HCC NEL PAZIENTE HBV VIROSOPPRESSO - Una chimera o realtà?
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
HCC NEL PAZIENTE HBV
VIROSOPPRESSO
Una chimera o realtà?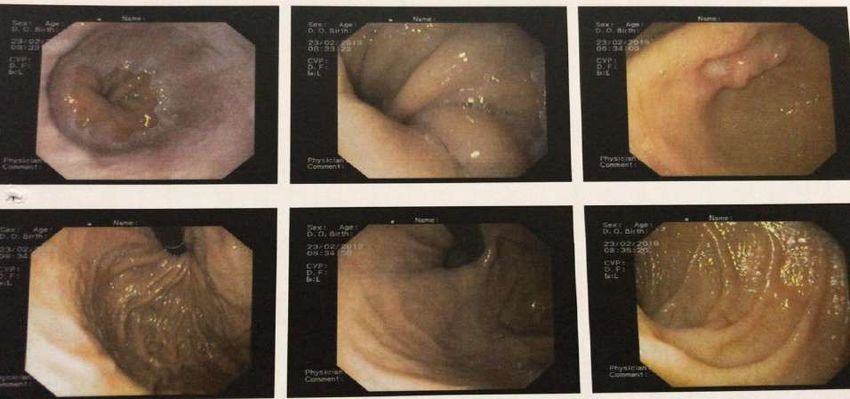
VIRTUAL CLINICAL CASE Ø Paziente maschio di 57 anni Ø HBV + da 30 anni (scoperto in seguito a donazione) Ø Impiegato Ø Alcool 50gr/die Ø Padre deceduto per cirrosi epatica. Ø Altezza 1.70m, Peso 66Kg Ø Ipertensione arteriosa

ESAMI DI LABORATORIO 2003 ALT 70 AST 91 GAMMA GT 35 FOSFATASI ALCALINA 92 BILIRUBINA 0.7 PLT 130000 ALBUMINA 4 INR 0.8 HIV neg Anti HCV neg HBsAg + Anti HBsAg - Anti HBcAg + Anti HBeAg + HBV DNA 224628

Ecografia addominale: 28/10/03 fegato di dimensioni normali ( 133 dlm) presenta discreta disomogenità ecostrutturale con echi grossolani a margini lievemente irregolari come nelle condizioni di epatopatia cronica. non lesioni focali. Microlitiasi della colecisti; vena porta e coledoco nella norma. Pancreas regolare con vicino un linfonodo reattivo. milza aumentata di dimensioni ( 126 x 42) microlitiasi renale destra. Cisti displasica sn.

Titolo asse
10
12
14
16
0
2
4
6
8
Lam
2003
2004
2004
2005
Lam-Adv
242473
2006
2007
IRC
2008
Entecavir
2009
2010
2011
2012
2013
250
HBV DNA
200
400
600
800
0
1000
1200
1400
1600
2003
2004
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2016
2018
2018
2018
alfafeto
2016 alfafetoproteina 68.9ng/ml etg addome
negativo. Dopo 4 mesi alfafetoproteina negativa
1600
1400 2018 (febbraio) alfafetoproteina 213.87ng/ml---
1200 richiesto e programmato controllo ecografico c/o
1000 specialista dedicato: conferma assenza di lesioni
800 focali epatiche
600
400
2018 (maggio) alfafetoproteina 432,09 ng/ml---etg
200
addome negativo
0
2003
2004
2006
2008
2010
2012
2014
2016
2018
2018
2018 (novembre) alfafetoproteina 1497 ng/ml---etg
addome negativo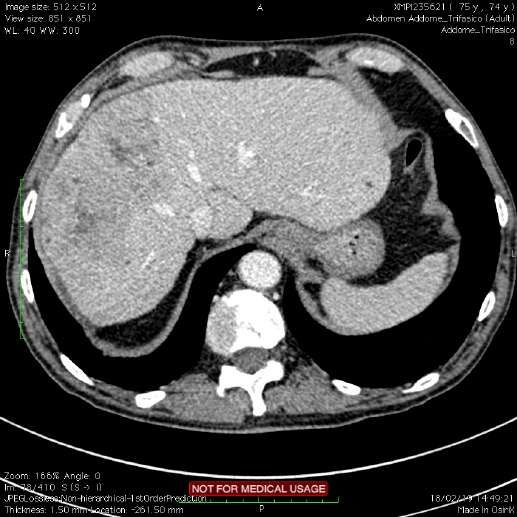
ECOGRAFIA DEI TESTICOLI Il didimo di destra e sinistra presentano dimensioni nei limiti inferiori rispetto alla norma (mm 36.7 X 20.5 x 24.9 e mm. 37.3 x 18 x 26.8 nei diametri longitudinale antero- posteriore e trasverso) ed aspetto ecostrutturale; nel contesto non si rilevano definite lesioni a focolaio. A carico dell'epididimo di destra si rileva una cisti di mm. 2.2 di diametro; a carico dell'epididimo di sinistra si rileva altra cisti di mm. 5.4 di diametro. Modesto idrocele destro e sinistro con scrotoliti. Utile consulenza urologica.
