L'algoritmo diagnostico terapeutico nelle infezione sessualmente trasmesse - Marco Cusini Fondazione IRCCS Policlinico - ICAR 2019
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

L’algoritmo diagnostico
terapeutico nelle infezione
sessualmente trasmesse
Marco Cusini
Fondazione IRCCS Policlinico
UO Dermatologia – Centro MTS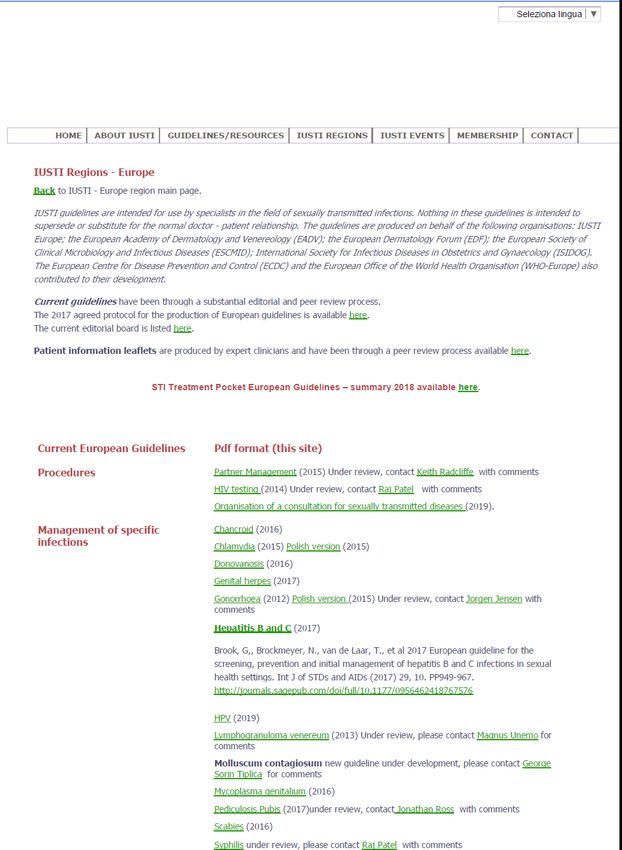
DEFINIZIONE MTS
Malattia sessualmente trasmessa
Infezione che può essere acquisita tramite
contatto sessuale
QUANDO E’ SESSO COMPORTAMENTO MASCHI FEMMINE BACIO 1.4% 2.9% CONT. CON CAPEZ. (fatto) 1.7% 5.3% CONT. CON CAPEZ. (subìto) 2.0% 4.5% CONT. CON GENIT. (fatto) 11.6% 17.1% CONT. CON GENIT (subìto) 12.2% 19.2% CONT. ORO-GEN. (fatto) 37.3% 43.7% CONT. ORO-GEN (subìto) 37.7% 43.9% RAPPORTO PENO-ANALE 82.3% 79.1% RAPPORTO PENO-VAG. 99.7% 99.2% Sanders SA et al. JAMA 1999 would You say You “had sex” if…?
AGENTI SESSUALMENTE TRASMISSIBILI
BATTERI VIRUS
– Neisseria gonorrhoeae – Human immunodeficiency virus
– Chlamydia trachomatis – Herpes simplex virus
– Mycoplasma hominis – Human papillomavirus
– Ureaplasma urealyticum – Virus epatite A, B, C
– Mycoplasma genitalium – Cytomegalovirus
– Treponema pallidum – Virus del mollusco contagioso
– Gardnerella vaginalis – Herpes virus tipo 8
– Mobiluncus curtisii PROTOZOI
– Mobiluncus mulieris – Trichomonas vaginalis
– Haemophilus ducreyi – Entamoeba histolytica
– Calymmatobacterium granulomatis – Giardia lamblia
– Shigella spp FUNGHI
– Campylobacter spp – Candida albicans e spp.
