INCONTRO CON LA CARDIOCHIRURGIA PEDIATRICA DI PADOVA: STORIE DA RACCONTARE E DA CONOSCERE - Prof. Giovanni Stellin UOC Cardiochirurgia Pediatrica ...
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

INCONTRO CON LA CARDIOCHIRURGIA PEDIATRICA DI PADOVA:
STORIE DA RACCONTARE E DA CONOSCERE
Introduzione storica: la Cardiochirurgia di Padova
Prof. Giovanni Stellin
UOC Cardiochirurgia Pediatrica e Cardiopatie Congenite
Università degli Studi di Padova
University of Padua - “Il Bo”
“Il Bo” - The Hall of the Forty and the Galileo Galilei’s podium
The tower of the Astronomical Observatory “La Specola”
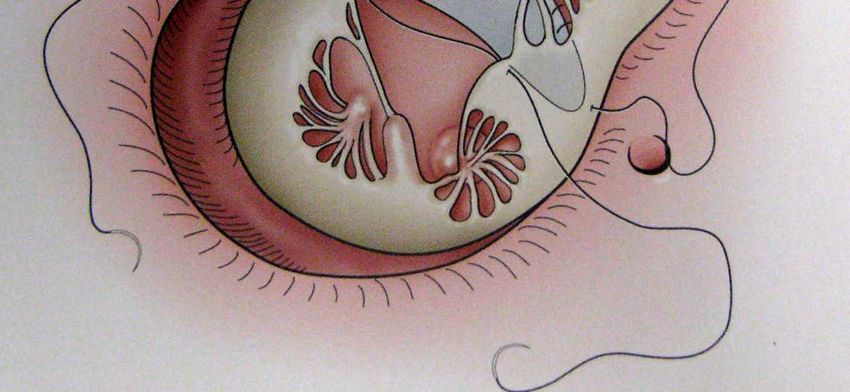
“Il Bo” The Anatomy Theatre of Girolamo Fabrici d’Acquapedente
“Exercitazio Anatomico de Motus
Cordis et Sanguinis in Animalibus”
Portrait of
William Harvey
Carlo A. Carlon MD
The Journal of International College of
Surgeons
July. 1951
Pier Giuseppe Cevese and his pupils

November 14, 1985:
Vincenzo Gallucci performs the first cardiac
transplant in Italy
Aldo R. Castaneda
William I. Norwood
Richard and Stella Van Praagh
Milestones in the History of Cardiac Surgery of Congenital Heart Disease at the University of Padua January 1964 Closure of Interatrial Defect December 1968 Correction of Tetralogy of Fallot November 1985 Heart transplant in Italy September 1988 First Norwood operation in Europe May 1989 First neonatal Htx in Italy
INCONTRO CON LA CARDIOCHIRURGIA PEDIATRICA DI PADOVA:
STORIE DA RACCONTARE E DA CONOSCERE
Presentazione attività UOC Cardiochirurgia Pediatrica e Cardiopatie Congenite
Correzione chirurgica precoce delle cardiopatie congenite (CAVC, TGA, TOF)
Prof. Giovanni Stellin
UOC Cardiochirurgia Pediatrica e Cardiopatie Congenite
Università degli Studi di PadovaIl Centro Cardiopatie Congenite e Pediatriche di Padova è il Centro di Riferimento Regionale per il trattamento di pazienti affetti da cardiopatie congenite
LA NOSTRA ATTIVITA’ correzione chirurgica di TUTTE LE CARDIOPATIE CONGENITE (presenti alla nascita) nel bambino e nell’adulto con prevalenza di interventi in età neonatale o nei primi mesi di vita (correzione precoce).
I NOSTRI RISULTATI circa 300 procedure all’anno Negli ultimi anni il rischio chirurgico è sceso per assestarsi attorno al 3% con risultati paragonabili ai migliori centri in Europa e del Nord America.
ECCELLENZE • Correzione chirurgica precoce delle cardiopatie congenite • Chirurgia Mini-invasiva • Il Cardiopatico congenito adulto (ACHD) • Progetto Europei ARISE ed ESPOIR
La correzione precoce
Vantaggi
• Correzione del vizio anatomico
• Eliminazione del sovraccarico cronico e/o
della cianosi cronica
• Preserva il cuore ed altri organi ed
apparati
• Garantisce il miglior risultato funzionale a
lungo termineMyocardial potential
Mechanism of myocardial cell
hyperplasia, together with
myocites hypertrophy which
is retained for a few weeks
after birth, it is well
recognised .