A Dicembre 2018 V
T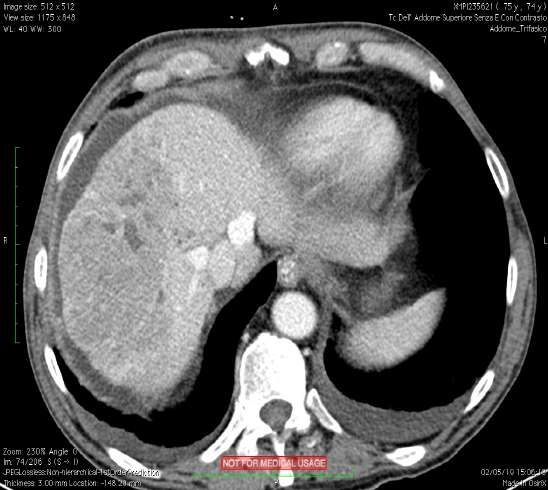
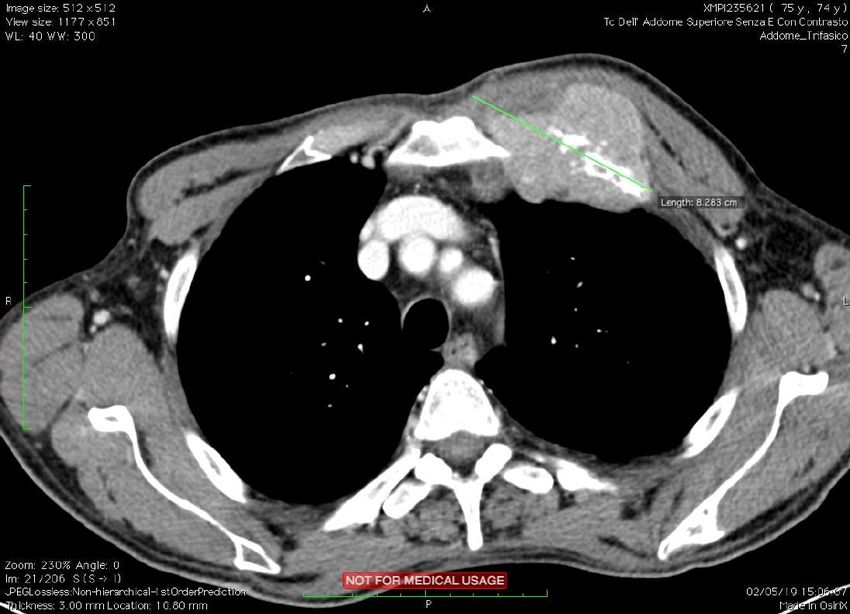
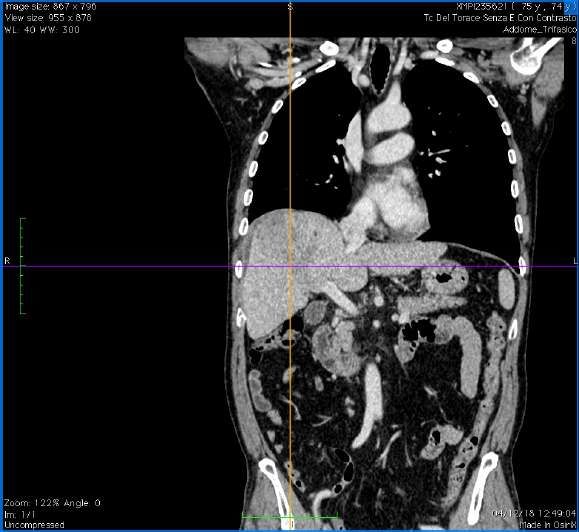
TC DEL TORACE, SENZA E CON CONTRASTO L'esame dimostra una formazione espansiva a carico della parete toracica anteriore a sinistra di circa 39 mm di diametro che interessa l'arco anteriore della II costa in prossimità della articolazione con lo sterno determinando erosione parziale dell'estremo costale con reazione sclerosante. Il reperto è da riferire a localizzazione secondaria costale con invasione del tessuti molli adiacenti. Non sono presenti tumefazioni linfonodali significative delle catene mediastiniche. Non versamenti pleurici. Non si riconoscono lesioni polmonari di significato ripetitivo. Esiti cicatriziali in sede apicale bilateralmente. TC ADDOME COMPL. CON E SENZA CONTR. Si riconosce una estesa neoformazione che occupa gran parte del segmenti epatici 8 e 5 di circa 11 x 7 x 7,5 cm rispettivamente nel diametri sagittale; trasverso e cranio-caudale, disomogenea in tutte le fasi dopo mezzo di contrasto con tendenza alla Ipodensità nelle fasi tardive, compatibile con eteroplasia primitiva. Il fegato appare dismorfico con iperplasia del segmenti del lobo sinistro come si osserva nelle epatopatie croniche. Non dilatazione delle vie billari. Calcolosi multipla mista della colecisti. Pervio l'asse spleno-portale. Piccole cisti displasiche renale a sinistra. Non lesioni focali della milza, pancreas, surreni e rene destro. Non tumefazloni linfonodall significative delle catene addominali esplorate. Non lesioni espansive in sede pelvica né versamenti endoaddominali. Non lesioni ripetitive a carico del metameri dorso-lombari né del cingolo pelvico.
MODIFIED BCLC STAGING SYSTEM AND
TREATMENT STRATEGY
HCC in cirrhotic liver
Very early stage (0) Early stage (A) Intermediate stage (B) Advanced stage (C) Terminal stage (D)
Single 2.5 years ≥10 months 3 months
*Child–Pugh A without ascites. Applies to all treatment options apart from LT; †PS 1; tumour-induced modification of performance capacity;
‡Multiparametric evaluation: compensated Child–Pugh class A liver function with MELD scoreREGIONE AUTONOMA DELLA SARDEGNA
AZIENDA OSPEDALIERO UNIVERSITARIA DI SASSARI
UNITA’ INTEGRATA DI EPATOLOGIA
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
!
UNIEP
!
!