ECTOPARASSITOSI
– Phthirus pubis
– Sarcoptes scabiei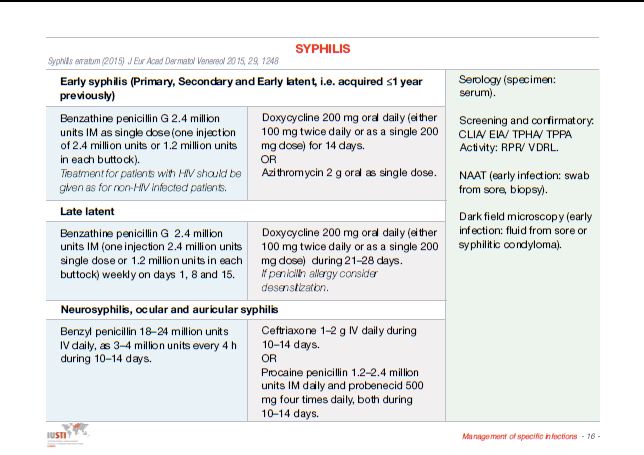
PERCHÉ LE LINEE GUIDA? Per utilizzare algoritmi diagnostico terapeutici basati sull’evidenza medica Per fornire un mezzo educativo a studenti, specializzandi e specialisti Per individuare lacune nelle conoscenze attuali, meritevoli di ulteriori studi Per fornire alle strutture di governo indicazioni di politica socio-sanitaria
LINEE GUIDA E IST Epidemiologia variabile nel tempo e nello spazio Multidisciplinarietà Trattamento on the spot Prevenzione della diffusione Attenzione per i gruppi a rischio Norme comportamentali
TARGET LINEE GUIDA A qualsiasi specialista può capitare di vedere una IST Non esiste in Italia la figura dello specialista di IST I dermatologi hanno storicamente ed accademicamente la competenza maggiore nel campo delle IST Pochi sono i dermatologi con un reale interesse nel campo La gestione di una IST è a volte molto complicata e l’approccio multidisciplinare è obbligatorio Nel nostro paese l’approccio diagnostico terapeutico è spesso molto diverso a seconda della specialità del medico che lo applica
LINEE GUIDA IST Nella stesura è importante considerare l’aspetto socio-epidemiologico Una linea guida non è solo diagnosi e terapia Dovrebbero essere sempre indicati i metodi di screening e di contact tracing Trattamento dati sensibili
IN PRATICA…. Disponibilità dei finanziamenti Tipologia di paziente Tempo disponibile Risorse diagnostiche disponibili
LINEE GUIDA IN ITALIA Linee guida internazionali (CDC IUSTI) Linee guida nazionali (società scientifiche) Linee guida locali (??????)
CDC e IUSTI
PREGI DIFETTI
Emanate da Lingua inglese
organismi prestigiosi Invecchiamento
Basate su algoritmi precoce
rigorosi Poco diffuse
Facile consultazione Non raccomandate
dalle nostre Società
Facile applicabilità
Scientifiche
Complete Non raccomandate dal
SSNSexually Transmitted Diseases
Treatment Guidelines, 2015
MMWR
June 15, 2015
Volume 64
No. RR- 03STD Prevention and Control Education and counseling to reduce risk of STD acquisition Detection of asymptomatic and/or symptomatic persons unlikely to seek evaluation Effective diagnosis and treatment Evaluation, treatment, and counseling of sexual partners Preexposure vaccination--hepatitis A, B, C e non solo
Syphilis
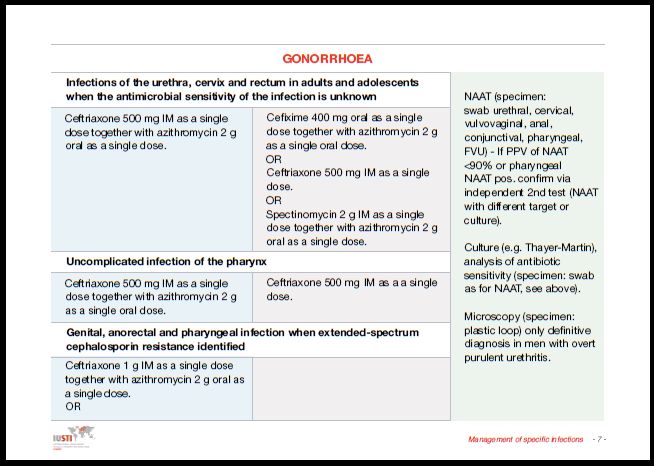
GONORRHOEA
Resistance in gonococci has usually developed first in
the WHO Western Pacific Region (frequently Japan)
followed by international spread.
