I TEMI DI VISUALIZZAZIONE, ESPOSIZIONE E MANIPOLAZIONE NELLA CHIRURGIA TRANSORALE: EXCURSUS STORICO, LA CHIRURGIA ROBOTICA TRANSORALE (TORS) E ...
←
→
Trascrizione del contenuto della pagina
Se il tuo browser non visualizza correttamente la pagina, ti preghiamo di leggere il contenuto della pagina quaggiù

I TEMI DI VISUALIZZAZIONE, ESPOSIZIONE E
MANIPOLAZIONE NELLA CHIRURGIA TRANSORALE:
EXCURSUS STORICO, LA CHIRURGIA ROBOTICA TRANSORALE
(TORS) E NUOVE PROSPETTIVE
Relatori: Alberto Caranti, Mauro Budini
Tutor: prof. Claudio Vicini
UN CAMPO OPERATORIO DI DIFFICILE ACCESSO

UNA CHIAVE DI LETTURA CHE CORRE SU TRE BINARI PARALLELI

1885: IL TEMA DELL’ESPOSIZIONE E LA
CHIRURGIA TRANSORALE MODERNA
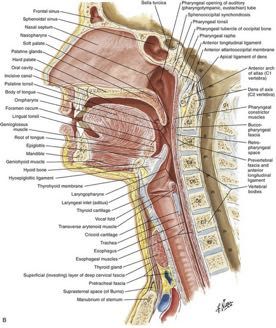
Per poter performare efficacemente un intervento transorale, era necessario
rettilinearizzare cavo orale, faringe e laringe. Nacquero a questo scopo i primi
laringoscopi tubulari.
Negli anni a seguire fu un fiorire di varianti sul tema, vale a dire che vennero
introdotti laringoscopi dalla lunghezza, dal diametro e dalle forme sempre più
variabili e adattate alle esigenze del chirurgo e alle variabili anatomiche e
patologiche dei pazienti.
risultato è quindi quello di avere sì l’esposizione delle corde vocali e della
che il laringoscopio offre la prospettiva su di un campo operatorio bidimensionale e statico,
operatorio che se ne ricava è estremamente ridotto in superficie.
introducendo un problema non indifferente sia per quanto riguarda la percezione della profondità di
campo dell’operatore, percezione che si è dimostrato migliorare seguendo una curva
Dall’altro lato si è introdotto un handicap dal punto di vista della visualizzaz
VISUALIZZAZIONEdistretto anatomico che rimane all’interno del: collo, ad una profondità di dive
d’apprendimento molto lenta, sia per quanto riguarda la possibilità di adattare l’esposizione ad
eventuali modifiche [2].
E MANIPOLAZIONE
orale, è chiaro che la luce ambientale in grado di raggiungere il campo oper
non addirittura
Resta quindi da districare il nodo della manipolazione. Da un certo punto nulla quando
di vista il problema è lo l’interno del laringoscopio viene occupato dagli
è quindi
stesso dell’esposizione, vale a dire uno spazio estremamente limitato reso necessario
dal punto introdurre un sistema di illuminazione che consentiss
di vista delle
Con l’introduzione del laringoscopio tubulare si arrivò ad esporre opportunamente
esaminare
dimensioni attraverso il quale far passare gli strumenti e quindi performare il campo
l’intervento. operatorio ora esposto. Inizialmente allora si partì dallo s
Ricordiamo
il campo operatorio.
infatti che il limite che avevamo posto a inizio trattazione, vale a diredire una lente
la ridotta riflettente
apertura posizionata sul capo dell’operatore che avesse com
del cavo
Resta
orale, non viene di fattoperò
risolto, siilrende
problema inerente
pertanto necessario il tema
che la manoconfluiredella
quanta
del chirurgo VISUALIZZAZIONE,
più luce
rimanga dato
possibile su di un determinato
esterna che
punto di interesse. La
al cavo oralebaselingua, faringe
stesso. Questo significa che gli e laringe
strumenti rimangono
dovranno celati
essere estremamente
dotata in uno
lunghi
di un piccoloper spazio
poter
pertugio anatomico
attraverso ristretto
il quale l’occhio e potesse “
del chirurgo
essere gestitilontano
dalla manodalla luce ambientale.
dell’operatore e raggiungere al contempo la laringe, attraversando tutta
l’estensione del laringoscopio (Fig. 3A e Fig. 3B).
E ancora, abbiamo il problema inerente il tema della
MANIPOLAZIONE, abbiamo il problema di quali
strumenti utilizzare per manipolare un tessuto
attraverso un tubulare dal diametro di pochi centimetri.
Fig. 2: Specchio frontale.
