I trattamenti non farmacologici nella prevenzione secondaria dell'infarto
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
13/07/2015
I trattamenti non farmacologici nella
prevenzione secondaria dell’infarto
Pier Luigi Temporelli
Divisione di Cardiologia Riabilitativa
Fondazione Salvatore Maugeri, IRCCS, Veruno
Il valore aggiunto di una adeguata
prevenzione secondaria
Difficile non è sapere una cosa,
ma sapere far uso di ciò che si sa.
Han Fei, Han Fei Tzu, III sec. a.c.
1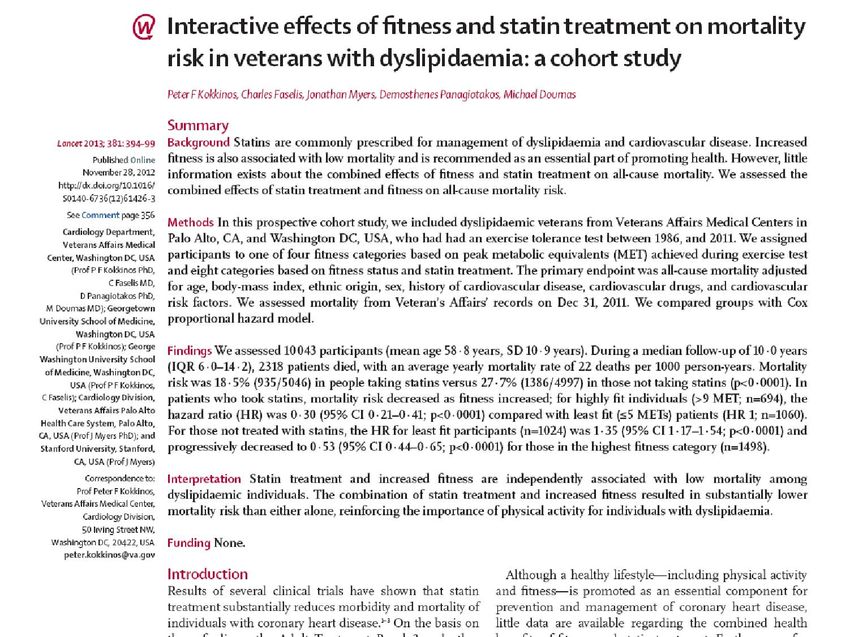
13/07/2015
…“Fumo, ipertensione, diabete, obesità, ridotto consumo di
frutta e vegetali, e mancanza di attività fisica regolare sono
responsabili della maggior parte degli infarti nel mondo intero,
per entrambi i sessi e per tutte le aree abitate”
…“Questi dati suggeriscono che l’approccio alla prevenzione nel
mondo si basa sugli stessi principi ed uno stile di vita corretto è
ovunque in grado di prevenire la maggior parte di casi di infarto
miocardico”
“Our findings suggest that targeted interventions that
reduce blood pressure and smoking, and promote
physical activity and a healthy diet, could substantially
reduce the burden of stroke”
2
13/07/2015
Potential cumulative impact of four
simple secondary-prevention treatments
Yusuf S. Lancet 2002
Risk Reduction 2-year event rate
• ASA 20-30% 6.0%
• Beta Blockers 20-35% 4.5%
• ACE inhibitors 22-25% 3.0%
• Statins 25-42% 2.3%
If all four drugs are used cumulative RRR
is about 75% !!
Impatto cumulativo potenziale dei
farmaci in prevenzione secondaria
Adattata da Yusuf S. Lancet 2002
Riduzione del rischio Eventi a 2 anni
• Nessuno ---- 8%
• Aspirina 20-30% 6.0%
• Beta Bloccanti 20-35% 4.5%
• ACE-inibitori 22-25% 3.0%
• Statine 25-42% 2.3%
• n-3 PUFA 20% 1.8%
If all five drugs are used cumulative RRR
is about 85% !!
