IL RUOLO DEL CARDIOLOGO NELLA GESTIONE DEL PAZIENTE AD ALTO RISCHIO NONOSTANTE LE RISORSE LIMITATE - GIANCARLO CASOLO, PHD, FACC - OLTRE
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

Firenze 25-26 Ottobre 2018
Il ruolo del cardiologo nella gestione
del paziente ad alto rischio
nonostante le risorse limitate
Giancarlo Casolo, PhD, FACC
Disclosures: receives honoraria for courses and seminars, including this one
Credit: UK’s National Health Service
I NUMERI DELLE MALATTIE CARDIOVASCOLARI IN ITALIA
1
Morti CV
v
Altre
morti
1 Istat, «Report, L’evoluzione della mortalità per causa: le prime 25 cause di morte», 4 maggio 2017
Percentage of the Decrease in Deaths from Age-adjusted CVD Mortality Rates, Coronary Heart Disease Attributed to 1950–2014 Treatments and Risk-Factor Changes Mensah et al. Circ Res. 2017 Ford et Al. N Engl J Med 2007

Trend in MI and use of preventive drugs Yeh et Al. N Engl J Med 2010

La salute è un valore ma ha un costo
Fonti di spesa
Prevenzione
Trattamento
Castellano et Al. JACC 2014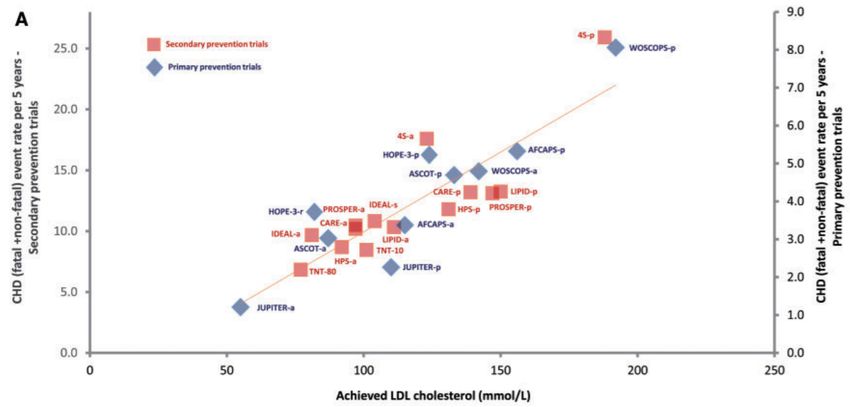
Dalla Evidence Based Medicine al concetto di
Value-Based Healthcare
• Evidence-based medicine is the conscientious explicit
and judicious use of current best evidence in making
decisions about the care of individual patients
• Value based healthcare is “the health outcomes
achieved per dollar spent”. The “best value” of an
intervention for a population
2014
The Outcome Measures Hierarchy
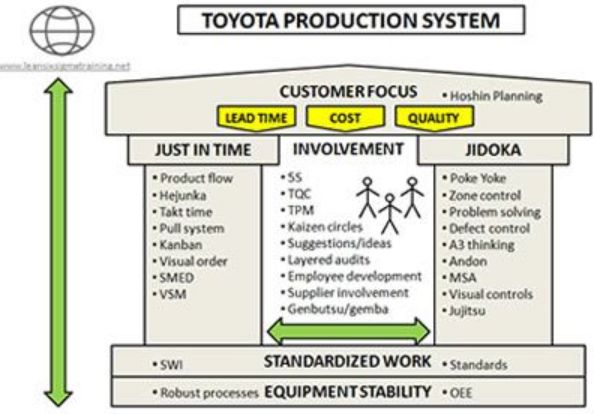
La Sanità come Azienda
(metalmeccanica)
Qualità totale attraverso il
Lean Thinking
James P. Womack and Daniel T. JonesMalintesi occorsi
• Qualità = fare le stesse cose in modo efficace
ed efficiente
• Valore = risparmio di risorse
Concentrazione su COSTI
Scarsa attenzione agli ESITI
Crescente preoccupazione ai PROMS e PREMS
Scarsa attenzione al VALORE effettivo prodottoLDL colesterolo come fattore causale della malattia
aterosclerotica
Ference et Al. Eur Heart J 2017Meta-analysis of effect of 1-mmol/L LDL-C lowering on the
risk of major vascular events & Lower is better
When examining 11 492 major vascular events, there was
a 21% relative risk reduction per 1-mmol/L (38.7-mg/dL)
reduction in LDL-C
Meta-regression of achieved
LDL-C and rate of major vascular
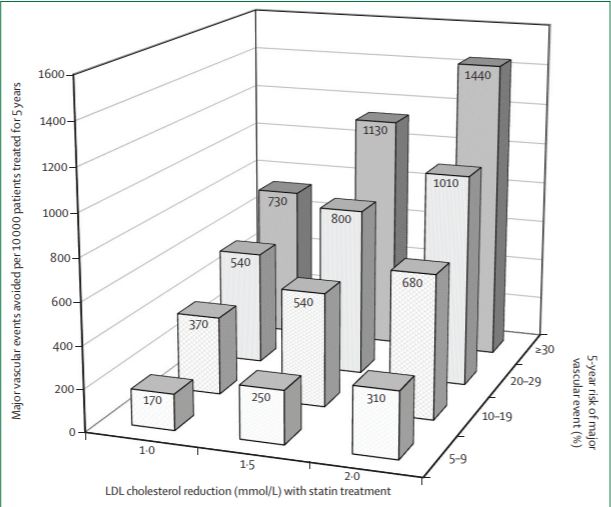
Sabatine M et Al. JAMA Cardiol 2018 eventsPredicted absolute reductions in risks of major vascular events by lowering LDL
cholesterol with statin therapy for 5 years in people at different levels of
absolute risk
Collins et Al. Lancet 2016NNT to reduce mortality, major cardiovascular (CV) events,
or myocardial infarction (MI) on a yearly basis
Known CAD
Bittl & Maron JACC 2017Total costs and health outcome in QALYs per patient
for the different treatment strategies