Many bacterial species share their mechanisms of
resistance through horizontal gene transfer and
subsequent recombination.
Horizontal gene transfer is particularly possible in the
pharynx , which harbours many non-gonococcal
Neisseria spp, and can facilitate the emergence and
spread of antimicrobial resistance particularly in high-
frequency transmitting populations, such as MSM and
commercial sex workers….
Sexually transmitted infections: challenges ahead
Magnus Unemo*, Catriona S Bradshaw*, Jane S Hocking et al. Lancet Infect
Dis 2017 17: e235–79Gonorrohea cont The prevalence of multidrug-resistant (MDR)gonococcal strains substantially increased during the past decade. The first extensively drug-resistant (XDR) gonococcal strains, displaying high-level resistance to ceftriaxone (minimum inhibitory concentration [MIC] of 2–4 mg/L) and retained resistance to previously used therapeutic antimicrobials, have also been isolated in Japan, France, and Spain Many additional ceftriaxone-resistant strains might already be circulating but are undetected because of suboptimal antimicrobial resistance surveillance in many settings
Gonorrohea cont (2) Dual antimicrobial therapy is recommended for treatment where up-to-date, local, and high-quality antimicrobial resistance surveillance data do not support other therapy Solithromycin, gepotidacin, and particularly zoliflodacin can be promising for gonorrhoea treatment and deserve further attention. Ultimately, as for chlamydia, a gonococcal vaccine might be the only sustainable solution for gonorrhoea control.
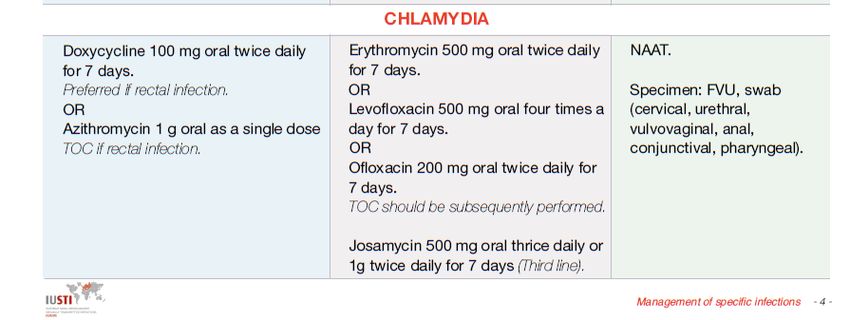
Chlamydia (escluso LGV) Epidemiologia (18 – 26 anni) : prevalenza: 3 -5.3% (♀) 2,4 -7.3 (♂) Contagio diretto attraverso le mucose (rischio di contagio 10% per singolo atto- 55% in relazione stabile di sei mesi) Clearance spontanea circa 50% dopo un anno Infezione asintomatica nel 70-90% ♀ e in 50% ♂ Infezione anale 3- 10% (MSM) 8.4% ♀ con infezione urogenitale Infezione faringea 0,5% - 2,3% (MSM)
Indications for laboratory testing (Level of
evidence IV; Grade C recommendation)
.