3
13/07/2015
Osservatorio ARNO cardiovascolare
4
13/07/2015
Terapia dopo SCA nel mondo reale
Primo semestre
Circulation. November 29,2011
1. Abolizione del fumo
2. Controllo della dislipidemia
3. Controllo dei valori pressori
4. Regolare attività fisica
5. Controllo del peso corporeo
6. Gestione del Diabete Mellito
7. Terapia anti-aggregante
8. Terapia con ACE-inibitori/Sartani
9. Terapia beta-bloccante
10. Vaccinazione anti-influenzale
11. Cardiologia Riabilitativa
5
13/07/2015
Key points
Lifestyle changes are vital in the management of stable
angina, including smoking cessation, healthy diet, weight
loss and control of lipid levels
Associated conditions, such as hypertension and diabetes,
should be treated according to relevant guidance
Anti-anginal drugs should be titrated to the optimal licensed
dose to control symptoms
Revascularisation should be considered in selected patients
6
13/07/2015
Percentage of the Decrease in Deaths from CHD
Attributed to Treatments and Risk-Factor Changes
The Centers for Disease Control
Ford ES et al. N Engl J Med 2007; 356:2388
The use of revascularization
for chronic angina resulted in
a reduction of approximately
15,690 deaths in 2000, as
compared with deaths in
1980, or approximately
5% of the total and only
1.3% was attributable to PCI.
7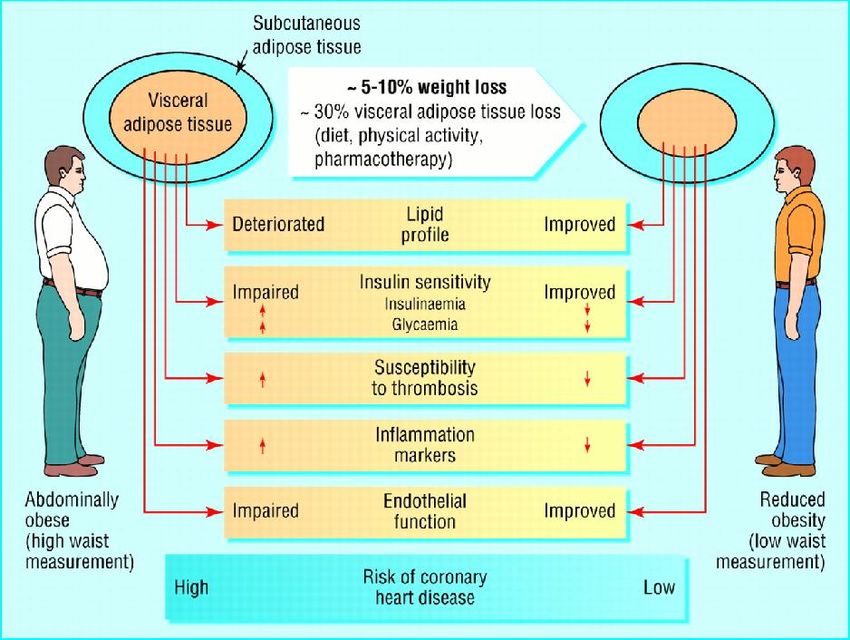
13/07/2015
Circulation. November 29,2011
1. Abolizione del fumo
2. Controllo della dislipidemia
3. Controllo dei valori pressori
4. Regolare attività fisica
5. Controllo del peso corporeo
6. Gestione del Diabete Mellito
7. Terapia anti-aggregante
8. Terapia con ACE-inibitori/Sartani
9. Terapia beta-bloccante
10. Vaccinazione anti-influenzale
11. Cardiologia Riabilitativa
Smoking and high blood pressure top
risk factors for US preventable deaths
PLoS Medicine 2009; 6:1-23
The study of 12 modifiable risk factors showed
smoking was responsible for nearly 1/5 US adult
deaths, while high blood pressure accounted for 1/6
Of 2,448,017 US deaths in 2005
467,000 deaths were associated with tobacco smoking
395,000 with high blood pressure
8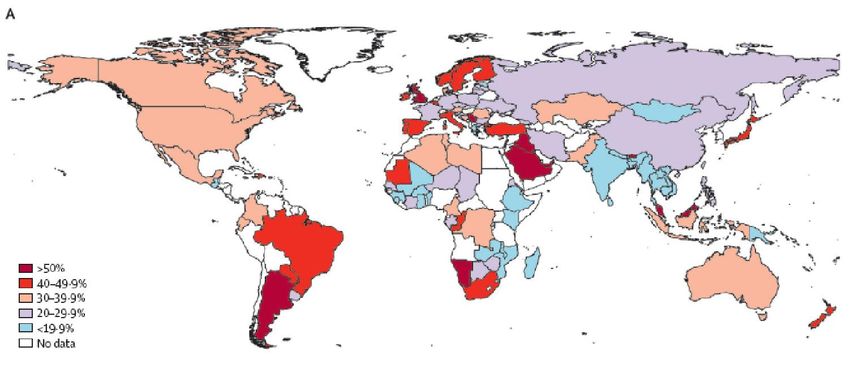
13/07/2015
Effetti diretti ed indiretti dell’attività di diverse
industrie su morbilità e mortalità prematura
nell’uomo
Produttori di