COSA RESTA DA RISOLVERE? ESPOSIZIONE: • Il campo operatorio è ora esposto ma resta difficilmente accessibile per via delle limitazioni intrinseche nel laringoscopio. VISUALIZZAZIONE: • Illuminazione comunque limitata; • La sezione di pochi centimetri e la distanza tra l’occhio dell’operatore ed il campo operatorio limitano la visualizzazione. MANIPOLAZIONE: • Effetto fulcro • Tremore • Movimenti limitati

1960: L’AVVENTO DEL MICROSCOPIO ED IL
PROGRESSO IN CAMPO DI VISUALIZZAZIONE
Nel 1960 G. J. Jako introduce il microscopio ottico nella microchirurgia della
laringe, strumento che permetteva di magnificare il campo operatorio con
ingrandimento del 6x fino al 10x.
Migliora sensibilmente la capacità del chirurgo di esaminare il campo operatorio,
apprezzandone decisamente meglio l’anatomia.
Ma come abbiamo imparato, quando su uno dei tre binari si registra un progresso,
esso rappresenta un trigger anche per gli altri due. Viene stimolata la
MANIPOLAZIONE, con l’introduzione di alcune novità:
• Strumenti miniaturizzati
• Laser a CO2
IN FONDO, SI POTREBBE DIRE CHE POCO È CAMBIATO… Gustav Killian, 1910 2017

2005: HOCKSTEIN ET AL PUBBLICANO SU
THE LARYNGOSCOPE IL PRIMO CASO DI
TORS
Neil G. Hockstein et al. individuano per prima cosa i 3 punti critici che hanno
ostacolato l’avvento della chirurgia robotica nel campo ORL:
1. L’introduzione dei bracci robotici all’interno del cavo orale, a raggiungere la
faringe e laringe,
2. Ottenere un’adeguata esposizione della laringe senza entrare in conflitto con le
braccia del robot,
3. Assicurare un adeguato managing delle vie aeree.are un adeguato managing delleThevie aeree.
Laryngoscope
Lippincott Williams & Wilkins, Inc.
© 2005 The American Laryngological,
Rhinological and Otological Society, Inc. Il passo successivo alla sperimentazione su cadavere fu quello di passare ad un sis
risolvere questi tre problemi, Neil G. Hockstein et al. hanno quindi deciso di simulare
farlo fu scelto il modello canino. Si procedette quindi ad un primo intervento di
Robotic Microlaryngeal Surgery: A Technical
e di interventi su dei modelli sintetici di faringe e laringe, utilizzando il una
robot chirurgico della glottide su cani anestetizzati ed intubati. Lo scopo della s
microchirurgia
Feasibility
andosi del primo approccio robotico Study
alla chirurgia della Using
laringe, furono thesedaVinci
sperimentati
quello di verificare Surgical
fosse possibile trasferire i vantaggi che si erano individuati su
Robot
ti utili ad assicurare una adeguata and
esposizione, an Airway
dal laringoscopio Lindholm Mannequin
(Fig. 1)
e su cadavere anche in vivo. La tecnica e gli strumenti utilizzati furono gli stessi
McIvor (Fig. 2), diversi tipi di strumenti chirurgici con cui venivano attrezzati
precedenti.i bracci
In questo caso si vollero valutare:
alibri variabili (diametri di 5 eNeil
8 mm), e con MD;
G. Hockstein, varie funzioni
J. Paul Nolan;( Bert
forbici dalla
Se punta
W. -O’Malley,
viJr, MD; Y.differenze
fossero Joseph Woo, MDperformance fra l’utilizzo di strumenti di 5 m
the
nze e tagliente), fino a diversi tipi di ottiche, utili ad ottenere sia una visualizzazione
diametro, in questo caso forbici dalla punta arrotondata e forcipe Debakey
Sempre nella
che tridimensionale. medesima pubblicazione
mally invasive surgery però,
Objectives/Hypothesis: The trend toward mini-
- Le
has led to the development trova
vasivespazio la sperimentazione,
cally. Key Words: Robotic, endoscopic, minimally in-
tempistiche dimicrosurgery,
surgery, intervento, larynx, daVinci. sotto forma
and mastery of endoscopic and laparoscopic surgical Laryngoscope, 115:780 –785, 2005
techniques. These minimally invasive approaches, - L’emostasi,
di simulazioni su modelli sintetici di laringe, fatte utilizzando il Da Vinci .
which only two decades ago were either novel or ex-
perimental, are now mainstream. More recently,
INTRODUCTION ®
Over the last century, surgical innovation has bene-
robot-assisted surgery has evolved as an adjunct - to La visualizzazione del campo operatorio.