Nome: Lorenzo Nicolò
Cognome: Fiori
Data di Nascita 7/8/1944
Età del paziente: 74
CPT: A 5
Eziologia: HBV
Terapia per epatopatia no virale: Nessuna
Terapia per epatopatia virale: Baraclude
Grado di epatopatia: grado 2 stadio 3
Presenza di ipertensione portale: No
Numero lesioni focali: una lesione epatica + LESIONE espansiva a carico della parete toracica anteriore
sinistra delle dimensioni di 39mm che interessa l’ arcoanteriore della seconda costa in prossimità dell’
articolazioen con lo sterno con invasione dei tessuti molli adiacenti
Sede lesioni: seg 8-5
Dimensioni: 11x7x7.5cm
Tecniche diagnostiche effettuate: TC con MDC
Stadio BCLC: C
DECISIONE TERAPEUTICA MULTIDISCIPLINARE:
Sorafenib 800mg/die
www.aousassari.it!!!!!!!UNIEP!:!viale!San!Pietro,!Padiglione!Malattie!Infettive,!piano!terra!–!07100!Sassari!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!Tel:!!!!!!!!!!!!!!!!!!!!!!!mail:!!!uniep@aousassari.it! ! !!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
!Ø 7/1/18 Comparsa di rush cutaneo esteso
Riduzione del Nexavar a 400mg/diePeggioramento del grado di ipertensione arteriosa
Classificazione Molto comune Comune Non comune Raro Non Nota
per sistemi e
organi
Emorragia Aneurismi e
(incluse dissezioni
emorragie arteriose
Patologie gastrointestina Crisi
Vampate
vascolari li*, delle vie ipertensiva*
respiratorie* e
cerebrali*)
Ipertensione
Patologie Rinorrea Eventi simil
respiratorie, Disfonia malattie
toraciche e interstiziali
mediastiniche del polmone*
(polmonite,
polmonite da
Aggiunto all’ ibersartan la lercanidipina
raggi,
sofferenza
respiratoria
acuta, etc)
Patologie Diarrea Stomatite Pancreatite
gastrointestinali Nausea (incluse bocca Gastrite
Vomito secca e Perforazioni
Costipazione glossodinia) gastrointesti-
Dispepsia nali*
Disfagia
Reflusso
gastro
esofageo
Patologie Aumento Epatite daFebbraio 2019: Ricovero c/o O.C di Alghero per anemia secondaria ad ulcera gastrica
prepilorica Forrest 3
SOSPENSIONE NEXAVARFebbraio 2019 TC ADDOME SUP con MDC: confrontata con esame del 04/12/2018 non mostra sostanziali modifiche volumetriche e morfologiche nelle varie fasi vascolari, della nota lesione espansiva a carico dei segmenti epatici 8 e 5 del fegato. Sostanzialmente nella norma la milza e pancreas ed i surreni. Cisti displasiche renali a sinistra; nella norma il rene di destra. Il fegato appare dismorfico con iperplasia dei segmenti del lobo sinistro come si osserva nelle epatopatie croniche. Non dilatazioni delle vie biliari: Calcolosi multipla della colecisti. Mal valutabile l’asse vascolare venoso dei i segmenti inferiore del fegato.. Non tumefazioni linfonodali patologiche. Prostata aumentata di volume. Diverticolosi multipla del sigma.
A Febbraio 2019 V
TFebbraio 2019
9/3/19 Conclusioni diagnostiche : ERNIA IALTALE. POLIPI GASTRICI IN ATTESA DI TIPIZZAZIONE ISTOLOGICA. PRESENZA DI CLIP ADESA A UNA ULCERA ANTRALE. PRESENZA DI SECONDA ULCERA (Forrest III).
Ø 19 Marzo 2019 Il paziente viene rivalutato in ambulatorio per la comparsa di intenso dolore agli arti inferiori in assenza di chiare tumefazioni ma impotenza funzionale Ø Targin 5/2.5 1cpx2 Ø Richiesta gastroscopia di controllo Ø Richiesta scintigrafia ossea Ø Valutazione ortopedica Ø TC addome e torace
Maggio 2019
Maggio 2019
Maggio 2019
• Gastroscopia negativa
• Introduzione in terapia di Lyrica, Laroxyl, Alghedon e Abstral
Localizzazione di malattia anca di sinistra
• Diversi ricoveri in Medicina con exitus nell’ agosto 2019Titolo asse
10
12
14
16
0
2
4
6
8
2003
2004
2004
2005
242473
2006
2007
IRC
2008
Entecavir
2009
2010
2011
2012
250
2013
HBV DNAHBV DNA
12
Ø HBV DNA apparentemente soppresso fino al
2012 (HBVThe AASLD suggests that persons with persistent low-level viremia (1 log compared to nadir or an HBV-DNA level of 100 IU/mL or higher in persons on NA therapy with a previously undetectable level (
Review
Risk of hepatocellular carcinoma in chronic hepatitis B:
Assessment and modification with current antiviral therapy
George V. Papatheodoridis1,⇑, Henry Lik-Yuen Chan2, Bettina E. Hansen3, Harry L.A. Janssen3,4,
Pietro Lampertico5
1
Academic Department of Gastroenterology, Athens University Medical School, Laiko General Hospital, Athens, Greece; 2Department of Medicine
and Therapeutics and Institute of Digestive Disease, The Chinese University of Hong Kong, Hong Kong Special Administrative Region;
3
Department of Gastroenterology & Hepatology, Erasmus MC University Hospital, Rotterdam, The Netherlands; 4Francis Family Liver Clinic,
Toronto Western & General Hospital, Division of Gastroenterology, University of Toronto, Toronto, Canada; 51st Division of Gastroenterology,
Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, Milan, Italy
Summary NAs, HCC risk can be reduced but not eliminated, probably due
to risk factors that are not amenable to change by antiviral ther-
In the treatment of chronic hepatitis B (CHB), the ultimate goal is apy, or events that may have taken place before treatment ini-
preventing hepatitis B virus (HBV)-associated liver disease, tiation. Validated pre- and on-therapy HCC risk calculators that
including hepatocellular carcinoma (HCC). Recently published inform the best practice for HCC surveillance and facilitate
studies show that in CHB patients treated with the currently rec- patient counseling would be of great practical value.
ommended first-line nucleos(t)ide analogs (NAs) entecavir or ! 2015 European Association for the Study of the Liver. Published
tenofovir, annual HCC incidences range from 0.01% to 1.4% in by Elsevier B.V. Open access under CC BY-NC-ND license.
non-cirrhotic patients, and from 0.9% to 5.4% in those with cirrho-
sis. In Asian studies including matched untreated controls, cur-
rent NA therapy consistently resulted in a significantly lower Introduction
HCC incidence in patients with cirrhosis, amounting to an overall
HCC risk reduction of !30%; in non-cirrhotic patients, HCC risk Despite the dramatic improvement in the management of chron-
reduction was overall !80%, but this was only observed in some ic hepatitis B (CHB), hepatocellular carcinoma (HCC) remains a
studies. For patients of Caucasian origin, no appropriate com- major cause of morbidity and mortality, accounting for around
parative studies are available to date to evaluate the impact of 350,000 deaths worldwide every year [1,2]. Natural history stud-
NA treatment on HCC. Achievement of a virologic response under ies in untreated patients have reported annual HCC incidences of
current NA therapy was associated with a lower HCC risk in 0.3–0.6% in non-cirrhotic patients, and 2.2–3.7% in compensated
Asian, but not Caucasian studies. Studies comparing entecavir cirrhotic patients, with the highest rates observed in Asia [2].
or tenofovir with older NAs generally found no difference in The mechanism of hepatitis B virus (HBV)-related hepatocar-
HCC risk reduction between agents, except for one study which cinogenesis is thought to involve several factors [3–5]. HBV DNA
used no rescue therapy in patients developing lamivudine resis- sequences integrate into the host genome, which may down-
tance. Overall, these data indicate that with the current, potent regulate tumor suppressor genes. Recent studies have shown that
integrated HBV is more frequent in HCCs than in adjacent liverHCC pazienti trattati vs pazienti non trattati
Review
Table 1. HCC outcomes in treated vs. untreated patients.
