Non dimentichiamoci dell'ipertensione e della terapia - Franco Rabbia - eventi-comunicare.it
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù
Non dimentichiamoci dell'ipertensione e della
terapia
Franco Rabbia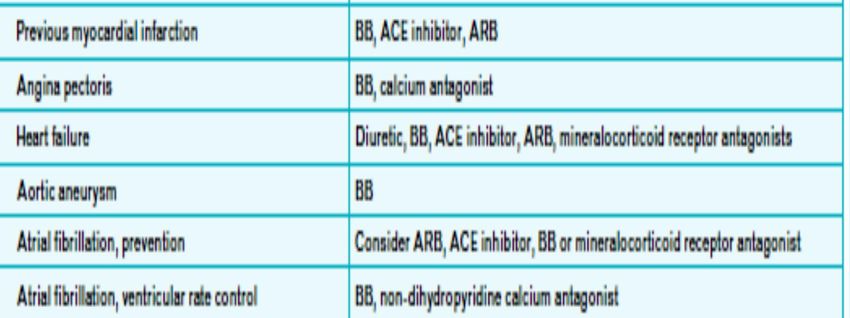
Hypertension Silent killer, global public health crisis, new targets in 2018?

Lg esh 2013
TABLE 3 2013 ESH/ESC Guidelines for the
management of arterial
hypertension: The Task Force for the
management of arterial hypertension
of the European Society of
Hypertension (ESH) and of the
European Society of Cardiology
(ESC)
Mancia, Giuseppe; Fagard, Robert;
Narkiewicz, Krzysztof; Redón, Josep;
Zanchetti, Alberto; Böhm, Michael;
Christiaens, Thierry; Cifkova, Renata;
De Backer, Guy; Dominiczak, Anna;
Galderisi, Maurizio; Grobbee, Diederick
E.; Jaarsma, Tiny; Kirchhof, Paulus;
Kjeldsen, Sverre E.; Laurent, Stéphane;
Manolis, Athanasios J.; Nilsson, Peter
M.; Ruilope, Luis Miguel; Schmieder,
Roland E.; Sirnes, Per Anton; Sleight,
Peter; Viigimaa, Margus; Waeber,
Bernard; Zannad, Faiez; List of
authorsTask Force Members:
Journal of Hypertension. 31(7):1281-
1357, July 2013.
doi:
10.1097/01.hjh.0000431740.32696.cc
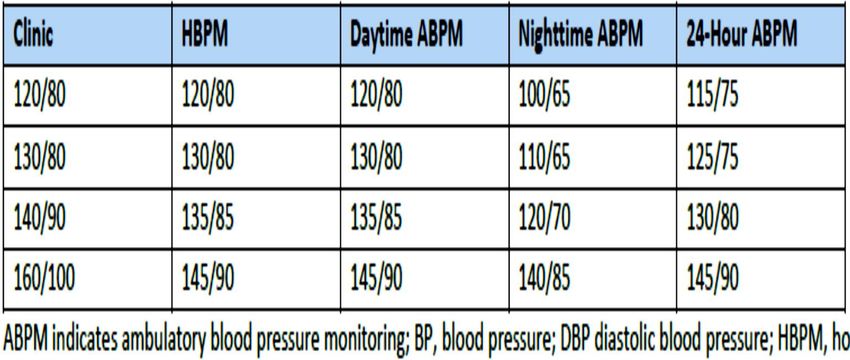
TABLE 3 Definitions and classification
of office blood pressure levels (mmHg)a
Copyright © 2013 Journal of Hypertension. Published by Lippincott Williams & Wilkins. 3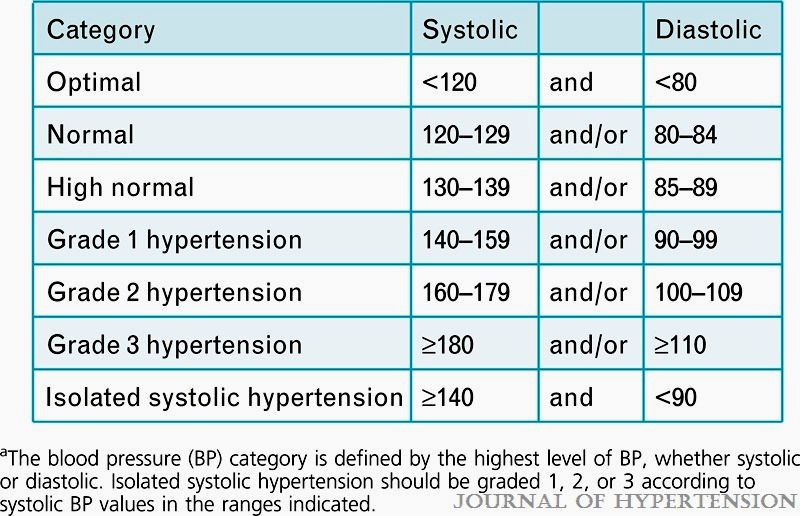
Lg ACC AHA 2017
Futura definizione ESH 2018 ?