fited from discovery in other fields of study. Perhaps the
open and endoscopic techniques. Surgical robots are
greatest improvement in outcome after total laryngectomy
now approved by the United States Food and Drug
Administration for a variety of thoracic and abdomi- resulted from the discovery of antibiotics.1 In the field of
nal/pelvic surgical procedures. The purpose of this rhinologic surgery, the development of surgical telescopes
study is to demonstrate the technical feasibility of and the computed tomography scanner have led to revo-
robot-assisted microlaryngeal surgery. Study Design: lutionary advances in the treatment of diseases of the
Experimental surgical manipulation of the larynx paranasal sinuses.2 The recent advances in surgical robot-
in an airway mannequin with a surgical robot. ics emerged after the development of robotic technology
Methods: A variety of laryngoscopes and mouthgags, for industrial and aerospace applications. Surgical robot-
coupled with the daVinci Surgical Robot’s (Intuitive ics required miniaturization of both the mechanical ro-
Surgical, Sunnyvale, CA) 0-degree and 30-degree, two- botic components and the solid-state components. These
dimensional and three-dimensional endoscopes, were
miniaturized robots coupled with improved three-
utilized to optimize visualization of the larynx in an
airway mannequin. Five millimeter and 8 mm micro- dimensional optic technology have paved the way for ad-
instruments compatible with the daVinci robot were vancement and application of surgical robotic technology.
utilized to manipulate different elements of the lar- The advantages that surgical robots have brought to
ynx. Experiments were recorded with both still and abdominal and thoracic surgery can be applied in the head
video photography. Results: The endoscope and ro- and neck as well. The primary obstacles to the perfor-
botic arms of the daVinci robot are well suited to mance of robotic-assisted pharyngeal and laryngeal sur-
airway surgery. Conclusions: Robot-assisted laryn- gery are 1) the introduction of the robotic arms and in-
geal surgery can be performed with currently avail- struments into the narrow funnel created by the oral
able technology. The potential for fine manipulation cavity, pharynx, and larynx, 2) the means of suspending
of tissues, increased freedom of instrument move- and exposing the larynx to allow for adequate exposure
ment, and endolaryngeal suturing may increase the
without interfering with introduction of the robotic arms,
Fig. 1: Laringoscopio di Lindholm
precision of endoscopic laryngeal microsurgery and
and 3) a means of managing the airway. To assess the
offers the potential to increase the variety of laryn-
geal procedures that can be performed endoscopi- potential to overcome these obstacles, we simulated sev-
Fig.
eral 5: Forbici
endoscopic a punta
pharyngeal andarrotondata (sullaus-
laryngeal procedures dx) e forcipe di Debakey (su
Fig. 2: Apribocca di McIvor con lame di diversa ing themisura.
daVinci surgical robot.
Abstract submitted for presentation at the 2005 Annual Meeting of
the Triologic Society.
MATERIALS AND METHODS
From the Department of Otorhinolaryngology—Head and Neck Sur-
Using the daVinci Surgical Robot (Intuitive Surgical,ANCORA STUDI PRELIMINARI
The Laryngoscope
Lippincott Williams & Wilkins, Inc.
© 2005 The American Laryngological,
Rhinological and Otological Society, Inc.
Robot-Assisted Pharyngeal and Laryngeal
Microsurgery: Results of Robotic Cadaver
Dissections
Neil G. Hockstein, MD; J. Paul Nolan, BS; Bert W. O’Malley, Jr, MD; Y. Joseph Woo, MD
Objectives/Hypothesis: Robotic surgery has signif- ryngeal and microlaryngeal surgery. Surgical robots
Transoral Robotic Surgery (TORS): Glottic
icant potential in pharyngeal and microlaryngeal sur- offer the ability to manipulate instruments at their
gery. We demonstrate the use of a surgical robot in distal ends with increased freedom of movement,
Microsurgery in a Canine Model
pharyngeal and microlaryngeal surgery in a cadaver. scaled movement, tremor buffering, and under ste-
Study Design: Six experimental surgical dissections, reoscopic three-dimensional visualization. Surgical
modeled after commonly performed pharyngeal and robots may increase the precision with which we per-
microlaryngeal procedures, were performed in a ca- form currently described procedures; 1 additionally,
Bert W. O’Malley, Jr.,
daver with a commercially available surgical robot in Gregory S. Weinstein,
surgical androbots
Neil mayG. Hockstein
advance the field of endoscopic
an The
operating room suite to demonstrate proof of con-
Laryngoscope laryngeal and pharyngeal surgery. Key Words: Ro-
Lippincott
cept. Williams
Methods: & Wilkins,
Using Inc.
the daVinci Surgical Robot (In-Pennsylvania
Philadelphia, botic, endoscopic, minimally invasive surgery, micro-
© 2006 The American Laryngological,
tuitive Surgical,
Rhinological Sunnyvale,
and Otological Society, CA),
Inc. surgical procedures surgery, larynx, partial laryngectomy, lateral pharyn-
were performed on an edentulous, female cadaver. gotomy, laryngeal cancer, daVinci.