Study Treatment N Follow-up, yr, HCC incidence, %* HCC with vs. without NA treatment
median (range)
3-yr 5-yr 7-yr All pts Cirrhosis No cirrhosis
Hosaka [26] ETV Total: 316 3.3 (2.3–4.3) 1.2 3.7 n.r. 5-year incidence 5-year incidence 5-year incidence
(Japan) No cirrhosis: 237 0 2.5 3.7% vs. 13.7% 7.0% vs. 38.9% 2.5% vs. 3.6%
NA-naive Cirrhosis: 79 4.3 7 pHCC in pazienti trattati con risposta virologica vs non responders
960
Review
Table 2. HCC outcomes in treated patients with vs. without virologic response.
Study Treatment N Follow-up, VR* HCC incidence, %† HCC with vs. without NA treatment
yr, median
(range)
3-yr 5-yr 7-yr All pts Cirrhosis No cirrhosis
Wong [25] ETV Total: 1446 3.0‡ + VR: 77% 8.7 n.r. n.r. 3-year incidence 3-year incidence n.r.
(Hong Kong) No cirrhosis: 984 8.7% vs. 10.7% p = 0.02
Tx-naive + Cirrhosis: 482 – VR: n.r. 10.7 n.r. n.r. p = 0.33
-experienced
Yang [33] ETV Total: 323 3.0 (1.0–6.0) + VR: 83-98% n.r. n.r. n.r. n.r. HR = 0.08 HR = 0.21
(Taiwan) No cirrhosis: 202 – VR: n.r. n.r. n.r. n.r. p = 0.001 p = 0.001
Tx-naive + Comp cirrhosis: 106
Journal of Hepatology 2015 vol. 62 j 956–967
-experienced Decomp cirr: 15
Kim [34] ETV Cirrhosis: 324 3.0‡ + VR: n.r. n.r. n.r. n.r. n.r. RR = 0.056 n.r.
(Korea) Comp cirrhosis: 220 – VR: n.r. n.r. n.r. n.r. pJOURNAL OF HEPATOLOGY
Table 3. HCC outcomes with current NAs vs. older NAs.
Study Treatment N Follow-up, yr; HCC incidence, %* HCC with current vs. older NAs
median (range) 3-yr 5-yr 7-yr All pts Cirrhosis No
cirrhosis
Hosaka [26] ETV Total: 316 3.3 (2.3–4.3) 1.2 3.7 n.r. 5-year 5-year 5-year
(Japan) (rescue No cirrhosis: 237 0 2.5 incidence incidence incidence
Tx-naive therapy: none) Cirrhosis: 79 4.3 7.0 7.0% vs. 7.0% vs. 2.5% vs.
Historical, PS- LVD Total: 182 6.8 (5.0–9.9) n.r. n.r. n.r. 22.2% 22.2% 4.9%
matched control (rescue No cirrhosis: 97 3.2 4.9 p = 0.043 p = 0.043 p = 0.126
therapy: none) Cirrhosis: 85 12.2 22.2
Kobashi [39] ETV Total: 129 2.9 (0.4–7.5) 7.0 11.8 n.r. 5-year n.r. n.r.
(Japan) (rescue No cirrhosis: 101 incidence
Tx-naïve therapy:Review
ETV TDF ETV or TDF
A No cirrhosis Asian Caucasian*
Prior
Tx-naive and/or exposure Tx-naive and/or
Tx-naive tx-experienced n.r. Tx-naive tx-experienced
2.0 2.0
Annual HCC incidence (%)
1.5 1.4 1.5
1.0 1.0
0.9
1.0 1.0
0.7 0.7
0.7 0.7 0.7
0.5 0.5 0.5
0.5 0.5
0.1
0.0
0.0 0.0
Hosaka Wong Yang Lim Cho Yamada Wong Yang Wu Lampertico Arends Papatheodoridis
[24] [50] [31] [38] [33] [62] [23] [31] [27] [42] [43] [35] [36] [51]
N = 237 N = 813 N = 202 N = 878 N = 933 N = 402 N = 984 N = 314 N = 18,748 N = 213 N = 243 N = 580 N = 212 N = 780
B With cirrhosis Asian Compensated Caucasian*
Prior
Tx-naive and/or exposure Tx-naive and/or
Tx-naive tx-experienced n.r. Tx-naive tx-experienced
6
5.4 5.4 5.2
5.1
Annual HCC incidence (%)
5 4.5
4.1 4.2
3.9
4
3.3 3.3
2.8 2.8
3 2.6 2.5
2.2
2.0
1.8
2 1.5
1.4
0.9
1
0
Lampertico [42]
Lampertico [43]
Papatheodoridis [36]
N = 155
N = 131
N = 69
Arends [35]
N = 164
Papatheodoridis [51]
Koklü [40]
N = 77
N = 353
Koklü [40]
N = 72
Hosaka [24]
N = 79
Wong [50]
N = 247
Yang [31]
N = 121
Chen [44]
N = 239
Lim [38]
N = 860
Cho [33]
N = 445
Su [25]
N = 666
Yamada [62]
N = 94
Wong [23]
N = 482
Kim [32]
N = 324
Chen [44]
N = 143
Yang [31]
N = 152
Wu [27]
N = 2847
Fig. 1. Annual HCC incidence rates with entecavir or tenofovir in CHB without cirrhosis (A) and with cirrhosis (B). Annual HCC incidences were calculated from studies
with different follow-up duration by assuming constant incidence rates over time. In panel B, the following studies reported rates for compensated cirrhotic patients only
(decompensated excluded): Wong [25,53]; Yang, naive/experienced cohort [33]; Lampertico, ETV cohort [44]; Papatheodoridis, ETV/TDF cohort [54]. The following studieson untreated Asian patients, have been developed to predict the
risk of HBV-related HCC based on some of the known HCC risk An important question is whether HCC risk predictors are also
factors (Table 4, [31,47–49]). The REACH-B score was based on applicable in patients receiving antiviral therapy, as this general-
data from the Taiwanese Risk Evaluation of Viral Load Elevation ly results in HBV DNA suppression and sometimes also regression
Table 4. Comparisons of published risk scoring systems for HCC.
