Innovazioni farmacologiche nella depressione - Giuseppe Lanza U.O.C Neurologia IC - More ...
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
Innovazioni
farmacologiche
nella depressione
Giuseppe Lanza
U.O.C Neurologia IC
I.R.C.C.S. “Oasi Maria SS.”
Troina (EN)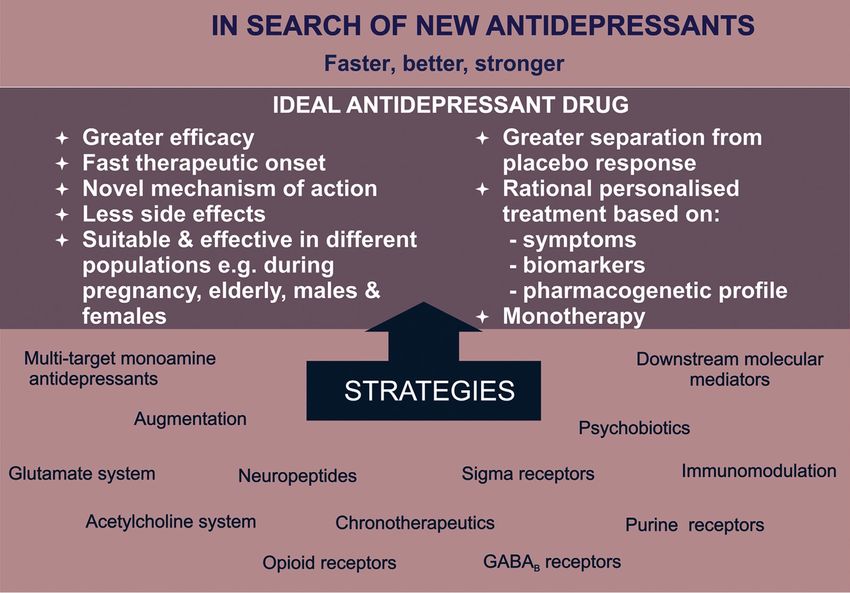
Depression is a common psychiatric comorbidity of most neurological disorders (20- 50%), especially among patients with stroke, Multiple Sclerosis, epilepsy, Parkinson's disease and dementia. Depression is an independent predictor of poor quality of life, and has a negative impact on the response to treatment, course and recovery of neurological deficits. Depression may predate the development of some neurodegenerative disorders, and depressive illness itself may be a risk factor for dementia. Treatment of depression should be part of the management of neurologic disorders. Trials of treatment and new drugs are urgently needed.

“Screening for depression in the outpatient clinic”
“I neurologi ambulatoriali dovrebbero avvalersi di
strumenti di screening per identificare eventuale presenza
o co-morbidità di depressione nei loro pazienti.”
Kanner AM. Epilepsy Behav 2005
LIMITI:
- la maggior parte delle scale cliniche per la depressione ha valore di screening;
- molte scale risentono della componente somatica e/o vegetativa della
depressione;
- un adeguato follow-up non è sempre possibile;
- bassa compliance alla terapia, con alto rischio di discontinuation e di
“antidepressant roulette”.