Prenatal Diagnosis and surgical outcome: a teamworkTeam-work CHDs heterogeneous and often complex Team-work of experts is needed with the aim of : Best medical and surgical planning Best counseling with the parents Prenatal Diagnosis and surgical outcome: a teamwork
Team-work
DIAGNOSIS (or
Pediatric Cardiologist Pediatric Cardiac Surgeon
suspected)
Couseling
Third level center Therapeutic Plan
Prenatal Diagnosis and surgical outcome: a teamworkClinical history
TRASPOSIZIONE DELLE GRANDI ARTERIE±
±DIV
•Circa il 12% delle cardiopatie congenite
diagnosticate alla nascita
•Aorta nasce da VDx e arteria polmonare da
VSx.
•Raramente anomalie extracardiache associate
•Alla nascita, cianosi ingravescente, polipnea,
scompenso cardiacoTRASPOSIZIONE DELLE GRANDI ARTERIE±
±DIV
•Circa il 12% delle cardiopatie congenite
diagnosticate alla nascita
•Aorta nasce da VDx e arteria polmonare da
VSx.
•Raramente anomalie extracardiache associate
•Alla nascita, cianosi ingravescente, polipnea,
scompenso cardiacoTRASPOSIZIONE DELLE GRANDI ARTERIE±
±DIV
•Circolazione sistemica e
polmonare non in serie
ma in parallelo
•Sopravvivenza
assicurata dal “mixing” a
livello atriale,
ventricolare e duttaleDiagnosi
• La DIAGNOSI è spesso prenatale
TGA nascita in elezione presso centri 3 °livello
1) Ipossia e acidosi: entro 24 ore ( chiusura del PDA) infusione PGE1
2) Segni si scompenso cardiaco (epatomegalia, polipnea) se è
presente un VSD
3) Diagnosi ecocardiografica accurata e programmazione correzionePrimi trattamenti
• Infusione di PGE1 per far riaprire il dotto arterioso se è presente cianosi
• Atriosettostomia sec. Rashkind: procedura ecoguidata, si introduce un
catetere con pallone in vena femorale e da qui lo si spinge attravero la vena
cava inferiore in atrio destro. Si fa passare in catetere attraverso il forame
ovale in atrio sinistro. Si gonfia il pallone e si tira con forza per lacerare la
valvola del forame ovale in modo da aumentare il mixing intracardiaco.
• Terapia medica antiscompenso fino all’intervento.Correzione chirurgica Indicazioni all’intervento: CORREZIONE PRIMARIA NELLE PRIME 2 SETTIMANE DI VITA Correzione precoce: il ventricolo sinistro perde la sua ipertrofia contro le basse resistenze polmonari. Non più in grado di sostenere acutamente le resistenze sistemiche post intervento correttivo.
TRASPOSIZIONE DELLE GRANDI ARTERIE±
±DIV
•Utile la diagnosi prenatale
•Alla nascita, PGE1 ed eventualmente
Rashkind
•Intervento chirurgico (Arterial Switch)
deve essere effettuato nelle prime
settimane di vita
•Ottimi risultati chirurgici nel breve e
lungo termineRisultati
•Periodo: 1990-2017
•N=260 pazienti
Associated CHDs in complex D-TGA
VSD* 79 (95%)
•Simple DTGA IVS: 177 LVOTO* 10 (12%)
Aortic Coarctation* 10
•Complex DTGA: 83 (12%)
Other less common CHDs* ǂ 16 (19%)
•Età correzione: 8 giorni (IQR 6-12 giorni)
•Mortalità ospedaliera: 5.8 %
•Simple DTGA: 3.4 %
•Complex DTGA: 11%
•Mortalità tardiva: 2 (0.8%)(complex DTGA)
•Reinterventi tardivi: 6.9%
•Procedure emodinamiche al follow-up: 9.8%University of Padua Medical School Pediatric and Congenital Cardiac Surgery Unit
Tetralogia di Fallot
Viene chiamata anche
Morbo blu o Maladie bleu.
Descritta per la prima volta nel 1888
da Etienne-Louis Arthur Fallot.Fisopatologia
La cianosi è dovuta allo shunt destro-sinistro.
L’entità dello shunt destro-sinistro è determinata dal grado di stenosi del RVOT e
dalle resistenze vascolari sistemiche.