CU-HCC GAG-HCC REACH-B PAGE-B
(Wong et al.) [47] (Yuen et al.) [48] (Yang et al.) [31] (Papatheodoridis et al.) [49]
Number of patients 1005 820 3584 1619
Place of development Hong Kong Hong Kong Taiwan Europe
Ethnicity Asian Asian Asian Caucasian
Age (years) 48.0 40.6 45.7 53
HBeAg-negative (%) Not reported 56.6 84.8 84
Cirrhosis (%) 38.1 15.1 0 30
Follow-up (years) 9.94 5.62 12.0 3.3
Antiviral therapy (%) 15.1 0 0 100
HCC (n, %) 105, 10.4 40, 4.9 131, 3.7 56, 3.5
Scoring system Variable Points Variable Points Variable Points Variable Points
Age Age Age Age
>50 years 3 Per year 1 (1*) Per 5 years 1Body mass index1, kg/m2 26.1 (4.4)
Patients with normal ALT, n/N (%) 518/1225
PAGE-B predicts the risk of developing hepatocellular carcinoma
ALT in cases with abnormal ALT, IU/L 82 (85)
in Caucasians with chronic hepatitis B on 5-year antiviral therapy
Platelets , x10 /mm 191 (76)
2 3 3
Patients with HBV DNA 12 mesi
Ø 1851
Medicine, National and Kapodistrian University of Athens, Athens, Greece; 5Department of Gastroenterology, University of Ankara Medical
6
School, Ankara, Turkey; Hospital General Universitario Valle Hebron and Ciberehd, Barcelona, Spain; 4th Department 7
1
Αristotle University of Thessaloniki Medical School, Thessaloniki, Greece; 8Hospital U Puerta de Hierro, IDIPHIM CIBERehd, Madrid, Spain;
of Internal Medicine,
Available in 1055 and 480 patients of the derivation and validation dataset. 2Availabl
9 10 variables: median (IQR) values.
Department
Table 1. Main characteristics of Caucasianofpatients
Gastroenterology & Hepatology,
with chronic hepatitis ErasmusMC,
B (CHB) who Rotterdam,
were treated with entecavir Netherlands; Division of Gastroenterology and Hepatology,
(ETV) or tenofovir (TDF).
Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, Milano, Italy; Liver(Peg-)IFNa, 11
Clinic,pegylated
Toronto interferon-alfa;
Western NA(s),
& nucleos(t)ide analogue(s); HCC, hepatocell
General Hospital, University Health Network, Toronto, ON, Canada
Derivation dataset Validation dataset p value
(N = 1325, 8 centers) (N = 490, 1 center)
Age, years Background & Aims: Risk scores for hepatocellular 52 (21) carcinoma 56in(14)
the validation dataset.CALCOLO
Table 3. Construction of the PAGE-B risk score for predictionPAGE B SCORE
of hepatocellular patients with evaluable PAGE-B score in the deriva
carcinoma in Caucasian chronic hepatitis B(5patients
anni pz in terapia
under entecavir con
or 312 (24.7%), had low (69), 597 (47.2%) intermediate
tenofovir. The score ranges from 0 to 25. entecavir/tenofovir)
355 (28.1%) had high (P18) PAGE-B score. The p
patients AGE with cirrhosis was 3.9% 10 +(12/309), 18.0% (1
Age (years) Gender Platelets (/mm3)
Gender 6+
16-29: 0 Female: 0 ≥200,000: 0 40.9% PLT (144/352)
(191000) 6= score 69, 10–
in cases with PAGE-B
30-39: 2 Male: 6 100,000-199,999: 6 (pSURVEILLANCE IN PATIENTS AT HIGH RISK OF
HCC
• Surveillance is recommended in specific target populations
Recommendations Level of evidence Grade of recommendation
• Cirrhotic patients, Child–Pugh stage A and B Low Strong
• Cirrhotic patients, Child–Pugh stage C awaiting LT Low Strong
• Non-cirrhotic HBV patients at intermediate or high risk of HCC* (according to PAGE-
Low Weak
B† classes for Caucasian subjects, respectively 10-17 and ≥18 score points)
• Non-cirrhotic F3 patients, based on an individual risk assessment Low Weak
• Interval should be dictated by rate of tumour growth and tumour
incidence in target population
• 6-month interval is reasonable and cost-effective
• 3 months: no clinical benefit
• 12 months: fewer early stage diagnoses and shorter survival
*Patients at low HCC risk left untreated for HBV and without regular 6-month surveillance must be reassessed at latest on a yearly basis to verify
progression of HCC risk. †PAGE-B score is based on decade of age (16–29 = 0, 30–39 = 2, 40–49 = 4, 50–59 = 6, 60–69 = 8, ≥70=10), gender (M
= 6, F = 0) and platelet count (≥200,000/µl = 0, 100,000–199,999µl = 1,84.8 84
0 30
REACH-B Score for Hepatocellular Carcinoma
12.0 3.3
0 100
(HCC)
131, 3.7 56, 3.5
Variable Points Variable Points
Age Age
Per 5 years 1 6Research Article JOURNAL
OF HEPATOLOGY
Cancer
Toronto HCC risk index: A validated scoring system to predict
10-year risk of HCC in patients with cirrhosis
Suraj A. Sharma1, Matthew Kowgier1,5, Bettina E. Hansen2, Willem Pieter Brouwer2, Raoel Maan2,
David Wong1, Hemant Shah1, Korosh Khalili3, Colina Yim1, E. Jenny Heathcote1, Harry L.A. Janssen1,2,
JOURNAL
1
Morris Sherman1, Gideon M. Hirschfield4,y, Jordan J. Feld1,⇑,y
OF HEPATOLOG
Toronto Centre for Liver Disease, University Health Network, University of Toronto, Canada; 2Department of Gastroenterology and Hepatology,
Erasmus MC University Medical Centre, Rotterdam, The Netherlands; 3Department of Medical Imaging, University Health Network,
University of Toronto, Canada; 4Centre for Liver Research and NIHR Biomedical Research Unit, University of Birmingham, Birmingham, UK;
Table 3. Components of the Toronto HCC Risk Index.5
Dalla Lana School of Public Health, University of Toronto, Canada Cumulative HCC incidence by THRI risk category
Risk Factor Score 0.4
Age Background & Aims: Current guidelines recommend biannual cirrhosis, and has been validated in an external cohort. This risk
surveillance for hepatocellular carcinoma (HCC) in all patients score may help to guide recommendations regarding HCC
240
Etiologynosed
Methods: A derivation cohort of patients with cirrhosis diag- with cirrhosis, and has been validated in an external cohort. This
Autoimmune
by biopsy or non-invasive measures was identified
through retrospective chart review. 0 The disease-specific inci-
THRI ≤120 0.2incidenza HCC per anno
risk score may help to guide recommendations regarding HCC
surveillance among patients with cirrhosis.