The procedures included 1) bilateral true vocal cord Laryngoscope, 115:1003–1008, 2005
stripping, 2) rotation Summary: Objectives/Hypothesis:
of a mucosal flap from the epi- We hypothesize that bimanual, three-
Assessment of Intraoperative Safety in
glottis to the anterior dimensional
cordectomy, 4) arytenoidectomy,
robotic surgery
commissure,
cedures. Study Design:5) partial
will prove
3) partial vocalvaluable for Robot-assisted
epiglottec-
To test
glottic microsurgical
this hypothesis,olutionizing
we developed theand
cardiac
optimized
ways
pro-and urologic surgery are rev-
in which cardiac valvular disease
Transoral Robotic Surgery
tomy and thyrohyoid dissection
a canine model for and 6) partial
glottic resec-using aand
microsurgery commercially available
prostate cancer aresurgi-
being treated. Surgeries are being
tion of the base ofcal tongue
robot. with
Methods primary
Using aclosure.
da Vinci All performed
Surgical Robot without
(Intuitive largeInc.,
Surgical, thoracotomies or laparotomies,
procedures were timed andCA),documented with still
Sunnyvale, glottic microsurgery morbidity
was performed withis adecreased,
hydrodissectionand patients are leaving the hos-
and video photography. Results: The daVinci Surgical
Robot, with currently technique in a canine
available model. The
instruments, experiments pital
enabled sooner.1,2 These
were performed on twoimproved
orotra- outcomes are the result of
Neil G. Hockstein,
performance cheal
of severalMD; intubated
Bert W.
laryngeal mongrel
and dogs
O’Malley,
pharyngealunder general
Jr.,sur- many
anesthesia
MD; Gregory S. assets
in theofsupine
surgical
Weinstein, MDrobotics, including improved op-
position
gical procedures onona acadaver.standard Laryngeal
operating room andtable.
pharyn- tics,and
A videoscope increased freedomrotat-
two, 360-degree of endoscopic instrument move-
geal exposure wasing, excellent, instruments
5- and 8-mm, wrested-end movement ment,were
effector instruments and introduced
tremor filtration.
transor-
was unimpeded, tissue handling
ally with three wasroboticdelicate and surgeon
arms. The pre- performed Thethepotential to apply the advantages of robot-
actual procedures
cise, and endolaryngeal suturing was relatively easily assisted surgery to the pharynx and larynx is great, and
Introduction: whileRobotic
positionedtechnology
at a robotic has been
system console that transoral
was located surgery.
across Additionally,
the oper- we discuss sev-
performed. The duration of the different robotic ca- previous work andhas to
demonstrated the technical
safely integrated into
ating thoracic
room suite. Theand abdominopel-
procedure was performed eral
in strategies
duplicate was increase
docu- patient safety feasibility
in TORS.
daver dissections
vic surgery, and was comparable
the with
early to procedure dura- ofKey
introducing
Words: the roboticwas instruments through the mouth
tion using mented
conventional stillexperience
andConclusions: has been Results:
video photography. Glottic Robotic,
microsurgery endoscopic, minimally inva-
very promising withtechniques.
veryperformed
successfully rare complications
using
Us-
the da Vinci into
sive
re- Surgical the pharynx
surgery,
Robot, and
both larynx.
with microsurgery,
3
5- and Thelarynx,
breadthpartial
of pharyngeal
laryn-
inglated
the todaVinci Surgical Robot,
robotic device failure. Recently, severalsix different gectomy, laryngeal cancer, DaVinci,
and microlaryngeal surgical procedures and transoral ro-
specific appli-
pharyngeal
reports have and microlaryngeal
documented thedissections
8-mm instrumentation. technical were
The smaller, suc-
5-mm instruments
feasibility botic in afforded greater
surgery visu-
cessfully performed in a cadaver. The recent develop- cations which a(TORS),
surgical complications.
robot may be useful have not
alization of the operative
of transoral robotic surgery (TORS) with the da- site and increased maneuverability, which resulted in
Laryngoscope, 116:165–168, 2006
ment of surgical robotics has a potential role in pha- been identified. To assess potential applications of robot-Annul.\ ofOtnhgy. Rliinohsy & Ijiryni-iilofiy lift I): 19-23.