Whelton, Hypertension 2017
Obiettivi pressori secondo
le diverse Linee Guida Internazionali (mmHg)
ESH/ESC JNC 8 ASH NICE-BHS CHEP
2013
Age > 80 years < 150/90 < 150/90 < 150/90 < 150/90 < 150/90
Age 60-79 years < 140/90 < 150/90 < 140/90 < 140/90 < 140/90
Age < 60 years < 140/90 < 140/90 < 140/90 < 140/90 < 140/90
Diabetes < 140/85 < 140/90 < 140/90 < 140/90 < 130/80
Nephropathy < 140/90 < 140/90 < 140/90 < 140/90 < 140/90
Proteinuria < 130 * < 130/80 < 130/80
Lg ACC AHA 2017
Whelton, Hypertension 2017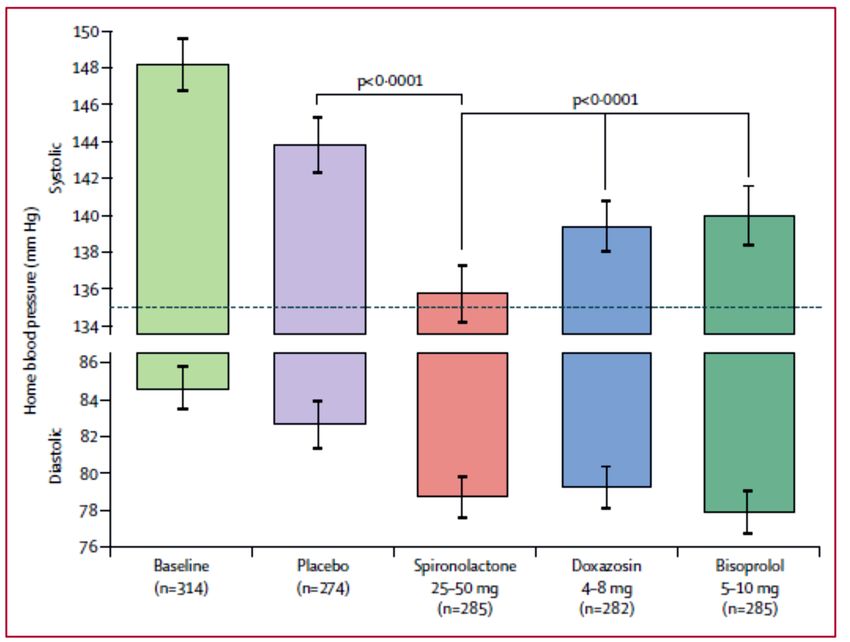
SPRINT. A Randomized Trial of Intensive versus Standard
Blood-Pressure Control
myocardial infarction, other acute coronary syndromes, stroke, heart
failure, or death from cardiovascular causes.