0,3
dence of HCC was calculated according to etiology of cirrhosis. ! 2017 European Association for the Study of the Liver. Published by
HCV SVRFactors associated with HCC were 0 identified through multivari- Elsevier B.V. All rights reserved.
able Cox regression and used to develop a scoring system to pre-
Other dict HCC risk. The scoring system
cohort for validation.
36 was evaluated in an external
Introduction
THRI 120-240 incidenza HCC per anno 1
Steatohepatitis
Results: Of 2,079 patients with 54 cirrhosis and ≥6 months follow- Ambulatory management of cirrhosis is 0.1
of increasing
up, 226 (10.8%) developed HCC. The 10-year cumulative inci- importance with rising rates of chronic liver disease and the
HCV dence of HCC varied by etiologic 97category from 22% in patients associated complications of end-stage cirrhosis. One such
HBV with 97
viral hepatitis, to 16% in those with steatohepatitis and 5%
in those with autoimmune liver disease (p 240
common malignancy among men globally, and seventh most
incidenza HCC per anno
complication, hepatocellular carcinoma (HCC), is the fifth most 3.2%
Gender variable Cox regression, age, sex, etiology and platelets were common malignancy among women, leading to more than 0.0
associated with HCC. Points were assigned in proportion to each 700,000 deaths annually.1–3 In the US, the age-adjusted inci-
Femalehazard ratio to create the Toronto 0 HCC Risk Index (THRI). The 0
dence of HCC rose from 1.6 to 4.5 per 100,000 people between 2
1975 and 2005.4 Currently, one-year survival for HCC is still less
4 6 8 10
10-year cumulative HCC incidence was 3%, 10% and 32% in the
Male low-risk (240) groups respectively, values that remained consistent surveillance and the availability of better therapies.4–6
Plateletsafter internal validation. External validation was performed on Current guidelines recommend twice-yearly ultrasounds for
>200 aviral
cohort of patients with primary biliary cirrhosis, hepatitis B
0 Fig. 2. Cumulative HCC incidence by THRI. The THRI stratified patients
HCC surveillance in all patients with cirrhosis.6,7 These recom-
and hepatitis C viral cirrhosis (n = 1,144), with similar pre- mendations8 result from studies evaluating HCC doubling
low-, intermediate- and high-risk groups. Patients with a THRI score be
time,9,10 cost-effectiveness,11 and one randomized trial of HCC
140–200dictive ability (Harrell’s c statistic20 0.77) in the validation and
derivation cohorts. 120 had an annualized HCC incidence of 0.3% per year. The annual
surveillance in patients with chronic hepatitis B (CHB) infection
80–139 Conclusion: HCC incidence varies 70 markedly by etiology of cir- from China.12 AASLD guidelines state that HCC surveillance is
rhosis. The THRI, using readily available clinical and laboratory incidence in patients with intermediate risk (120–240 points) was
cost-effective at an annualized incidence of 1.5% or above in
240 points) was 3.2%. The curves for
However, the risk of HCC in patients with cirrhosis is known
Total Keywords: Cirrhosis; Hepatocellular0–366
carcinoma; HCC; Toronto hepatoma risk index
to vary with etiology, age, gender and other factors.13–16 Scoring
three risk groups were compared using the log-rank test. HCC, hepatocell
(THRI); Cumulative incidence. systems have been developed for HCC risk prediction in patients
HBV, Hepatitis
Received B25 virus; HCV,
July 2016; Hepatitis
received
available online 24 August 2017
in revisedCform
virus;
8 JulySVR,
2017;sustained virologic
accepted 29 July 2017; response. carcinoma; THRI, Toronto HCC Risk Index.
with specific causes of liver disease, such as CHB. However,
etiology-independent risk stratification is currently not possi-
⇑ Corresponding author. Address: Toronto Center for Liver Disease, Sandra Rotman
Centre for Global Health, University Health Network, University of Toronto, 6B-Fell ble. As a result, HCC surveillance is recommended for all
Pavilion Rm 158, 399 Bathurst Street, Toronto, Ontario M5T 2S8, Canada. patients with cirrhosis, regardless of the etiology of liver disease
E-mail address: Jordan.feld@uhn.ca (J.J. Feld). or the presence of other risk factors.
high-risk group was 3.2% per year, suggesting that th
y
These authors contributed equally to the supervision of this study.
annualized incidence of HCC was lower than the AASLD recom-gies all’inquadramento
utilizing ultrasound and MR replace, the need for liver biopsy and should be seen as
diagnostico e, soprattutto, prognostico.