AO
RV LVAnatomy
Surgical history of repair
(University of Padua)
Evolution of our surgical policy
• Since 80’s: “Classic” transventricular
repair in infants
• Since 1991: Early transatrial one-stage
repair (6-3 months of age)
• Since 2007: Further evolution: PV
preservationCorrezione chirurgica
Indicazioni all’intervento:
Timing chirurgico:
a) Pazienti sintomatici (neonati cianotici, crisi ipossiche) correzione
immediata
b) Pazienti asintomatici correzione elettiva nei primi 3 mesi di vitaSurgical repair: timing
The timing for complete repair is still controversial and varies from center to
center.
World-wide trend favors early repair (3-6 months of life), just as for many other
complex CHDs.
Complete early repair has been advocated to avoid:
- Abolish chronic cyanosis and spells
- Systemic-to-pulmonary artery shunts and their consequences
- Chronic RV pressure overload and myocardial compensatory hypertrophy
(which requires a more extensive resection, at the time of the repair)
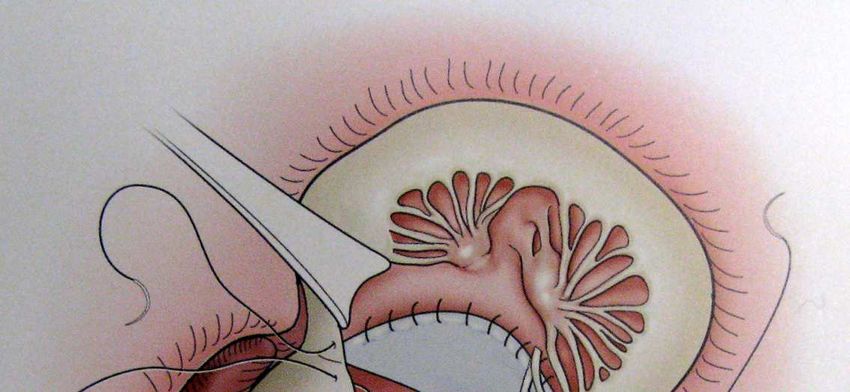
- Hospital costs and offering patients one instead of two operations.Trans-atrial approach Our standard institutional policy for TOF repair in early infancy since June 1991 (usually in patients ≤3 months of life) includes: 1) trans-atrial/trans-pulmonary approach to the pulmonary outflow tract 2) incision of the PV annulus with minimal right ventriculotomy (3-5 mm), when necessary 3)trans-atrial closure of the ventricular septal defect using an autologous pericardial patch
Trans-atrial approach We have demonstrated a trend towards a reduced RV volume and a better ejection fraction in the long term after transatrial repair, when compared to a classic transventricular repair. Minimizing or eliminating a right ventriculotomy may also reduce the substrate for ventricular arrhythmias arising from incisions in the right ventricle. Stellin G, Milanesi O, Rubino M, Michielon G, Bianco R, Moreolo GS, Boneva R, Sorbara C, Casarotto D. Repair of tetralogy of Fallot in the first six months of life: transatrial versus transventricular approach. Ann Thorac Surg. 1995 Dec;60(6 Suppl):S588-91.
Transannular patch
• Despite the awareness of late consequences of
pulmonary valve regurgitation, TAP remains the
most prevalent technique for repairing TOF.
Leading inevitably to chronic PRMonocusp for RVOT reconstruction Monocusp reconstruction of the RVOT by using either pulmonary homografts (less frequently prosthetic material) This can avoid immediate PVR, improving the short-term clinical outcome. Nonetheless, when a cusp needs to be added, leaflets function often deteriorate over time, resulting in a progressive PV regurgitation.
PV preservation techniques
Since 2007
Transatrial / transpulmonary approach
+
PV balloon dilation (trans-atrial)
+/- valve resuspension
Initial indication PV Z-score ≥ -3
Vida VL, Padalino MA, Maschietto N, Biffanti R, Anderson RH, Milanesi O, Stellin G.
The balloon dilation of the pulmonary valve during early repair of Tetralogy of Fallot.