armi da guerra,
droghe pesanti
Produttori di
tabacco
9
13/07/2015
Decreto Sirchia,
gennaio 2003
1013/07/2015
Mortality risk reduction associated with
smoking cessation in pts with coronary
artery disease
Critchley JA et al. JAMA. 2003;290:86-97
Study RR (95% Cl)
Aberg, et al. 1983 0.67 (0.53-0.84)
Herlitz, et al. 1995 Smoking cessation 0.99 (0.42-2.33)
Johansson, et al. 1985 0.79 (0.46-1.37)
determines a 25% RR
Perkins, et al. 1985 3.87 (0.81-18.37)
Sato, et al. 1992 reduction of MI 0.10 (0.00-1.95)
Sparrow, et al. 1978
recurrence over 2 years 0.76 (0.37-1.58)
Vlietstra, et al. 1986 0.63 (0.51-0.78)
Voors, et al. 1996 0.54 (0.29-1.01)
0.1 1.0 10
Ceased smoking Continued smoking
Conclusions.
Our analysis finds smoking to be an independent predictor of
higher 1-year mortality in patients presenting with NSTE-ACS,
and our angiographic study demonstrates CAD in smokers that is
comparable to that in nonsmokers but evident 1 decade earlier.
1113/07/2015
Effect of Smoking Relapse on Outcome After
Acute Coronary Syndromes
Colivicchi F et al. Am J Cardiol 2011;108:804-8
813 patients out of 1,294 (62.8%) resumed regular smoking
The median interval from discharge to smoking relapse was 19 days (range 9 to 76)
Risk of All-Cause Mortality, Recurrent Myocardial Infarction,
and HF Hospitalization Associated With Smoking Status
Following MI With LV Dysfunction
SAVE Investigators, Am J Cardiol 2010; 106:911-16
1213/07/2015
Risk of All-Cause Mortality, Recurrent Myocardial Infarction,
and HF Hospitalization Associated With Smoking Status
Following MI With LV Dysfunction
SAVE Investigators, Am J Cardiol 2010; 106:911-16
Duration of Smoking Cessation After Myocardial Infarction
6 Months 12 Months 24 Months
(adjusted)
Death 0.57 (0.36–0.91) 0.58 (0.33–0.99) 0.53 (0.25–1.08)
Death or recurrent MI 0.68 (0.47–0.99) 0.63 (0.40–0.98) 0.51 (0.28–0.92)
Death or HF 0.65 (0.46–0.92) 0.68 (0.47–0.99) 0.61 (0.39–0.96)
…The approximately 40% lower risk of all-cause mortality associated with
smoking cessation compares favorably to other established therapies for
patients with LV dysfunction after MI, including ACE inhibitors (19%
relative risk decrease), Beta blockers (23% relative risk decrease), and
aldosterone antagonists (15% relative risk decrease).