NEJM 2015
Effect of Lowering Diastolic Pressure in Patients
With and Without Cardiovascular Disease
Analysis of the SPRINT (Systolic Blood Pressure Intervention Trial)
Clinical CVD (other than stroke) was defined as
(1) previous myocardial infarction (MI), percutaneous
coronary intervention, coronary artery bypass grafting,
carotid endarterectomy, carotid stenting,
(2) peripheral artery disease with revascularization,
(3) acute coronary syndrome with or without resting ECG
change, ECG changes on a graded exercise test, or
positive cardiac imaging study,
(4) at least a 50% diameter stenosis of a coronary, carotid,
or lower extremity artery, or abdominal aortic aneurysm ≥5
cm with or without repair
Kahn, Hypertension 2018
Effect of Lowering Diastolic Pressure in Patients
With and Without Cardiovascular Disease
Analysis of the SPRINT (Systolic Blood Pressure Intervention Trial)
Kahn, Hypertension 2018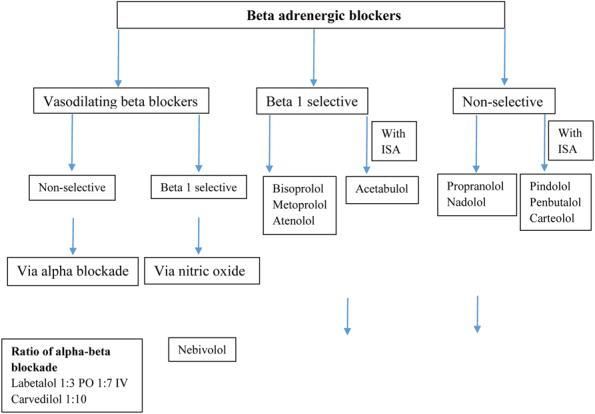
Buon compenso Pressione arteriosa office, dovrebbe associarsi a
buon compenso Pressione out of office
Whelton, Hypertension 2017Reappraisal of European guidelines on hypertension
management: a European Society of Hypertension Task Force document
Combination therapy
Whenever possible, use of fixed dose (or
single pill) combinations should be
preferred, because simplification of
treatment carries advantages for
compliance to treatment.
Mancia, J Hypertension 2009Lg usa 2018
2013 ESH−ESC Recommendations
for Combining BP-lowering Drugs
Preferred
Useful (with some limitations) Thiazide Diuretics
possible but less well tested
Not recommended
b-blockers Angiotensin
receptor blockers
(ARBs)
Other Calcium channel
Antihypertensives blockers (CCBs)
Angiotensin-converting enzyme (ACE)
inhibitors J Hypertens 2013LINEE GUIDA ESH 2013
TERAPIA DI COMBINAZIONE
Diuretici
Tiazidici
Calcio
antagonisti ARB/ACEI
Mancia, J Hypertension 2013CRITERI PER L’ASSOCIAZIONE DI
FARMACI ANTIPERTENSIVI
1. Associare farmaci con lo stesso profilo farmacocinetico in termini
di tempo di picco e di durata d’azione
2. Associare farmaci che hanno meccanismi d’azione diversi, ma
complementari
3. L’efficacia antipertensiva dell’ associazione deve essere superiore
all’ efficacia di ciascun singolo componente.
4. L’associazione deve minimizzare gli effetti umorali/collaterali
indesiderati.
Effetto Additivo: 1+1=2
Sinergismo: 1+1>2ASSOCIAZIONI ANTIPERTENSIVI
NON RAZIONALI
Effetto subaddittivo: 1+1> 1 ma < 2
Antagonismo: 1+1< 1
Associazione di Farmaci con Interazione Negativa
sull’Effetto Ipotensivo
- 1-Bloccante+ Clonidina
Associazione di Farmaci Antipertensivi Potenzialmente Pericolosa
- b-Bloccante + Clonidina
- b-Bloccante + Ca-antagonista non DHPCurve Dose-Risposta dei Farmaci Cardiovascolari
FARMACO A FARMACO B
PA PA
5 10 15 20
5
10
15
20
0 6 12 18 24 0 6 12 18 24
Durata d’azione (h) Durata d’azione (h)
Il farmaco di tipo A ha curva efficacia-durata Il farmaco di tipo B ha curva dose-risposta
ACE-I CCB
Diuretici
AIIRA
-bloccanti
β-bloccanti
Fogari, J Hypertens, 1997Drugs to be preferred in specific conditions
2013 ESH/ESC Hypertension Guidelinesß-blockers and the treatment of hypertension
Headace
Messerli, Lancet 2007Properties of commonly used [beta]-blockers
Betabloccanti e sonno
Più sono lipofilici più causano insonnia e incubi riducendo il sonno
NREM
1. Propranololo
2. Metoprololo
3. Labetalolo
4. carvedilolo
Reddy, American Journal of Therapeutics, 20167IPERTENSIONE RESISTENTE
Definizione
L’ipertensione resistente è definita come una
pressione sistolica e/o diastolica che rimane
superiore al target pressoriononostante
un’adeguata correzione dello stile di vita e una
terapia farmacologica con almeno tre farmaci a
dosaggio pieno compreso un diuretico
Guidelines for Management of Hypertension ESH ESC 2013Therapeutic drug monitoring guided definition of adherence profiles in
resistant hypertension and identification of predictors of poor adherence.