© 2tK)7 Annals Piibliihing Company. All rights reserved.
Transoral Robotic Surgery: Supraglottic Partial Laryngectomy
Gregory S. Weinstein, MD; Bert W. O'Malley, Jr, MD; Wendy Snyder;
NeilG.Hockstein,MD
Objectives: We assessed the feasibility of performing transoral supraglottic partial laryngectomy with robotic instrumen-
tation.
Il primo caso il mondo di utilizzo della TORS su di un paziente umano vivo, fu
Methods: Transoral robotic surgery (TORS) was performed on 3 human patients with supraglottic carcinoma in a pro-
spective human trial. Tlie study was approved by our institutional review bourd and involved the da Vinci Surgical Robot
realizzato presso il Dipartimento di otorinolaringoiatria dell’Università della
(Intuitive Surgical, Inc. Sunnyvale, California). I
Results: Ail procedures were completed robotically. The median overall operation time to perform Ihe robotic procedure
was 120 minutes (range. 1:32:48 to 2:58:18), including 18 minutes (range.00:6:07 to (K):3O:39J for exposure and robotic
Pennsylvania, in Philadelphia. Tra il mese di maggio e ottobre 2005, tre pazienti
positioning. There were no intraoperative or postoperative complications or surgical mortality.
Conclusions: Tlie preliminary results of our series suggest that application of the da Vinci robotic surgical system for
TORS H) supragloiiic partial laryngectomy is technically feasible and relatively safe. Furthermore. TORS provides ex-
vennero trattati tramite TORS, con interventi di laringectomia parziale sopraglottica.
cellent surgical exposure that allows complete lumor resection. Most importantly, TORS provides aii alternative to open
approaches and "conventional" transoral supraglottic partial laryngectomy.
Key Words: da Vinci Surgical Robot, minimally invasive surgery, robotics, supraglottic cancer, supraglottic surgery,
• Retrattore FK transoral robotic surgery.
• Ottica endoscopicaT^^rRODucTION
con inclinazione 30° acronym TORS (transoral robotic surgery) in a de-
scription of supraglottiu laryngectomy in a canine
Transoral laser supraglottic partial laryngectomy
by means of standard instrumentation with an oper- model by means of the robotic system. Transoral ro-
• Forcipe di Cadiere e Spatola cauterizzante
ative microscope and a carbon dioxide laser is gen- botic surgery is defined as surgery done via the oral
erally accepted for diagnostic and therapetitic proce- cavity that uses a minimum of 3 robotic arms and al-
dures in patients with supraglottic malignant lesions. lows for bimanual surgical techniques.'^ We present
Although in many cases standard instrumentation the world's first cases of TORS supraglottic partial
Non vennero riscontrate complicanze intra o post operatorie
provides excellent exposure that allows for a suc-
cessful transoral operation, in some cases, the tumor
laryngectomy performed in human patients.
MATERIALS AND METHODS
location may render present standard approaches Patients. From May to October 2005. a total of 3
suboptimal and technically challenging, thus possi- patients underwent supraglottic partial laryngecto-
bly increasing the ri.sk of surgical complications. my in a pilot study to assess TORS as part of a Uni-
The recent introduction of robotic systeins has re- versity of Pennsylvania Institutional Review Board-
sulted in improved surgical approaches in various approved protocol. Informed con.sent was obtained
surgical fields. The two specialties in which the da from al! patients. The median age of the 3 patientsI PUNTI DI FORZA In conclusione di questa esperienza, gli autori sottolineano come la TORS porti con se degli innegabili vantaggi: • I movimenti della mano sono fedelmente trasmessi dalle pinze della consolle agli strumenti chirurgici, che grazie ai 6°di libertà consentono movimenti molto più ampi rispetto agli strumenti tradizionali; • Il robot permette di evitare il cosiddetto “effetto fulcro”; • L’alta definizione e la visuale 3D consentono di avere una visualizzazione estremamente superiore a qualunque altra.
GLI SVANTAGGI Tuttavia vengono anche segnalati due potenziali handicap di cui la TORS potrebbe risentire: • La mancanza di un feedback tattile che non consente al chirurgo di avere una sensazione circa la consistenza del tessuto che sta manipolando, • Il costo estremamente alto della chirurgia robotica, inteso come costo per l’acquisto del robot Da Vinci, • Il costo annuale per l’utilizzo, il costo degli strumenti chirurgici (che possono essere usati al massimo per 20 interventi prima di essere sostituiti)
RITORNIAMO ALLORA AL NOSTRO SISTEMA DI LETTURA A TRE BINARI…
… E FACCIAMO IL PUNTO DELLA
SITUAZIONE
VISUALIZZAZIONE:
Ora abbiamo una visualizzazione adeguata, grazie ad ottiche endoscopiche ad
alta definizione ed un sistema binoculare di visione 3D.