Catheter Cardiovasc Interv. 2012 Nov 15;80(6):915-21.PV preservation techniques
Data at follow-up
• 58 pts (96%) at follow-up
• Median follow-up time of 3.5 yrs (IQR 1.6-5.2 yrs)
• Only 1 late reoperations for RVOT early in our experience
• The median RVOT gradient: 20 mmHg (IQR 15-25 mmHg)
• The degree of PV regurgitation (total at follow-up)
None/mild in 42 pts (75%)
Moderate in 14 pts (25%)Conclusions We believe that the preservation of the PV function during early repair of TOF, by combining different intra-operative surgical maneuvers, can be extended to almost all patients with classic TOF
Conclusions • Our results show that this new surgical technique: • 1) can reduce early and mid-term post-operative pulmonary regurgitation • 2) improving RV function
Conclusions
• By preserving PV function during early TOF repair we
should contribute to ameliorate the long-term follow-up,
possibly decreasing the number of future re-interventions on
the RVOT.
• A longer follow-up and a larger case-series are needed.Anatomical Theatre – Palazzo Bo - Padova Galileo Galilei’s chair– Palazzo Bo - Padova
Difetti del setto
atrioventricolare (Canale A-V)
Forma parziale
Forma completaCanale atrio-ventricolare completo
Canale atrio-ventricolare completo
RX torace
Segni di iperafflusso
polmonareCanale atrio-ventricolare completo
Anomalie associate
Sindrome di Down (70%)
Tetralogia of Fallot
Ventricolo destro a doppia entrata e trasposizioni delle grandi
arterie
Ostruzione del tratto d’efflusso del ventricolo sinistro
DIV multipli
Valvola Mitrale a doppio orifizio
Muscolo papillare singoloCanale atrio-ventricolare completo
Approccio chirurgico
Correzione elettiva entro 2-3 mesi di vita
PA banding in rari casi con controindicazione BPCPT
Diagnosi ecocardiografica esaustivaCanale atrio-ventricolare completo
Correzione chirurgicaRisultati
•Periodo: 1992-2014 (22 anni)
•N=159 pazienti con CAVC
•133 CAVC
•21 CAVC forma transizionale
•Età correzione: 96 giorni (IQR 73-128 giorni)
•Mortalità ospedaliera: 1.9%
•CAVC: 2.3 %
•CAVC forma transizionale: 0%
•Mortalità tardiva: 7.7%
•Reinterventi sulla valvola AV sx: 10%U.O.A. Cardiochirurgia Pediatrica, Università degli Studi di Padova
Transposition of the great arteries: history
Surgical atrial septectomy
1950 The surgery of TGA commenced in 1950 when Alfred
Blalock and Rollins Hanlon described a closed method of atrial
septectomy at the Johns Hopkins Hospital.
First palliative procedure that
permitted survival of children with
TGA.
Blalock A, Hanlon CR:
The surgical treatment of complete
transposition of the aorta and the pulmonary
artery.
Surg Gynaecol Obstet 1950, 90: 1Transposition of the great arteries: history
Surgical atrial septectomy
Although the Blalock-Hanlon
operation and its modifications
were eventually superseded by
Rashkind’s technique of enlarging
the foramen ovale with a balloon
catheter, they produced good
intermediate-term palliation and
were applied in some institutions
for decades after their first
description.Transposition of the great arteries: history
Early arterial switch attempts
In the 50’s : Early arterial switch attempts and techniques of venous
return transfer:
The initial attempts were all universally fatal.
1952: Mustard (Hospital for Sick Children, Toronto): several attempts in infancy
by transferring the LCA into the neoaorta, in isolation, using a monkey lung as a
biological oxygenator.
Mustard WT et Al
The surgical approach to transposition of the great vessels with extracorporeal
circuit.
Surgery 1954;36:39–51.Transposition of the great arteries: history
Early arterial switch attempts
In the 50’s: Early arterial switch attempts and techniques of venous
return transfer:
The initial attempts were all universally fatal.
1955: Ake Senning (Karolinska Institutet, Sweden): after several attempts
concluded that the obstacle to the anatomical correction→transfer of the coronary
arteries
Senning A.
Surgical correction of transposition of the great vessels.
Surgery 1959;45:966–80.Transposition of the great arteries: history
Early atrial switch attempts
1953: Walton Lillehei and Richard Varco described the first attempt of a
physiological repair, consisting of the anastomosis of right pulmonary veins to
RA and the IVC to LA, a technique that became known as the Baffes’
operation (without CPBP, 38 pts, 19 survivers).
Lillehei CW, Varco RL:
Certain physiologic, pathologic, and surgical
features of complete transposition of the great
arteries
Surgery 1953, 34: 376
Baffes TG:
New method for surgical correction of
transposition of aorta and pulmonary artery.