La diagnosi definitiva richiede sempre una valutazione
specialistica clinico-strumentale multidisciplinare.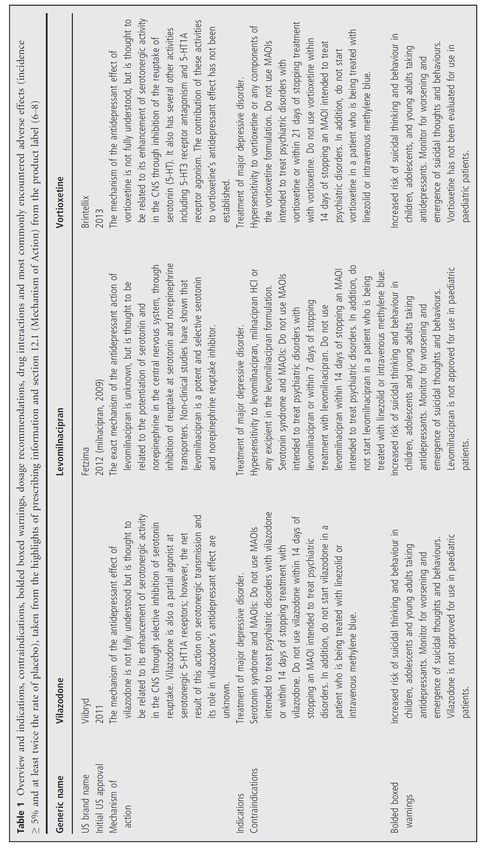
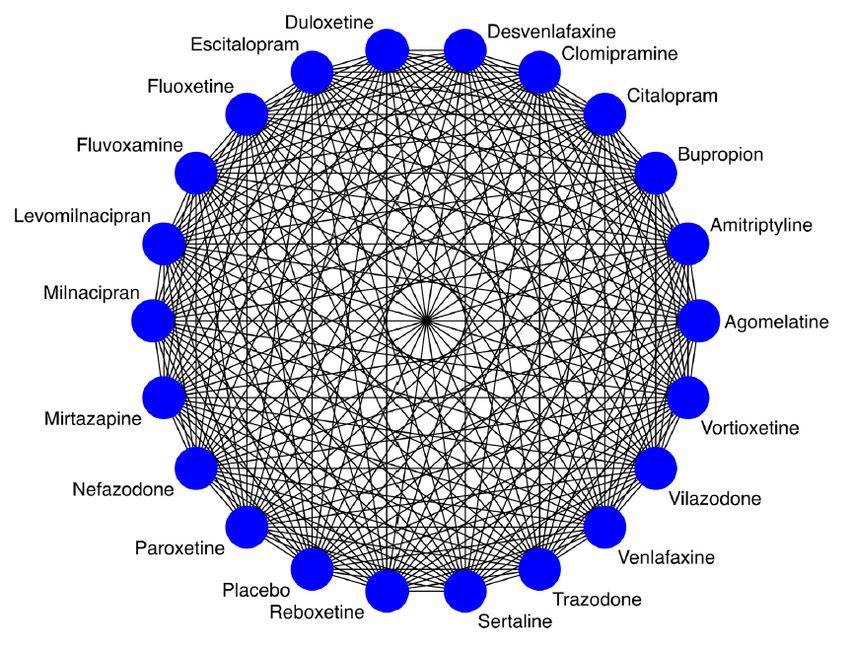
FARMACI ANTIDEPRESSIVI
Noradrenalina Serotonina
Norepinephrine reuptake Selective serotonin
inhibitor (NARI) reuptake inhibitor (SSRI )
Tricyclic antidepressant (TCA)
Serotonin-norepinephrine reuptake inhibitor (SNRI)
Noradrenergic and specific serotonergic antidepressant
(NaSSA)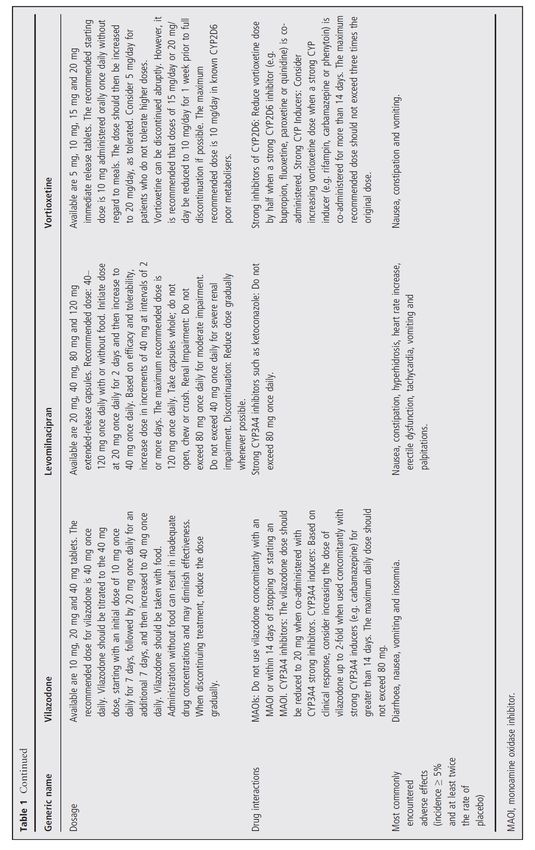
Conclusions: “antidepressants are effective for the treatment of depression in patients with neurological disorders but the evidence for the efficacy of antidepressants in improving quality of life, and functional and cognitive outcomes is inconclusive.”