1313/07/2015
Association Between Smoke-Free Legislation and
Hospitalizations for CV and Respiratory Diseases
A Meta-Analysis
Tan CE and Glantz SA. Circulation, October 30, 2012
Acute Respiratory and Cardiovascular Admissions after
a Public Smoking Ban in Geneva, Switzerland
Humair J-P et al. PLOS ONE, March 2014
1413/07/2015
Circulation. November 29,2011
1. Abolizione del fumo
2. Controllo della dislipidemia
3. Controllo dei valori pressori
4. Regolare attività fisica
5. Controllo del peso corporeo
6. Gestione del Diabete Mellito
7. Terapia anti-aggregante
8. Terapia con ACE-inibitori/Sartani
9. Terapia beta-bloccante
10. Vaccinazione anti-influenzale
11. Cardiologia Riabilitativa
1513/07/2015
Physical inactivity in adults worldwide
Hallal PC et al. Lancet 2012;380:247-57
Age Adjusted Mortality Rates in Subjects
with CAD categorised by level of fitness
Myers J et al. N Engl J Med. 2002;346:793-801
5
LEAST FIT
4,5
(3.3-5.2)
4
3,5
(2.4-3.7)
3
1.0 - 4.9
MET
2,5 (1.7-2.8)
2
5.0 – 6.4
(1.4-2.2)
MET
6.5 – 8.2
1,5
MET
MOST FIT
8.3 – 10.6
1
MET
10.7
MET
0,5
0
1 2 3 4 5
1613/07/2015
Survival analysis of mortality by change in
level of Physical Activity in Myocardial
Infarction patients
Steffen-Batey, Circulation 2000
1.0
Survival probability
increased
active
decreased
0.5
sedentary
2 =46 p65 yrs; follow
up 5 yrs) after MI
Wannamethee S. Circulation 2000
Age-adjusted mortality/1000
60
All-cause
mortality
40
20 Cardiovascular
mortality
inactive light moderate vigorous
Physical Activity
1713/07/2015
Relative mortality risk
by fitness category
Interpretation
Both statin treatment and increased fitness lower all-cause mortality significantly
and independently of other clinical characteristics in dyslipidaemic individuals.
Additionally, the combination of statin treatment and fitness lowers mortality
more than do either alone.
1813/07/2015
• Reduction of resting and exercise heart rate
• Reduction of resting and exercise blood pressure
• Reduction of myocardial oxygen demand at submaximal
levels of physical activity
• Increase in myocardial contractility
• Favorable changes in fibrinolytic system
• Increased endothelium-dependent vasodilation
• Enhanced parasympathetic tone
• Increases in coronary blood flow, collateral vessels, and
myocardial capillary density
Persone di 3 anni e più che praticano sport, qualche attività
fisica e persone non praticanti per sesso - Anni 2001-2009
(per 100 persone di 3 anni e più dello stesso sesso)
Anno Praticano sport Praticano solo Non praticano sport
saltuario continuativo qualche attività fisica né attività fisica
2001 23,1 13,2 28,8 34,2
2002 23,9 12,4 27,9 35,1
2003 25,1 12,3 26,9 35,1
2005 25,2 12,9 26,4 34,7
2006 24,4 12,7
MASCHI 26,1 36,0
2007 24,8 11,9 28,1 34,5
2008 25,8 12,0 26,1 35,3
2009 25,8 11,6 25,8 36,1
2001 15,3 8,0 29,9 46,1
2002 15,7 7,6 FEMMINE 29,3 46,9
2003 16,3 7,9 28,1 47,0
2005 16,9 7,9 29,8 44,5
2006 16,8 8,1 28,4 45,9
2007 16,7 7,4 31,0 44,2
2008 17,6 7,5 29,2 44,9
2009 17,5 7,6 29,4 44,8
1913/07/2015
Physical activity
Why?