Surg. Gynec & Obst, 1956, 102: 227Transposition of the great arteries: history
Early atrial switch attempts
1954 Harold M. Albert (Children's Memorial Hospital Chicago): flap of
the atrial septum for systemic and pulmonary venous flow redirection in dogs.
Albert HM.
Surgical correction of transposition of the
great vessels.
Surg Forum 1954;5:74–7Transposition of the great arteries: history
Early atrial switch attempts
1957 Alvin Merendino (University of Washington in Seattle):
first attempted to clinically apply a modified Albert’s technique.
Merendino used a premodeled atrial septal prosthesis.
(2 Attempts; both patients died)
Meredino KA et Al
Interatrial venous transposition.
Surgery 1957;42:898–909.Transposition of the great arteries: history
Atrial switch
1957, Ake Senning (Karolinska Hospital): using flaps of
autogenous atrial tissue.
First successful atrial switch.
Senning A.
Surgical correction of transposition of the
great vessels.
Surgery 1959;45:966–80.Transposition of the great arteries: history
Arterial and atrial switch
1961 John W. Kirklin used the Senning
operation at the Mayo Clinic and by 1961 had
operated on 11 infants, with 4 survivors.
Kirklin JW
Open intracardiac repair of transposition of the
great vessels.
Surgery 1961;50: 58–66.Transposition of the great arteries: history
Atrial switch
1963, Bill Mustard (Hospital for Sick Children, Toronto)
atrial switch using an autologous pericardial baffle upon an 18-
month-old girl who had previously undergone a Blalock-Hanlon
operation.
First successful atrial switch using a
pantaloon patch .
Mustard WT.
Successful two-stage correction of the
transposition of the great vessels.
Surgery 1964;55:469–72Transposition of the great arteries: history
Atrial switch
In the ’60s the Senning operation was
largely abandoned to favor a less
complicated Mustard operation.
For the next decade, the Mustard operation
was universally employed.
In the middle 70’s the Senning operation
was eventually revived for the potential
advantage of avoiding prosthetic baffles,
especially in small children.
Quaegebeur JM, Rohmer J, Brom AG.
Revival of the Senning operation in the
treatment of transposition of the great
arteries.
Thorax 1977;32:517–24.Transposition of the great arteries: history
A revolution in palliation
1966: Rashkind and Miller in Philadelphia performed the first balloon atrial
septectomy
1975: Park modified this procedure introducing a blade catheter.
• Rashkind WJ, Miller WW.
Creation of an atrial septal defect without
thoracotomy. A Palliative Approach to
Complete Transposition of the Great Arteries.
JAMA. 1966
• Park SC.
A new atrial septostomy technique.
Cath Cardiovasc Diagn 1: 195, 1975Transposition of the great arteries: history
Arterial switch
1976, Adib Jatene (Hospital das Clínicas, São Paulo): first
succesfull arterial switch in patient with a VSD.
At that time, switch operation was performed
in the presence only either of a VSD or
subpolmonary obstruction
Jatene AD, Paulista et Al
Successful anatomic correction of TGA: a preliminary
report.
Arq Bras Cardiol. 1975
Jatene AD
Anatomic correction of transposition of the great
vessels.
J Thorac Cardiovasc Surg. 1976 Sep;72(3):364-70.Transposition of the great arteries: history
Arterial switch
In the ‘70s: high early operative mortality for switch due to
difficulties in transferring coronary arteries. Alternative
techniques avoiding the transfer of the coronary arteries
were developed By:
•1978 Aubert J
Transposition of the great arteries. New
technique for anatomical correction.
Br Heart J. 1978 Feb;40(2):204-8.
• 1980 Bex JP, Lecompte Y.
Anatomical correction of transposition of the
great arteries.
Ann Thorac Surg. 1980 Jan;29(1):86-8.
• 1975 Stansel HC Jr.
A new operation for d-loop transposition of the
great vessels.
Ann Thorac Surg. 1975 May;19(5):565-7.Transposition of the great arteries: history
Arterial switch
1981, Lecompte : important technical modification avoiding a
an RV-PA conduit.
Lecompte Y, et Al
Anatomic correction of transposition of the great
arteries.
J Thorac Cardiovasc Surg. 1981 Oct;82(4):629-31.Transposition of the great arteries: history
Arterial switch
1984, Aldo Castaneda (Boston Children’s Hospital) and Paul
Ebert demonstrated the feasibility of switch operation for d-
TGA and IVS provided it was performed within the first 3-4
weeks of life.