LINEE GUIDA
uch as Qualità acoustic radiation force a complementary tool in Forza
EPATOCARCINOMA the dellamanagement 2018 of chronic
dell’evidenza Raccomandazione clinica raccomandazione
diffusion-weightedSIGN MRsorveglianza.
imaging HBV-infected patients. clinica
1600 Tutti raccomandati
Pertanto, il monitoraggio semestrale dell’alfa-fetoproteina non può rientrare fra gli strumenti
HEPATOLOGY, April 2018
i pazienti condi cirrosi epatica del e funzione
paziente epatica
s well. These approaches soddisfacente make(classe
dell’ecografia. upTuttavia,
sorveglianza
A e B questo di Child-Pugh)
marcatore dovrebbero
a rischio di HCC, salvo che in assenza di disponibilità
mantiene la sua importanza come indicatore del rischio di sviluppo
B when surveillance
esseredisottoposti abegin.
sorveglianza semestrale delcon ecografia Positivafocale
debole
fibrosis are elas- 1400 HCC should e va (134,135)
dosato al momento Other sub- riscontro di una lesione epatica su cirrosi per contribuire
the liver biopsy by improving
dell’addome
all’inquadramento
fibrosis markers groups with a higher risk of HCC include persons
(13-HDV,
the
superiore per Use
la
diagnostico
18) or HIV coinfections and those with
of
diagnosi
e, risk calculators
precoce
soprattutto, di HCC
prognostico.
these noninva- with HCV,
heyfibrosis also("F2),
reduce
1200 fatty the
evidence di
need
(55,136-139)
to HCC,
recommend
for
liver.L’alfa-fetoproteinaAt liver
this ètime,
Qualità
HCC
dell’evidenza
un indicatore
surveillance
ma, per la ridotta sensibilità nei tumoriin
di rischio di sviluppo
there is insufficient
children di piccole
Raccomandazione clinica
Forza della
raccomandazione
ve with normal except in dimensioni,
U/L men) and 1000
B family
children with
member with
SIGN
non
HCC.
cirrhosis
dovrebbe
sorveglianza per mettere inTutti
Chronic
or with
essere a first-degree
motoi lepazienti
HBV
utilizzata
strategiecon
come infection
test di remains
cirrosi epaticaNegativa
di richiamo e funzione
an important
epatica
debole
cause of
clinica
uld be tested for ! risultati positivi soddisfacente (classeal Asuoe usoB di Child-Pugh) dovrebbero
urement
onths duringusing the TE
Guidance (Fibroscan
ed iStatements
frequenti
peggiorano
HBsAg-Positive Persons
) B for HCCHCC
was development.
che conseguono
Screening
sottoposti
in HCC causes poor qualityPositiva
il rapporto costo/beneficio della sorveglianza semestrale con ecografia
essere a sorveglianza of lifedeboleand
inactive CHB.800 semestrale rispetto alla sola dell’addome ecografia (20)superiore per la diagnosi precoce di HCC
and
BV-DNA is the
levelsmost1. All extensively
HBsAg-positive patients withshortened
evalu- (13-cirrhosis
18) should survival, and is thus regarded as a major health alfafeto
nth intervals. If be screened with US examinationL’alfa-fetoproteina with or without è un indicatore di rischio di sviluppo
alone can be600 AFP every 6 months.
e.ing Following
bove the 4. normal vigorous
Politica validations
di richiamo
2. HBsAg-positive inat highchallenge.
e diagnosi
adults
di HCC, ma, perThe
risk for HCC
dimensioni,
risksensibilità
la ridotta of CHB progressing
nei tumori
non dovrebbe essere utilizzata come test di
di piccole to HCC may be
DNA should be (including Asian or B black men over 40 years per
sorveglianza andmettere in moto le strategie di richiamo Negativa debole
shown
months). to be
La cirrosi è400a reliable
Asian women and accurate
over 50 years of age),
caratterizzata istologicamente da bande reduced persons
eddii frequenti by
tessuto fibroso
with antiviral
risultatichepositivi therapy
che conseguono
delimitano [146], and
al suo uso
noduli di rigenerazione surveillance with
000 IU/mL a first-degree family
but La presenza di piccoli noduli nel fegato member with a
peggiorano history of
epatocitaria. cirroticoilrappresenta
rapporto costo/beneficio
pertanto la norma. dellaTuttavia
sorveglianza
questi
sybutof inliverassessing
disease
noduli, che hanno the
HCC, severity
or personsofwith
•
generalmente
with US examination Il dosaggio liver HDV should
with orematico
dimensioni abdominal
semestrale
comprese
without AFP
be screened
rispetto ultrasonography
alla sola
dell’alfa-fetoproteina
tra 1 e 4
every
mm, non ecografia
vengono (20) and
(AFP)
rilevati serum
non
all’ecografia
è alpha-fetoprotein
un test efficace
not limited
convenzionale 200 in6scala
months.di grigi, che è la tecnica raccomandata nella sorveglianza.
ecent
ty, nonalcoholic
years,
Viene
liver disease.
many
definita3.“lesione
There patients
focale”, inperAsia-
una
are insufficient ladata
lesione sorveglianza
che tests dallo
to emerga
identify can bepertanto
esfondo
high-risk used
ecograficotononscreen devepiù
in modo patients
soppiantare for leearly
distinto (con HCC treat-
l’ecografia
4.
HCC Politica
normali sonde ecografiche
uld be evaluated 0 groups for epatica.
per addome)
Il testdiHowever,
o
in children. ad richiamo
altra
può tecnica
essereit is e
di rea-diagnosi
imaging,
richiesto e che, in genere,
in aggiunta ha dimensioni
tappe.all’ecografia
di
epatica. E’
beenprecancerose
evaluatedcomprendono
almeno 5 mm21
by
. Il
sonableTE,
percorso
to resulting
di
screen
consigliata
la displasia
in
cancerogenesi
HBsAg-positive
una
epatocellulare
ment.
epatica Although,
children
valutazione
ed or
nel
i foci
90%
and dei the
casi global
specialistica
displastici
avviene
(visibili solo al
anumber
in pazienti
Leof
microscopio)
individuals
lesioni
con
ed i aumento
infected
dei
2003
2004
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2016
2018
2018
2018
d HBsAg sero- adolescents Lawithcirrosi è
advanced caratterizzata
fibrosis istologicamente
(F3) cirrho- da bande di tessuto fibroso che delimitano noduli di rigenerazione
noduli displasticisischeand possono essere evidenziati macroscopicamente enel
confegato
tecniche di imaging.
-DNAexperience.