POSSIBILI EFFETTI COLLATERALI DI TUTTI I
FARMACI ANTIDEPRESSIVI
Sistema Nervoso Centrale
Cardiovascolari Sedazione, sonnolenza
Compromissione cognitiva
Ipertensione arteriosa
Insonnia, sonnolenza, irritabilità
Aritmie (↑ QT)
Cefalea, tremore
Tachicardia
Inappetenza/iperfagia
Gastrointestinali
Urogenitali Nausea, vomito
Stipsi, diarrea
Disfunzione erettile Dispepsia
Disturbi eiaculazione
Anorgasmia
Priapismo Sistema Nervoso Autonomo
Secchezza delle fauci
Ritenzione urinaria
Sudorazione
Ipotensione ortostatica
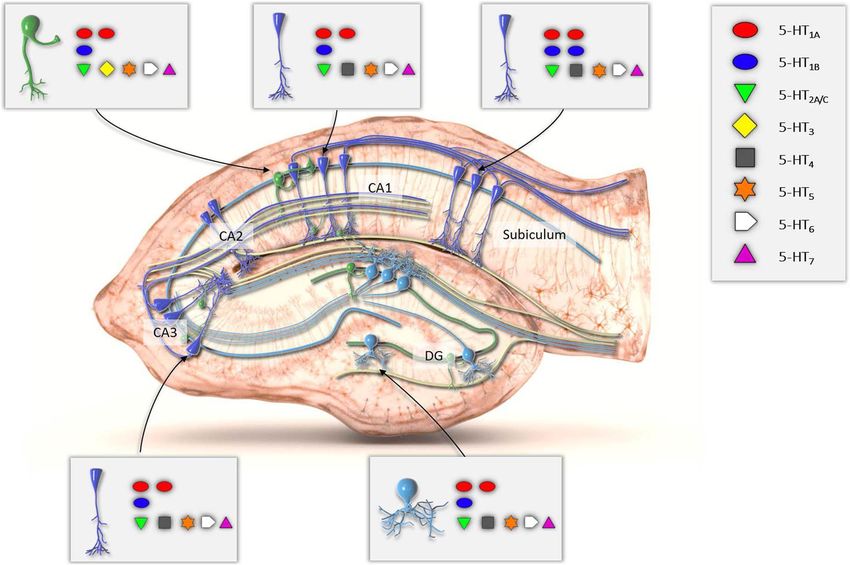
Serotonin modulator and stimulator (SMS) • SMS, or more simply “serotonin modulator”, is a multimodal drug specific to the serotonin neurotransmitter system. SMSs simultaneously modulate one or more serotonin receptors and inhibit the reuptake of serotonin. • Antidepressant vortioxetine acts as a serotonin reuptake inhibitor (SRI), partial agonist of the 5-HT1A receptor, and antagonist of the 5-HT3 and 5-HT7 receptors. • SMS can also technically be applied to vilazodone, which acts as an SRI and 5- HT1A receptor partial agonist. • SMSs were developed because there are many different subtypes of serotonin receptors (at least 15 in total), although not all of these receptors appear to be involved in the antidepressant effects of SRIs. Antagonism of 5-HT3 – a receptor that is involved in the regulation of nausea, vomiting, and the gastrointestinal tract – could counteract the undesirable increase in activation of this receptor mediated by SRIs.
• L’efficacia e la sicurezza di vortioxetina
sono state studiate in un programma
clinico che ha incluso più di 6.700
pazienti, dei quali più di 3.700 trattati
con vortioxetina in studi a breve termine
(≤12 settimane) (Depressione Maggiore)
(1,2 )
• Considerando anche gli studi condotti dopo la registrazione: 9.900 pazienti (3 )
1)RCP Vortioxetina2) European Medicines Agency (EMA) Assessment Report
(EPAR). Brintellix (vortioxetine). Assessment report for an initialmarketing
authorisation application. 24th October 2013. 3) Melander H et al. Eur
Neuropsychopharmacol 2008; 18:623-627Vortioxetina: efficacia nel trattamento della depressione in acuto (11 studi e
ntot circa 5.600 pazienti)
Variazione rispetto al basale del punteggio della scala MADRS a 6/8 settimana (FAS, MMRM)
In sintesi:1-12
• La metanalisi di 11 studi a breve termine
conferma l’efficacia di vortioxetina a 5,
10 e 20 mg/die, con effetto dose-
dipendente e su un ampio spettro di
sintomi depressivi.