Risk factor(s) for C. trachomatis infection and/or other STI (ageChlamydia diagnosis Nucleic acid amplification tests (NAATs), identifying C. trachomatis specific nucleic acid (DNA or RNA) in clinical specimens, are recommended to be used for diagnostics, due to their superior sensitivity, specificity, and speed (incubation 1-3 days) The recommended first choice specimens for diagnosis of urogenital chlamydial infections with NAATs are first- void urine for men (up to 20 ml sampled>1 h after previous micturition) (testing of semen specimens is not recommended) and (health-care worker- or self- collected) vulvo-vaginal swabs for women
Chlamydia diagnosis Annual C. trachomatis testing in STI or sexual health clinics is recommended for all sexually active young women and men (
Mycoplasma genitalium The prevalence of M. genitalium in men with NCNGU ranges from 10% to 35%, thus contributing significantly to the overall burden of disease. In comparison, M. genitalium is detected in only 1% to 3.3% of men and women in the general population In a recent meta-analysis, significant associations were found between M. genitalium and cervicitis [pooled odds ratio (OR) 1.66], and PID (pooled OR 2.14). M. genitalium has been associated with preterm birth (pooled OR 1.89), and spontaneous abortion (pooled OR 1.82) In a recent meta-analysis, persistent M. genitalium was associated with a pooled OR of 26 for persistent urethritis. Thus, failure to eradicate M. genitalium leads to persistent or recurrent disease in the vast majority of men with persistent infection and diagnosis and optimal treatment is extremely important. In sexually transmitted infection (STI) patients, the prevalence is usually from 60% to 85% of that of C. trachomatis, but in the general population, the ratio is generally significantly lower
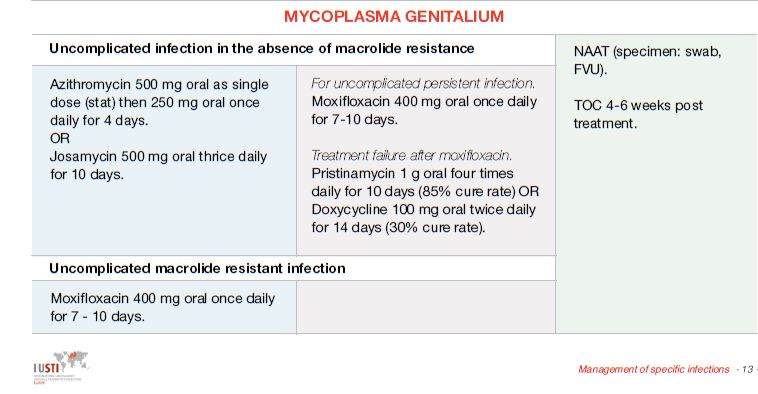
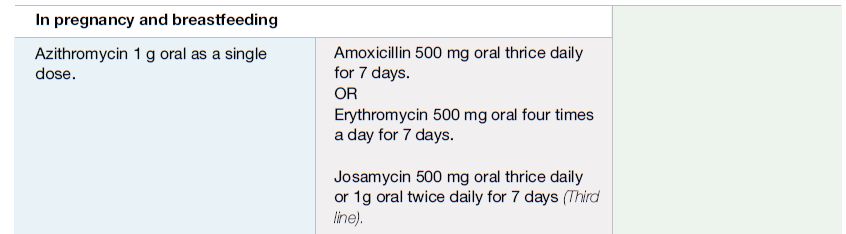
Mycoplasma genitalium
Treatment
Efficacia doxiciclina 30 - 40%
Efficacia Azitromicina 1gr 85% (resistenza 40%)
Efficacia azitromicina EC 95% (resistenza 40%)
Efficacia Josamicina 80% (stesso profilo resistenza)
Efficacia moxifloxacina >95% (resistenza 30%)
Efficacia pristinamicina >95% (resistenza ???)
Le linee guida indicano diversi scheni terapeutici a
seconda dei profili di resistenzaWelcome to IUSTI-Europe Congress 2019 Dear Friends and Colleagues, It is a great pleasure and an honour to extend to you a warm invitation to the 33rd IUSTI- Europe Congress on Sexually Transmitted Infections, to be held September 05 – 07, 2019 in Tallinn, Estonia. The meeting will take place in the historic venue of the Estonian National Opera in the heart of the medieval city. Organizers of the congress are determined to promote a stimulating atmosphere conducive to learning and debate as well as provide opportunities to network with colleagues. To help you make the most of your visit to Tallinn we will also host a number of memorable social events.
Puoi anche leggere