MANIPOLAZIONE:
La manipolazione è resa ottimale dalle braccia robotiche che vengono
introdotte all’interno del cavo orale e che godono di 6 gradi di libertà.
ESPOSIZIONE:
Utilizzo di vari modelli di apribocca per aumentare l’esposizione quanto più
possibileDEI TRE TEMI, L’ESPOSIZIONE
NEW DIMENSIONS È QUELLA in TORS, Endoscopic Laser Surgery and Conventional Microsurgery
CHE ANCORA RAPPRESENTA UN PROBLEMA Through its unrestricting design, the FK-WO TORS laryngo-pharyngosope retractor
offers unique exposition of the upper aerodigestive tract especially during TORS
(Trans-Oral Robotic Surgery), microsurgery or laser surgery of the base of tongue,
Circa mezzo secolo più tardi, nel 1961, sarà Dingman larynx
(Fig.and3)hypopharynx.
ad introdurre un'altra
In comparison with themodifica,
standard laryngoscopes, the non-
tubular concept of this device allows better view into the operation area, an improved
costruendo un apribocca dal design chiuso, per l’appunto access
l’apribocca di Dingman,
to it and easier manipulation dove la C aperta
of instruments.
del Crowe-Davis diveniva un rettangolo e dove venivano aggiunti anche due retrattori (uno per lato)
NON-TUBULAR DESIGN,
a sostenere le guance. FRAME CONSTRUCTION WITH
WIDE APERTURE
• The operation field is not restricted
like it is the case when using standard
operation laryngoscopes
• Ample space is provided even for
robotic instrument placement in TORS
• Movement and manipulation of
instruments is facilitated
ADJUSTABLE ANGLES OF
THE BLADES MOVING UPWARDS
AND DOWNWARDS
FORWARD AND BACKWARD
MOVEMENT OF THE BLADE FOR DEEP
OR LESS DEEP INTRODUCTION
• Excellent view of the anatomic
structures as the operation field
can be ideally exposed
• Head reclination only moderate
Fig 3. Apribocca di Dingman
Apribocca di McIvor con lame di diversa misura.
Per esporre il Ovviamente,
camponeloperatorio e permettere uno spazio di manovra il più ampio
corso degli anni si sono continuati a reinventare questi apribocca, modificandone
forme, inserti e dotazioni, ma mantenendone sempre rigidamente la struttura di base.
possibile alle braccia robotiche, si sono utilizzati diverse tipologie di apribocca.
autori riscontrarono nell’utilizzo del Da Vinci fu appannaggio della
dimensionale, resa possibile dall’utilizzo di due ottiche con focali, che
inoculare degli occhi umani, garantiva all’operatore
IL TEMA la percezione
DELL’ESPOSIZIONE della
NELLA TORS Exposure of oropharynx Exposure of larynx Exposure of hypopharynx and upper esophagus
utamente non consentita dalla visione bidimensionale delle ottiche
Arriviamo dunque alla quadratura del cerchio, e a dare un significato a questo focus sugli apribocca
3D ha un diametro di 10 mm e fu testata con diverse
che abbiamo appena inclinazioni
discusso. Con larispetto
comparsa del Da Vinci®, la chirurgia transorale ha sicuramente
goduto
e a 30 gradi, dove l’inclinazione a 30 di risulto
gradi un’implementazione
ottimale. in termini di manipolazione, dove le braccia robotiche si sono
sostituite alle mani del chirurgo aggirandone diversi limiti, e di visualizzazione, grazie alle ottiche diAn Overview of Retractor Systems Used in Transoral Robotic Surgery
Emily Funk, BA; Aaron Baker, MD, MS (presenter); David Goldenberg, MD; Neerav Goyal, MD, MPH
An Overview of Retractor Systems Used in Transoral Robotic Surg
ives: To review available literature on current retractor Emily Funk, BA; Aaron Baker, MD,Features
Retractor MS (presenter); David Goldenberg, MD; Limitations
Neerav Goyal, MD, MPH
ms used for transoral robotic surgery (TORS) in the oropharynx, Crowe-Davis Open lateral frame, easily accessible, familiar Limited base of tongue, hypopharynx, and larynx exposure
harynx and larynx, and obtain in-situ images.