Research done in USA estimated that inactive
people would gain 1.3-3.7 years from age 50 years
by becoming active
Franco OH et al. Arch Intern Med 2005;165:2355-60
In an East Asian population, life expectancy from
age 30 years in active people was 2.6-4.2 years
greater than that in inactive people
When CP et al. Lancet 2011;378:1244-53
2013/07/2015
Circulation. November 29,2011
1. Abolizione del fumo
2. Controllo della dislipidemia
3. Controllo dei valori pressori
4. Regolare attività fisica
5. Controllo del peso corporeo
6. Gestione del Diabete Mellito
7. Terapia anti-aggregante
8. Terapia con ACE-inibitori/Sartani
9. Terapia beta-bloccante
10. Vaccinazione anti-influenzale
11. Cardiologia Riabilitativa
Globesity
The Next Tobacco Epidemics
36%
Dati OMS 2005
2113/07/2015
Aspettativa di vita a 40 anni:
impatto dell’eccesso di peso corporeo
Peeters et al. Ann Intern Med 2003; 138: 24-32
Aspettativa di vita a 40 anni di età Normali (18,5-24,9 kg/m2)
50
Sovrappeso (25-29,9 kg/m2)
Obesi (30 kg/m2)
3,3 7,1
anni anni
45
3,1 5,8
46.3
anni anni
43.4
43.0
40
40.3
39.2
37.5
35
Donne Non- Uomini Non-
fumatrici fumatori
Benefici di una moderata
perdita di peso (5-10%)
Després JP et al BMJ 2001;322:716-20
2213/07/2015
GISSI-Prevenzione
Intervento dietetico
Eur J of Clinical Nutrition2003;57:604-611
Nel mondo occidentale per ogni dollaro speso per
promuovere alimenti sani, se ne spendono 500
per propagandare junk-food
Alla ricerca del giusto peso. Lucchin L. 2008
40 spot all’ora sul cibo
2313/07/2015
Perché poca attenzione agli
stili di vita dopo SCA?
2413/07/2015
Prevalence of a Healthy Lifestyle Among
Individuals With Cardiovascular Disease
in High-, Middle- and Low-Income Countries
The Prospective Urban Rural Epidemiology (PURE) Study
Yusuf S. JAMA 2013; 309:1613-1621
Prevalence of Adoption of Combination of Healthy Lifestyle Behaviors
by Country, Economic Status, and Region
Come impostare la promozione della
salute a partire dalla fase acuta
La prevenzione secondaria inizia in UTIC
La prevenzione secondaria continua con una
lettera di dimissione orientata alla prevenzione
2513/07/2015
EUROASPIRE II Study Group
Informazioni fornite alla dimissione
Cohen, Lancet 2001; 357
Per il 15% dei fumatori non c’erano informazioni
sulla necessità di smettere di fumare;
Solo nel 31% delle relazioni erano riportate
informazioni relative alla attività fisica;
Il 43% dei malati in sovrappeso non erano stati
informati sulla necessità di ridurre il peso;
Istruzioni sull’alimentazione erano state fornite al
33% degli ipertesi ed al 61% dei dislipidemici
Ideale lettera di dimissione
dalla Cardiologia
Uniformazione contenuti
Linguaggio più semplice (evitare uso
indiscriminato di acronimi e sigle)
Identificazione di un “minimal data set” di
informazioni da fornire irrinunciabile
Indicazioni al MMG sulla titolazione terapia e
sulle raccomandazioni per lo stile di vita
Indicazione per tempi/modalità dei controlli
Riferimenti alla CR del territorio (degenziale o
ambulatoriale) in base alle indicazioni
2613/07/2015
Come impostare la promozione della
salute a partire dalla fase acuta
La prevenzione secondaria inizia in UTIC
passa attraverso una lettera di dimissione
orientata alla prevenzione
continua in ambienti dove è radicata la
cultura della prevenzione e della modifica di
alterati stili di vita
Conclusion: The GOSPEL Study is the first trial
to demonstrate that a multifactorial, continued
reinforced intervention up to 3 years after
rehabilitation following MI is effective in
decreasing the risk of several important CV
outcomes, particularly nonfatal MI
2713/07/2015
Physical activity in CAD
Why poor adherence?
“Role Models” per i pazienti
2813/07/2015
Inpatient smoking-cessation counseling and all-cause
mortality in patients with acute myocardial infarction
Van Spall HGC et al. Am Heart J 2007;154:213-20
Relative risk of 1-year mortality associated with
smoking-cessation counseling
Hazard ratio (95% CI)
Unadjusted Adjusted
Not counseled (n = 1681) 1.00 1.00
Counseled (n = 1830) 0.41 (0.30-0.56) 0.63 (0.44-0.90)
Factors associated with no counseling
included admission under the care of a cardiologist
(OR 0.67, 95% CI 0.52-0.85)
2913/07/2015
“Tutti pensano a cambiare il mondo,
ma nessuno pensa a cambiare se stesso„
Lev Tolstoj
3013/07/2015
Prevalence of diabetes remission by intervention and year
31Puoi anche leggere