Castaneda AR, Norwood WI, Jonas RA,
Colon SD, Sanders SP, Lang P.
Transposition of the great arteries and
intact ventricular septum: anatomical repair
in the neonate.
Ann Thorac Surg. 1984 Nov;38(5):438-43.Transposition of the great arteries: history
Arterial switch
1977, Yacoub et Al introduced the two-stage approach by
banding the MPA (with or without systemic-pulmonary artery
shunt) to stimulate the development of left ventricle mass,
followed by arterial switch a few months later.
The majority of patients with TGA have an intact ventricular
septum and no pulmonary stenosis.
Yacoub MH
Two-stage operation for anatomical correction of
transposition of the great arteries with intact
interventricular septum.
Lancet. 1977 Jun 18;1(8025):1275-8Transposition of the great arteries: history
Arterial switch
1988, the Boston Children’s Hospital introduced the concept of
a “two-stage arterial switch operation with IVS (PA banding + B-
T shunt)” limiting the interval between the first and second
operation to an average of 7 days.
Jonas RA, Giglia TM, Sanders SP, Wernovsky G,
Nadal-Ginard B, Mayer JE Jr, Castaneda AR.
Rapid, two-stage arterial switch for transposition of
the great arteries and intact ventricular septum beyond
the neonatal period.
Circulation. 1989 Sep;80(3 Pt 1):I203-8Transposition of the great arteries: history
History of the University of Padua
1974 Vincenzo Gallucci performed the first Mustard operation.
In late ’70s Mustard operation was
abandoned to favor the Senning operation
with excellent outcome (Prof. V. Gallucci;
Prof. A. Mazzucco).
In early ’80s Padua was pioneering the
arterial switch operation in Italy to become
the preferred operation in the presence of
normal coronary arteries anatomy.Transposition of the great arteries: history
History of the University of Padua
1993: The first successful arterial switch operation
for d-TGA and intramural coronary arteries.
Since 1991, over 340 arterial switch operation have
been performed in our institution with a more recent
operative mortality of 2% and excellent long term
results.Transposition of the great arteries: history
Arterial switch
1984, Aldo Castaneda (Boston Children’s Hospital) and Paul
Ebert demonstrated the feasibility of switch operation for d-
TGA and IVS provided it was performed within the first 3-4
weeks of life.Diagnosi
Radiografia del Torace
• Cuore a scarpa
(coeur en sabot)
• Riduzione della
trama vascolare
polmonareCurrent criteria for ToF approach
Current protocol of treatment
• Elective early repair within the first 3 months of
age (in asymptomatic infants)
• Earlier repair when symptoms
«Classic» ToF • No B-T shunt (except for LBW, associated
morbidities) (3 B-T shunts since 2000)
• Cyanotic crises are controlled with β blocker
• No RVOT stenting
• PGE at birth;
ToF + PV atresia neonatal repair
(no MAPCAs)
• PDA stenting (since 2011);
early repairQuadro clinico
I quadri clinici dipendono dal grado di stenosi del RVOT
Età di
presentazione
Stenosi severa Cianosi neonatale 1°
° sett di vita Fallot blu
Stenosi moderata Crisi ipossiche Dopo i 3 mesi di
vita
Stenosi lieve No crisi ipossiche,
Fallot rosa
lieve cianosiCanale atrio-ventricolare completo •Difetto del setto atrioventricolare 1. DIA tipo Ostium Primum 2. DIV tipo inlet 3. Valvola AV comune
Anomalie associate 1. Difetto interatriale e/o forame ovale pervio (DIA) 2. Dotto arterioso pervio (PDA) 3. Origine anomala delle coronarie 4. Difetto del setto interventricolare (VSD) 5. Stenosi della valvola polmonare
Diagnosi
Ecocardiogramma
Permette il corretto inquadramento anatomico visualizzando
• Sbandamento anteriore del setto infundibulare
• Presenza del VSD
• Entità della stenosi del RVOT
- stenosi della valvola polmonare,
- valvola polmonare bicuspide, displasica, atresica o aplasica
- ipoplasia dell’annulus polmonare
- stenosi dinamiche di tipo muscolare
• Grado di ipertrofia ventricolare destro
• Dimensioni delle arterie polmonari
• Anomalie associatePuoi anche leggere