Referred n=1250 (100%)
Not RH
n=1105 (88,4%)
RH criteria n=145 (11,6%)
WCRH
n=36 (1,44%)
24h ABPM n=109 (9,2%)
Sec. Hypertension
n=22 (2,9%)
Secondary hypertension n=87 (6,8%)
Suboptimal treatment
n=37 (3%)
Treatment optimisation
Eligible for the study n=50 (4%)
Studio TDM Torino Rabbia F, Avataneo V. Br J clin Pharmacol 2018Antihypertensive drug therapy in
patients with resistant hypertension
Rimoldi Eur Heart J 2015Spironolactone versus placebo, bisoprolol, and doxazosin to determine the
optimal treatment for drug-resistant hypertension (PATHWAY-2): a
randomised, double-blind, crossover trial
Lancet 2015Spironolactone Versus Clonidine as a Fourth-Drug Therapy for
Resistant Hypertension
The ReHOT Randomized Study (Resistant Hypertension Optimal Treatment)
Office BP
Krieger, Hypertension 2018Why in 2016 are patients with hypertension not
100%
controlled? A call to action
Redon, J Hypertension 2016Gap esistente tra la prescrizione scritta
e l’uso dei farmaci
25-30
50-70 48-66 15-20
Per ogni 100 vengono
vanno in escono dalla vengono
prescrizioni assunte
farmacia farmacia rinnovate
correttamente
National Association of Chain Drug Stores, Pharmacies: Improving Health, Reducing Costs, July 2010. Based on IMS Health data.
American College of Preventive Medicine http://www.acpm.org/?MedAdherTT_ClinRefBournier: Pharmacol Res 2017
Adherence to Drugs That Prevent Cardiovascular Disease:
Meta-analysis on 376.162 Patients
Primary prevention Secondary prevention
Naderi et al, Am J medicine 2012Rabbia , Fulcheri, High Blood Press, 2016
Colloquio con il paziente
Metodi non invasivi
NON ADERENZA TERAPEUTICA
Diario
Questionario
Revisione delle prescrizioni (farmacista, MMG)
Accuratezza -
Accuratezza
Costi --
Conteggio delle pillole
Costi -
Metodi invasivi
Telemedicina Osservazione diretta
del paziente
Misurazione
farmaco/biomarcatore
plasma/urine (TDM) Monitoraggio
Accuratezza +++ elettronico
Costi +++
METODICHE DI VALUTAZIONE Accuratezza ++++
Costi
Rabbia, ++ High Blood Pressure 2016
Fulcheri:Risk Factors for Nonadherence to Antihypertensive Treatment
1380 pazienti ipertesi
Gupta. Hypertension 2017Percentuale
di non
aderenti
Hypertension 2016STUDIO TDM-TORINO
Rabbia F, Avataneo V. Br J clin Pharmacol 2018STUDIO TDM-TORINO
Rabbia F, Avataneo V. Br J clin Pharmacol 2018Possibili rimedi alla non aderenza • Medico ruolo primario nella educazione e motivazione continua del paziente • Fondamentale rapporto con paziente (più tempo) per migliorare aderenza • Controllare alcuni parametri indiretti (ad es FC se betabloccante o CA non diidropiridinico) piuttosto che concentrazione farmaco • Misuratori PA per automisurazione nell’attesa della visita da MMG • Applicazioni tecnologiche per “remind” e/o informazioni • Utilizzare farmaci in associazione • Ruolo farmacista: collaborazione vs barriera
A strategy to reduce cardiovascular disease by more
than 80%
Wald BMJ 2003“…the most effective therapy prescribed
by the most careful clinician will control
hypertension
only if the patient is motivated to take the
prescribed medication
and to establish and maintain a health-
promoting lifestyle.”
NEJM 2005Puoi anche leggere

















