Limited base of tongue, hypopharynx, and larynx exposure, closed
McIvor Easily accessible, familiar, useful in edentulous patient
Retractor Features frame Limitations
ods: A query was performed
Objectives: to identify
To review fullliterature
available text articles related retractor
on current
RS and the use of the Crowe-Davis Mouth Gag, McIvor(TORS)
Mouthin the oropharynx, Limited base of tongue, hypopharynx, and larynx exposure, closed
systems used for transoral robotic surgery Dingman Wide frame, cheek retractors, tie
Crowe-Davis down
Open points,
lateral accessible
frame, easily accessible, familiar Limited base of tongue, hypopharynx, and lar
frame
Dingman Mouth Gag, Feyh-Kastenbauer
hypopharynx and larynx, and (FK)
obtain Retractor,
in-situ images.
geal Advanced Retractor System (LARS) and Medrobotics Flex Wide frame, various blades designed Limited base of tongue, hypopharynx, and larynx
FK/ FK-WO McIvor Easily for exposurefamiliar,
accessible, of specific areas,
useful in edentulous patient Closed frame, expense
integrated suction, modified for TORS (FK-WO) frame
tor System. Images Awere
Methods: obtained
query in cadaveric
was performed to specimens.
identify full text articles related
to TORS and the use of the Crowe-Davis Mouth Gag, McIvor Mouth Designed for laryngeal procedures, curved frame, various blades, Limited base of tongue, hypopharynx, and larynx
LARS Dingman Wide frame, cheek retractors, tie down points, accessible Closed frame, expense
s: The demand for novelMouth
Gag, Dingman TORS retractor systems is being met
Gag, Feyh-Kastenbauer (FK) Retractor, vertically adjustable blades, instrument attachments frame
he evolution of a variety
Laryngeal of devices.
Advanced The goal
Retractor of these
System (LARS) systems
and Medrobotics Flex Flex
Medrobotics Designed for TORS, curvedWide frame various
frame, blades,
various bladedesigned
blades adjustment forinexposure of specific areas,
mprove exposure of the surgical site, while accommodating an FK/ FK-WO Closed frame, expense Closed frame, expense
Retractor System. Images were obtained in cadaveric specimens. (FRS) multiple planes, integraged integrated suction
suction, modified for TORS (FK-WO)
racheal tube, endoscope, and robotic effector arms. Standard
Designed for laryngeal procedures, curved frame, various blades,
h gags such as the Crowe-Davis and McIvor have been shown LARS Closed frame, expense
Results: The demand for novel TORS retractor systems is being met vertically adjustable blades, instrument attachments
useful in oropharyngeal procedures, and the Dingman
with the evolution of a variety of devices. The goal of these systems Medrobotics Flex Designed for TORS, curved frame various blades, blade adjustment in
tor improves base of tongue access. The development and Closed frame, expense
is to improve exposure of the surgical site, while accommodating an
cation of retractor systems has allowed for improved (FRS) multiple planes, integraged suction
endotracheal tube, endoscope, and robotic
zation and access to more distal sites. The use of the FK, and effector arms. Standard
mouth
difications by Drs.gags such asand
Weinstein theO’Malley
Crowe-Davis and McIvor have been shown
(FK-WO),
to be useful
tionized TORS. in oropharyngeal
The recent developmentprocedures, and the Dingman
of the LARS retractor
Figure 1: Crowe-Davis (left) and McIvor retractor (right)
systems with different sized tongue blades
Figure 2A: Dingman retractor system with different
sized tongue blades.
Figure 2B: Dingman retractor in
situ
Figure 3. FK-WO retractor system with blades
available for exposure of different areas.
retractor
yngeal surgery andimproves base of tongue
the Flex retractor access.
system with The development and
its fine
e blades modification
and retractionofhave
retractor
made systems
TORS an has allowed for improved
increasingly
option for a variety of head and neck procedures.sites.
visualization and access to more distal Theof
Pictures use of the FK, and
its modifications
ystem both by Drs.
on-table and in-situ Weinstein
were and O’Malley (FK-WO),
obtained. Figure 3. FK-WO retractor system with b
Figure 1: Crowe-Davis (left) and McIvor retractor (right) Figure 2A: Dingman retractor system with different Figure 2B: Dingman retractor in
revolutionized TORS. The recent development of the LARS retractor systems with different sized tongue blades sized tongue blades. situ available for exposure of different areas.
usion: Wefor laryngeal
provide surgery
a review and
of the the Flexretractor
available retractorsystems
system with its fine
tunable
TORS surgeon, asblades
well asand retraction
in-situ have
images of made
these TORS an increasingly Figure 4A: LARS retractor system with blades
systems. Figure 4B: LARS retractor in Figure 5A: Flex retractor system with blades available Figure 5B: Flex retractor in situ.
viable option for a variety of head and neck procedures. Pictures of available for exposure of different areas. situ. for exposure of different areas.
each system both on-table and in-situ were obtained.