In sintesi 1-12
• Una differenza di almeno 2 punti
rispetto a placebo nella variazione vs
basale della scala MADRS viene
considerata clinicamente rilevante
n vortioxetina: 2.700
n placebo: 2.812
RCP: La dose iniziale per gli adulti è 10 mg/die.
In base alla risposta individuale la dose può essere incrementata fino
ad un massimo di 20 mg/die o ridotta ad un minimo di 5 mg /die.
La minima dose efficace di 5 mg /die
per i pazienti di età ≥ 65 anni. Cautela quando si trattano pazienti
anziani con dosi > 10mg/die
← Effetto migliore Effetto peggiore → 11 .European Medicines Agency (EMA) Assessment Report
rispetto a placebo rispetto a placebo (EPAR). Brintellix (vortioxetine). Assessment report for an initialm
1. Alvarez et al. 2012; 2. Baldwin et al. 2012; arketing authorisation application. 24th October 2013.
3. Henigsberg et al. 2012; 4. Boulenger et al. 2013;
5. Mahableshwarkar et al. 2015; 6. Jacobsen et al. 2015;
7. Jain et al. 2013; 8. Mahableshwarkar et al. 2013;
9. Mahableshwarkar et al. 2015; 10. Katona et al. 2012;
11. Vortioxetine EPAR; 12. McIntyre et al. 2014;Vortioxetina: efficacia nel trattamento della
depressione nel paziente anziano
Disegno dello studio
Studio multicentrico, randomizzato, in doppio cieco, controllato vs placebo
452 pazienti età >= 65 anni con MDD suddivisi in tre gruppi di trattamento:
• Vortioxetina 5 mg/die
• Duloxetina 60 mg/die (gruppo di controllo attivo)
• Placebo
Durata del trattamento: 8 settimane
Obiettivo dello studio: verificare l’efficacia e la tollerabilità di una dose fissa di
Vortioxetina 5 mg/die in pazienti anziani con MMD
RCP 2016: La dose minima efficace di 5mg/die di vortioxetina deve essere sempre utilizzata come
dose iniziale per i pazienti di età >=65 anni. Cautela quando si trattano pazienti di età superiore
ai 65 anni con dosi superiori ai 10 mg/die rispetto ai quali i dati sono limitati
Katona et al. International Clinical Psychopharmacology 2012; 27(4): 215-223Risultati: analisi esplorativa predefinita sulle funzioni cognitive
Effect size standardizzato vs. placebo
Funzioni
esecutive
Velocità
Psicomotoria/
rapidità di processamento
Memoria
Attenzione
Standardized effect sizes of Lu AA21004 5 mg/day and duloxetine
60 mg/day compared with placebo on the Digit Symbol Substitution
Test (DSST) and the Rey Auditory Verbal Learning Test (RAVLT). Katona et al. Int Clin Psychopharmacol 2012;27:215–223
*PRisultati: analisi esplorativa predefinita sulle funzioni cognitive
Path analysis - DSST
Vortioxetina 5 mg/die
ha un effetto diretto dell’83% su DSST
(vs 26% duloxetina 60 mg/die)
Keefe et al. Poster presented at ECNP 2013
Katona et al. Int Clin Psychopharmacol 2012;27:215–223Analisi statistiche dimostrano che l’effetto di vortioxetina sulle
funzioni cognitive è indipendente dall’effetto antidepressivo
• Analisi post-hoc hanno inoltre