CAD Pts
Stam-Slob et Al. JAHA 2017Costo del trattamento se indicato dal profilo genetico
27-single-nucleotide
polymorphism cGRS
vs
No test
Jarmul et Al. Circ Cardiovasc Qual Outcomes. 2018Costi calcolati per il trattamento di un paziente con SCA
Gulizia et Al. G Ital Cardiol 2016Residual Cardiovascular Risk
Individuals categorised into five groups:
3012 Framingham Study participants
No CV disease
Lieb W, et al. Open Heart 2018Inflammation and residual CV risk
(Fourier Study)
Primary end point
Bohula et Al. Circulation 2018Controllo dei fattori di rischio in Europa Kotseva et Al. JACC 2015
UTILIZZO DI FARMACI IPOLIPEMIZZANTI IN ITALIA
Defined Daily Dose
5 Rapporto OSMED 2015UTILIZZO DI FARMACI IPOLIPEMIZZANTI IN ITALIA 5 Rapporto OSMED 2015
UTILIZZO DI FARMACI IPOLIPEMIZZANTI IN ITALIA
Aderenza all’uso
delle statine
50% c.ca
Rapporto OSMED 2015LIPID MANAGEMENT: UNMET NEEDS
Target achievement 1 Statin withdrawal 2
Achieved Goal
Did Not Achieved Goal
Cumulative incidence of all-cause mortality in
Propensity-score matched population
1. Kotseva K, et al. Eur J Prevent Cardiol. 2016;23(6):636-648., 2 Kim MC et al. Am J Cardiol. 2015 Jan 1;115(1):1-7. ,Obiettivi per il Cardiologo • Identificare i pazienti a rischio • Trattare a target • Assicurare un approccio step-by-step • Favorire la continuità terapeutica (aderenza e persistenza) con un adeguato follow-up • Avvalersi di tutte le professionalità esistenti
Cumulative Incidence of Death from Coronary Heart Disease
or Nonfatal Myocardial Infarction
…more preventive therapies were initiated in
Newby et Al. N Engl J Med 2018 patients in the CTA group- Patients’ Awareness - Therapeutic Inertia - Adherence and persistence - Side effects of drugs - Structured Follow-up - Insufficient control of known targets
The Digitized Cardiovascular Physician Visit Steinhubl RS, Topol EJ. JACC 2015
Performance of the machine-learning (ML) algorithms predicting 10-year cardiovascular disease
(CVD) risk derived from applying training algorithms on the validation cohort of 82,989 patients.
Can machine-learning improve cardiovascular risk
Weng SF, Reps J, Kai J, Garibaldi JM, Qureshi N (2017)
prediction using routine clinical data?. PLOS ONE 12(4): e0174944.
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0174944Design Thinking
Versilia GPs Network • 50 GPs • PHR • 68.000 Pts • 13.8% High Risk • Prospective registry
Conclusioni • Le risorse possono essere allocate in modo corretto rispettando il valore prodotto dal loro impiego • Sviluppare una gestione del rischio basata sul valore comporta un abbattimento degli sprechi ed un orientamento di sistema agli esiti • Il Cardiologo è chiamato a svolgere un ruolo fondamentale sia nello scenario attuale che nella costruzione di quello futuro
Puoi anche leggere