Conclusion: We provide a review of the available retractor systems
to the TORS surgeon, as well as in-situ images of these systems. Figure 4A: LARS retractor system with blades Figure 4B: LARS retractor in Figure 5A: Flex retractor system with blades available Figure 5B: Flex retractor in situ.
available for exposure of different areas. situ. for exposure of different areas.NUOVE PROSPETTIVE
The Laryngoscope
C 2016 The American Laryngological,
V
Rhinological and Otological Society, Inc.
Transoral Robotic Surgery in the Seated Position: Rethinking Our
Operative Approach
Eric J. Moore, MD; Kathryn M. Van Abel, MD; Kerry D. Olsen, MD
Objectives/Hypothesis: Transoral surgery (TOS) is commonly performed in a supine patient with an oral retractor. Par-
adoxically, this strategy can create difficulty with visualizing and accessing pathology at the base of tongue, inferior pharynx,
and larynx. We investigate the feasibility of TOS with the patient in the seated position.
Pensando di sfruttare la gravità come punto a favore, Moore decide di operare,
Study Design: Pilot study.
Methods: TOS utilizing the da Vinci Robotic Surgical Xi and Si systems (Intuitive Surgical, Sunnyvale, CA) was performed
on a fresh cadaver placed in both the traditional supine position and the seated position. Transoral robotic surgery (TORS) in
dapprima su cadavere, dopo di che sperimentando la medesima tecnica in vivo,
the seated position was then performed on two patients for a supraglottic laryngectomy and a hypopharyngeal carcinoma
resection.
Results: Visualization of the entire upper aerodigestive tract was possible in the cadaver and two patients in the seated
position. The Si was superior for docking, instrumentation, and assistant access. The minimum operating table height is criti-
su due pazienti affetti da tumore squamo cellulare della laringe, in posizione
cal for successful access. Advantages of this position included increased posterior airway/operative space by approximately 2
cm, ability to manipulate the surgical field (nonrigid retraction), and improved visualization. Surgical procedures were com-
pleted in comparable times compared with standard TORS procedures. There were no complications related to seated TORS.
seduta, proprio quella usata da ortopedici o neurochirurghi.
Conclusions: TORS in the seated position was both safe and effective in this pilot study. It allows the surgeon to opti-
mally operate in the inferior pharynx and larynx without the limitation of line of site access and visualization. A paradigm
shift in patient positioning during TOS may allow improved surgical access and even greater patient candidacy. Further clini-
cal investigation into this technique is warranted.
Key Words: Transoral robotic surgery, transoral surgery, oropharyngeal cancer, base of tongue cancer, larynx cancer,
pharynx cancer, seated surgery, supraglottis, hypopharynx.
Level of Evidence: NA
Laryngoscope, 00:000–000, 2016
INTRODUCTION retrognathia, macroglossia, narrow mandibular width, orNella posizione supina tradizionale infatti, la lingua e quindi il baselingua
tendono a cadere verso la parete posteriore dell’orofaringe, obliterando di
fatto la visualizzazione della parte inferiore del baselingua, la faringe
inferiore e la laringe (fatto reso evidente dall’endoscopia nasale performata
su cadavere proprio per dimostrare questa
situazione anatomica). Ancora, Moore
ribadisce questo aspetto, affermando che
anche con la retrazione anteriore della lingua,
nella posizione supina, la baselingua rimane
approssimativa all’epiglottide e quest’ultima
va a poggiare sulla parete posteriore del
faringe. Posizionando il paziente in seduta,
l’esposizione invece migliorava
considerevolmente.ALLA FINE SI TRATTA SOLO DI FORZA DI
GRAVITÀ…
Nella posizione supina i tessuti molli sopraglottici (nel cerchio blu) sono
perpendicolari rispetto al vettore e quindi la forza di gravità li porta a collassare
sulla parete posteriore, mentre nella posizione seduta, tale forza agisce
parallelamente, non perturbando quindi la normale anatomia.LA NOSTRA ESPERIENZA CON LA SEATING POSITION
Per poter performare la posizione seduta, le braccia del Da Vinci® devono essere disposte attorno alla testa del paziente
OLTRE ERIC J. MOORE? Posizione prona, come quella utilizzata dai neurochirurghi nella chirurgia del midollo spinale.
OLTRE ERIC J. MOORE? Posizione laterale, come quella utilizzata dai pazienti operati in chirurgia toracica toracoscopica.
GRAZIE PER L’ATTENZIONE
Puoi anche leggere