E’ comunqueThe
monitor-
difficile
with
performances
epatocitaria.
those
e allonoduli,
HCC
with
stessoUS
using
a
tempo
che
of
La presenza
first-degree
valori
importante
hanno
examination diwith di
family
CHB
piccoli
member
alfaetoproteina
identificare
generalmente
with or
is
la extensive,
noduli
dimensioni
without ed especially
cirrotico
di unecografia
naturacomprese nodulo
tra 1rilevato
e 4
in
rappresenta
epatica
nel
mm,
endemic
pertanto
non
la
negativa
contesto
vengono
areas
norma.
rilevati
such
Tuttavia
as
questi
all’ecografia
CC surveillance 20
di un fegato cirrotico
AFP every . Esistono
convenzionale
6 months. altri tipi di lesioni
in scala di grigi,maligne
che è lache possono
tecnica insorgere nella
raccomandata su cirrosi, quali il
sorveglianza.
ficant
or a long
fibrosis
cirrhosis, a first-
colangiocarcinoma (CF2 stage)
dura- 4. Fored HBsAg-positive
il linfoma and
Vieneepatico
definitacir-
primitivo,
“lesioneatma
persons Asian-Pacific
tali neoplasie
focale”,
high and sub-Saharan
for complessivamente
una lesione
risk che emerga dallonon African
costituiscono
sfondo ecografico piùinregions, only(cona le
modo più distinto
malesdel and2-3%
>50di tuttiHCC i nuovi normali
whonoduli. Le
are living sonde in ecografiche
metastasi whereper
areas epatiche US daaddome)notAISF
isaltri o ad sono
tumori 24/07/2019
altra tecnica
molto più di imaging,
rare nel epaziente
che, in genere, ha dimensioni di
ood,
n infected with
cirroticoAUROC
withrispetto
Dal punto di vista
ai of 0.81–0.95
soggetti
readily
months
almeno
non
available,
should
istologico,
5 21
cirrotici.
precancerose
le be
and
mm
screening . Il
with
comprendono
small
percorso
AFP
la
number
di
every
displasia
6 of
cancerogenesi patients
epatocellulare
performed. che avvengono durante la cancerogenesi sono accompagnate
trasformazioni
epatica
ed i
develop
nel
foci
90% end-stage
dei
displastici
casi avviene
(visibili
liver
solo al
diseases.
a tappe. Le lesioni
microscopio) ed i
noduli displastici che possono essere evidenziati macroscopicamente e con tecniche di imaging.
Mostincomponente
studies
genere dallareport 22 estimated
progressiva formazione
E’ comunquecutoff difficile Therefore,
di vasi arteriosi
e allo
anomalithe
stesso tempo identification
(neoangiogenesi
portale . Questo sbilanciamento fra le componenti del supporto vascolare fornisce all’HCCimportante
tumorale)
identificare and la
e triage ofunnodulo
perdita della
natura di un patients who
rilevato are
nel contestoHBV infection in the long term [26,27].
To date, there are 2 classes of agents for treatment of and BCP mutations in HBeAg positive patients were correlated
chronic hepatitis B: interferon (IFN)-α and nucleoside or with reduced response rates to IFN [33].
nucleotide analogues (NA). Some data suggest that lower HBsAg levels at baseline are
4000 associated with a better treatment response [34]. However,
HBsAg levels at baseline depend on the phase of HBV infec- Ø HBsAg quantitativo correla
tion and the genotype [11]. For example, HBeAg positive
3500
IFN-α treatment
patients, who were non-responders to IFN therapy, showed in modo significativo con la
notable differences in their HBsAg kinetics across the different
The aim of treatment with IFN is to achieve finite immu-
capacità trascrizionale del
3000
nologic control and HBsAg clearance after therapy. Hence, IFN genotypes A to D [35]. This supports the above mentioned
therapy is a time-restricted therapy, usually given for 48 weeks
[4]. Its purpose is sustained off-treatment response with low
notion that HBsAg levels need to be validated for a distinct
genotype.
cccDNA
2500
virus load and normal ALT without further required treatment.
In comparison with the NA-treatment, pegylated IFN (PEG-
Current data supports the further use of HBsAg as an
on-treatment surrogate marker for sustained treatment re-
IFN) produces rates of immunological response of about 30% sponse in HBeAg positive chronic hepatitis B (Table 2). Early Ø Lo studio REVEAL indica
2000
anti-HBe seroconversion [28] after 6 months of treatment,
whereas the rate of anti-HBe seroconversion is slightly lower
treatment response with HBsAg levelschimèra s. f. [dal lat. chimaera, gr. χίμαιρα, propr. «capra»]. – 1. a. Nella mitologia greca, mostro con testa e corpo di leone, una seconda testa di capra sulla schiena, e una coda di serpente fornita anch’essa di testa, raffigurata spesso nell’arte antica in atto di vomitare fuoco; era considerata come un’incarnazione di forze fisiche distruttrici (vulcani o tempeste). b. In araldica, figura fantastica derivata dal mito greco ma rappresentata con testa di donna, petto e zampe posteriori d’aquila, zampe anteriori di leone e coda di serpente. 2. fig. Idea senza fondamento, sogno vano, fantasticheria strana, utopia: le sue speranze non sono che chimere; l’unità d’Italia sembrava allora una chimera; inseguire chimere. 3. In zoologia, genere (lat. scient. Chimaera) di pesci cartilaginei: hanno corpo squaliforme, testa compressa e bocca piccola; una specie, la ch. mostruosa (lat. scient. Chimaera monstrosa), vive anche nel Mediterraneo a profondità fra 200 e 1200 m. Si conoscono molti generi fossili, dal giurassico al miocene incluso. 4. In biologia generale, individuo le cui cellule derivano da due diverse uova fecondate unite accidentalmente o sperimentalmente. Spesso i gemelli dizigotici nei mammiferi mostrano di essere chimere per i gruppi sanguigni (scambio di cellule staminali durante la vita fetale). 5. In botanica, l’individuo che risulta costituito da caratteri specifici diversi, derivanti dalla saldatura delle due parti concrescenti nell’innesto. Se al punto di contatto dei tessuti dei due individui innestati si originano rami nei quali, per es., il dermatogeno proviene da cellule di una specie, mentre i tessuti interni da cellule dell’altra specie, si hanno chimere periclinali; quando invece la parte destra di un ramo o di una foglia è identica al ramo o alle foglie di una specie, mentre la parte sinistra ha i caratteri di un’altra specie, oppure vi sono settori alterni fra loro con caratteri delle due specie, allora si hanno chimere settoriali.
2003 2004 2008 2019 Lamivudina Lamivudina+adefovir Entecavir
Puoi anche leggere