evidenziato benefici significativi sulle
Protocol-specified path analysis performance cognitive di vortioxetina vs
placebo in pazienti che erano:
Effetto diretto 64%
(95% CI: 47–82%; p=0.0007)
Vortioxetina Composite
– non-responders per il punteggio della
10 mg z-score
scala MADRS
Effetto
– non-remitters
indiretto 36% (MADRS punteggio totale>10)
MADRS
L’effetto positivo di
vortioxetina sulle funzioni
Effetto cognitive è indipendente dal
indiretto 52%
miglioramento alla MADRS
Vortioxetina
Composite
20 mg
z-score
Effetto diretto 48%
(95% CI: 23–73%; p=0.0246) Questi risultati confermano i
risultati dello studio di Katona
et al.2012
The ‘direct effect’ claim is a medical statement supported by published data
CI=confidence interval;
MADRS=Montgomery–Åsberg Depression Rating ScaleVortioxetina: efficacia nel trattamento della depressione in
pazienti che non avevano risposto a terapia precedente
Risultati: variazione del punteggio della scala MADRS vs basale
**pVortioxetina: l’efficacia in acuto è mantenuta
nel tempo
Risultati: Punteggio medio MADRS ad ogni visita (FAS, OC; endpoint
LOCF)
Remissione (MADRS≤10): 83%
Remissione (MADRS≤10): 42%
Baldwin et al. Curr Med Res Opin 2012;28(10):1717–1724
In the extension study, all patients received 5 mg/day during the first week; 57% of the patients subsequently increased their dose to 10 mg/day.Vortioxetina: efficacia nella prevenzione delle
ricadute
Risultati
Endpoint primario: tempo alla ricaduta entro le prime 24 settimane del periodo in doppio
cieco (punteggio MADRS ≥22 o risposta terapeutica insufficiente a giudizio del clinico).
Vortioxetina è efficace nel prevenire le ricadute; 50% di rischio in meno di ricadere per
pazienti che continuano l’assunzione di vortioxetina vs. placebo (13% vs 26%, p=0.0013)
Boulenger et al. J Psychopharmacol 2012;26(11):1408–1416Levomilnacipran (1S, 2R-milnacipran) is a potent and selective serotonin–norepinephrine reuptake inhibitor (SNRI) with greater potency for inhibition of norepinephrine relative to serotonin reuptake. It was approved for the treatment of major depressive disorder (MDD) by the US Food and Drug Administration (FDA) on 2013. Levomilnacipran is an active enantiomer of the racemic drug milnacipran, which is approved by the US FDA for the management of fibromyalgia and in other countries for the treatment of MDD.
THE DAY AFTER TOMORROW…
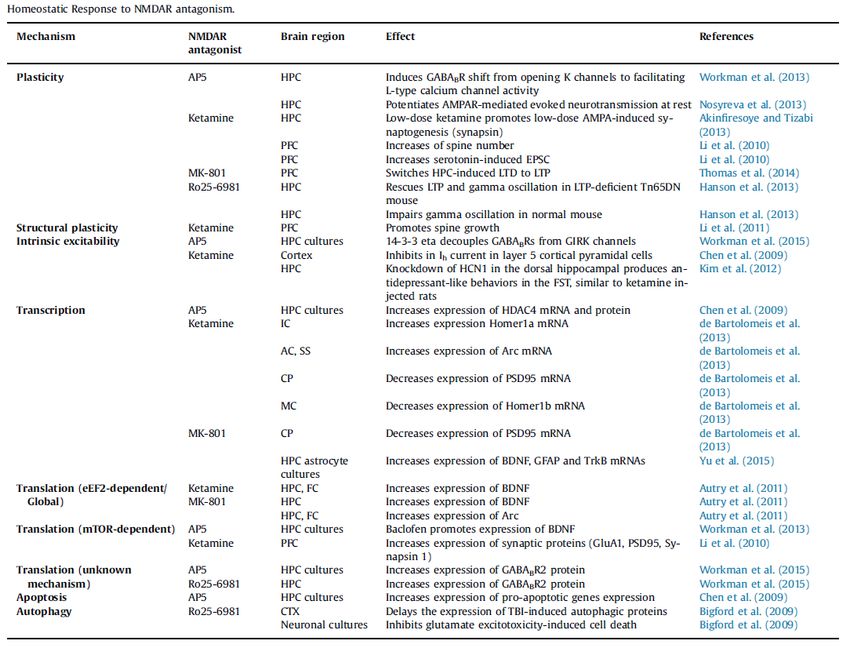
5HT3Rs located on the serotonergic and other neurotransmitter interneuronal projections control their release and affect mood and emotional behavior. Apart from modulating the neurotransmitter functions, 5HT3R antagonists have protective effects in the pathogenic events including hypothalamic–pituitary–adrenal- axis hyperactivity, brain oxidative stress and impaired neuronal plasticity.
