.
R = 100logN/(1-V1/V)
where V1 is the words spoken only once, V is the total vocabulary used and N is the total text length.
High value of R suggests a rich vocabulary used by the speaker.
Action Verbs rate The metric probes the rate of action verbs (i.e. verbs referring to physical action, like to put, to run, to eat) in
the spoken text.
Frequency-of-use tagging Mean frequency-of-use weight among words extracted from the De Mauro’s frequency list. De Mauro, 2000;
Propositional Idea Density Idea density is the number of expressed propositions (i.e. distinct facts or notions contained in a text) Snowdon et al.,
divided by the number of words. It is a measure of the extent to which the speaker is making assertions (or 1996; Roark et
asking questions) rather than just referring to entities. al., 2011
In this feature, propositions correspond to verbs, adjectives, adverbs, prepositions, and conjunctions. Nouns
are not considered to be propositions, as the main verb and all its arguments count as one proposition.
Mean Number of words in utterances Mean number of words in the speech utterances.Feature Description Refs
Number of dependent elements The feature explores Noun Phrase complexity, counting the number of dependent
linked to the noun elements linked to the head (e.g. Adjectives, Relative clauses…).
U.M: words Mean and Std. Deviation were taken into account.
Global Dependency Distance Given the memory overhead of long distance dependencies, the feature Roark et al., 2007; 2011
U.M: pure number quantifies the difficulty in syntactic processing.
Mean and Std. Deviation were taken into account.
Syntactic complexity Syntactic complexity is established by counting the linguistic tokens that can be Szmrecsanyi, 2004
U.M: pure number considered to telltale signs of increased grammatical subordinateness and
embeddedness, such as:
1. subordinating conjunctions (e.g. because, since, as, when, that, etc.);
Le features 2.
3.
4.
WH- pronouns (e.g. who, whose, whom, which);
verb forms, both finite and non-finite;
noun phrases.
Because subordinators and WH-pronouns are the most straightforward indicators
of increased embeddedness (and thus of high complexity), these features are
weighted more heavily than verb forms and noun phrases.
(2*CONJ+2*PRON+NOUNS+VERBS)/#word
Livello sintattico Syntactic embeddedness: maximum
depth of the structure
Syntactic complexity is also assessed by evaluating the “embeddedness”, i.e. the
maximum “depth” of the structure.
Mean and Std. Deviation were taken into account.
Utterance length Mean Length of utterance corresponds to the average number of words for
U.M: word/utterance utterance. It is calculated by counting the number of words in each utterance
divided by the total number of utterances.
Mean and Std. Deviation were taken into account. Comparazione delle performance nei test neuropsicologici e delle
differenze nei tratti linguistici
TEST NON PARAMETRICI
Analisi Mann-Whitney U-test: eD vs. CG
Kruskal-Wallis test (e test di Dunn, confronti multipli): aMCI vs.
statistica mdMCI vs. CG.
Entrambi: due code (“two-sided”)
Livello di significatività: p < 0.05
Software: the Prism version 6.0 [GraphPad, La Jolla, CA]Risultati 1. Esame neuropsicologico
Risultati 2. Esame del linguaggio spontaneo
Risultati 2. Esame del linguaggio spontaneo
Risultati 2. Esame del linguaggio spontaneo
Il livello acustico è quello più alterato. I parametri significativi
indagano caratteristiche temporali (es. silence segments duration,
speech segments duration, transformed phonation rate, standardized
pause rate) e proprietà spettrali della voce (Higuchi Fractal
dimension e spectral centroid).
Il livello acustico non risulta intaccato dalla patologia
Eccezione: task del “sogno”, per aMCI e mdMCI
I parametri lessicali, che cercano di catturare compromissioni della
conoscenza lessicale e/o di retrieval, risultano alterati
Discussione In particolare è ridotta la content density (“the ratio of open-class
words to closed-class words”), soprattutto per il task della figura, sia in
a-MCI che in mdMCI
Tendenza ad un globale impoverimento delle produzioni dal punto di
vista lessicale
Gli enunciati rimangono formalmente corretti
Parametri sintattici, pensati per catturare la complessità degli
enunciate, sono significativi
Gli enunciati del gruppo PG sono corretti, ma contengono meno
relazioni complesse tra sintagmi e strutture incassate proof-of-concept: l’analisi computazionale delle produzioni
parlate spontanee è in grado di identificare alterazioni non
rilevabili dalla testistica tradizionale
Strumento promettente per l’identificazione precoce del
deterioramento cognitivo
Ecologico
Applicabile su larga scala
Discussione A basso costo
Indicazione sul task da somministrare:
La descrizione di figura complessa è il più usato in letteratura
Il racconto del ”sogno” e della “giornata lavorativa” sembrano essere
task più sensibili: richiedono utilizzo della memoria e la produzione
di narrazioni , sintatticamente più strutturate Conferma delle ipotesi: necessario uno studio longitudinale
(follow-up)
Costruzione di un prototipo di classificatore machine learning
Sviluppi… Lungo periodo: realizzazione di un dispositivo per i medici di
base
Obiettivo: SCREENING, individuazione precoce dei soggetti da
inviare ad accertamenti neuropsicologiciPuoi anche leggere