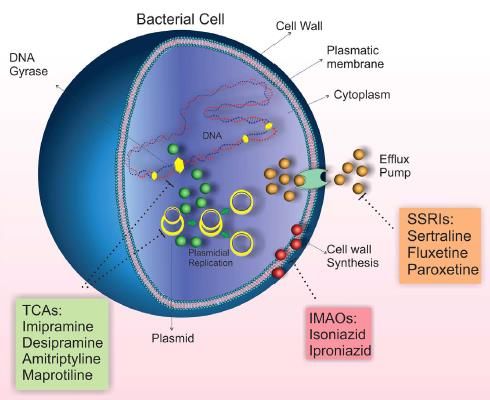
Microbiota– gut–brain axis for brain functioning and behavior in health and disease
MDD is associated with changes in gut permeability and microbiota composition. In this respect, antidepressant drugs present antimicrobial effects that could also be related to the effectiveness of these drugs for MDD treatment. Conversely, some antimicrobials pr esent antidepressant effects.
1) ALKS 5461 11) JNJ-42847922
Mechanism: Mu partial agonist/kappa antagonist Mechanism: OX2 receptor antagonist
Status: Phase III clinical trials Status: Phase I clinical trials
2) Amitifadine (DOV-21,947 or EB-1010) 12) Ansofaxine HCl (LY03005)
Mechanism: SNDRI Mechanism: SNDRI
Status: Phase III clinical trials Status: Phase I clinical trials
3) AV-101 (4-Cl-KYN) 13) LY2940094
Mechanism: NMDA receptor antagonist Mechanism: NOC-1 antagonist
Status: Phase II clinical trials Status: Phase II clinical trials
4) AVP-786 14) Mifepristone (RU-486)
Mechanism: NMDA/sigma-1 receptor antagonist Mechanism: Antiprogestogen /
Status: Phase II clinical trials antiglucocorticoid
5) AZD6423 Status: Phase III clinical trials
Mechanism: NMDA receptor antagonist 15) MIN-117
Status: Phase I clinical trials Mechanism: SDRI / 5-HT1A receptor antagonist
6) Basimglurant (RG7090) Status: Phase II clinical trials
Mechanism: mGluR5 antagonist 16) NRX-1074
Status: Phase II clinical trials Mechanism: NMDA receptor partial agonist
7) Botox (onabotulinumtoxinA) Status: Phase II clinical trials
Mechanism: Facial nerve inhibitor 17) NSI-189
Status: Phase II clinical trials Mechanism: Neurogenesis
8) CERC-301 Status: Phase I clinical trials
Mechanism: NR2B antagonist 18) Rapastinel (GLYX-13)
Status: Phase II clinical trials Mechanism: NMDA receptor modulator
9) DSP-1053 Status: Phase II clinical trials (complete)
Mechanism: SSRI / 5-HT1A partial agonist 19) Strada (MSI-195 or Ademetionine)
Status: Phase I clinical trials Mechanism: Methylation
10) Esketamine (Intranasal Ketamine) Status: Phase II clinical trials
Mechanism: NMDA receptor antagonist 20) Tedatioxetine (Lu AA24530)
Status: Phase II clinical trials Mechanism: SNDRI
Status: Phase II clinical trialsNel 2008 la Food and Drug Administration statunitense ha approvato la Stimolazione Magnetica Transcranica ripetitiva (rTMS) nel trattamento della depressione maggiore farmaco- resistente. Attualmente, anche in Italia la tecnica è utilizzata in alcuni centri con questa indicazione.
“The neurophysiological imbalance was restored the patients treated with
active rTMS. The reported clinical benefits in the test group might be related to
the plastic remodeling of synaptic connection induced by rTMS treatment.”
“High-frequency rTMS over the left DLPFC may have long-term
antidepressant effect in drug-resistant MDD.”“Both TMS and tDCS may have potential as interventions for the treatment of symptoms associated with dementia and PD. These results are promising; however, available data were limited, and major challenges exist in order to maximise the efficacy and clinical utility”
GRAZIE
Puoi anche leggere